
2022
Oregon Death
with Dignity Act
2022 Data Summary
PUBLIC HEALTH DIVISION

2
Acknowledgments
Report written by: Public Health Division, Center for Health Statistics
Date: March 8, 2023
For more information, see: http://www.healthoregon.org/dwd.
Contact: [email protected]
Oregon Death with Dignity Act |Acknowledgments

3
Executive summary
The Oregon Death with Dignity Act (DWDA) allows terminally ill patients who
meet specific qualifications to end their lives through voluntary self-administration
of a lethal dose of medications prescribed by a physician for that purpose. The Act
requires the Oregon Health Authority (OHA) to collect information about the
patients and physicians who participate in the Act and to publish an annual
statistical report.
In 2022, 431 people were reported to have received prescriptions under the
DWDA. As of January 20, 2023, 278 people had died in 2022 from ingesting the
prescribed medications, including 32 who had received prescriptions in previous
years. Demographic characteristics of DWDA patients were similar to those of
previous years: most patients were age 65 years or older (85%) and white (96%). The
most common diagnosis was cancer (64%), followed by heart disease (12%) and
neurological disease (10%). OHA made no referrals to the Oregon Medical Board
for failure to comply with DWDA reporting requirements.
Oregon Death with Dignity Act | Executive summary

4
Introduction
The Oregon Death with Dignity Act (DWDA) allows terminally ill patients who
meet specific qualifications to end their lives through voluntary self-
administration of a lethal dose of medications prescribed by a physician for that
purpose. The Act requires the Oregon Health Authority (OHA) to collect
information about the patients and physicians who participate in the Act and to
publish an annual statistical report.
The DWDA outlines specific patient requirements to participate. A patient must
be 1) 18 years of age or older, 2) capable of making and communicating health
care decisions to health care practitioners, and 3) diagnosed with a terminal
illness that will lead to death within six months. The attending and consulting
physicians must determine whether a patient meets these requirements and report
that fact to OHA at the time a prescription is written. When OHA identifies any
instance of noncompliance with the statutory requirements, it reports the instance
to the appropriate licensing board.
Data presented in this summary, including the number of people for whom
DWDA prescriptions were written (DWDA prescription recipients) and the
resulting deaths from the ingestion of the medications (DWDA deaths), are based
on required reporting forms and death certificates received by OHA as of January
20, 2023. More information on the reporting process, required forms and annual
reports is available at http://www.healthoregon.org/dwd.
Patient residency requirement
In October 2021, a lawsuit was filed against the State of Oregon in U.S. District
Court for the District of Oregon, alleging that the residency requirement in the
Act violated the Privileges and Immunities Clause and the Dormant Commerce
Clause of the United States Constitution, in part because it bars Oregon health
care providers from providing medical aid in dying to non-resident patients. In a
settlement on March 28, 2022, the State agreed not to enforce the residency
requirement in the Act and to submit a legislative concept that would repeal the
residency requirement in ORS 127.800(11), ORS 127.805(1), ORS 127.815(1)(b),
and ORS 127.860.
In accordance with the settlement, House Bill 2279 was introduced in the 2023
session of the Oregon Legislative Assembly. If the bill becomes law, it will remove
all text in the Act related to the residency requirement for patients receiving
medical aid in dying. No other changes to the text of the Act are proposed in this
bill.
Oregon Death with Dignity Act |Introduction

Information on a patient’s state of residence is not collected during the DWDA
prescription process. Residence and other demographic information are
collected from the death certificate. OHA does not receive death certificates
from other states unless the decedent was an Oregon resident. Therefore, if an
Oregon DWDA patient dies out of state and was not a resident of Oregon,
OHA is unlikely to obtain notice of the death. The out-of-state deaths reported
in Table 1 thus may not represent all DWDA deaths from out-of-state residents
who obtained a DWDA prescription from an Oregon health care provider.
Figure 1: DWDA prescription recipients and deaths*, by year, Oregon, 1998–2022
*As of January 20 , 2023
See Table 2 for detailed information
5
Oregon Death with Dignity Act | Introduction

6
Participation summary and trends
During 2022, 431 people received prescriptions for lethal doses of medications
under the provisions of the Oregon DWDA, compared to 384 reported during
2021 (Figure 1). As of January 20, 2023, OHA had received reports of 278
people who died during 2022 from ingesting the medications prescribed under
the DWDA, an increase from 255 in 2021.
Since the law was passed in 1997, a total of 3,712 people have received
prescriptions under the DWDA and 2,454 people (66%) have died from
ingesting the medications. During 2022, DWDA deaths accounted for an
estimated 0.6% of total deaths in Oregon.*
Figure 2 shows a summary of DWDA prescriptions written and medications
ingested. Of the 431 patients for whom prescriptions were written during 2022,
246 (57%) died from ingesting the medication. An additional 84 (19%) did not
take the medications and later died of other causes.
At the time of reporting, ingestion status was unknown for 101 patients
prescribed DWDA medications in 2022. Of these, 43 patients died but follow-
up information is not yet available. For the remaining 58 patients, both death
and ingestion status are not yet known (Figure 2). In all, 16 patients (6% of
DWDA deaths) outlived their prognosis (i.e., lived more than six months after
their prescription date).
* The percentage of total deaths is calculated using the total number of deaths occurring in Oregon during 2021 (45,028),
the most
recent year for which final death data are available.
Oregon Death with Dignity Act | Participation summary and trends

Figure 2: Summary of DWDA prescriptions written and medications ingested in 2022, as of
January 20, 2023
431 people had prescriptions
written during 2022
32 people with
prescriptions written
in previous years
ingested medication
during 2022
246
ingested
medication
278 died from
ingesting
medication
84
did not ingest
medication
and
subsequently
died
from other causes
101 ingestion status
unknown
43
died,
ingestion
status unknown
58
death and
ingestion
status
unknown
7
Oregon Death with Dignity Act | Participation summary and trends

8
Patient characteristics
Table 1 shows the characteristics and end-of-life care for 2022 DWDA deaths,
updated data for 2021 DWDA deaths, combined data for 1998–2020 DWDA
deaths, and total DWDA deaths. Of the 278 DWDA deaths during 2022, most
patients were aged 65 years or older (85%) and white (96%). The median age at
death was 75 years. Forty-nine percent of patients had at least a bachelor’s
degree.
Patients’ most common underlying illness was cancer (64%), followed by heart
disease (12%) and neurological disease (10%).
Most patients died at home (92%), and most were enrolled in hospice care (91%).
Excluding unknown cases, all patients had some form of health insurance. The
percentage of patients with private insurance declined slightly from 2021 (from
22% to 20%), while patients with Medicare or Medicaid insurance saw a slight
increase (from 78% to 80%).
As in previous years, the three most frequently reported end-of-life concerns
were decreasing ability to participate in activities that made life enjoyable (89%),
loss of autonomy (86%), and loss of dignity (62%).
Oregon Death with Dignity Act | Patient characteristics

DWDA process
A total of 146 physicians wrote 431 prescriptions during 2022 (1–51
prescriptions per physician; 78% of physicians wrote one or two prescriptions).
The number of attending physicians has increased most years (Table 2).
Around half of attending and consulting physicians practiced in the Portland
metropolitan area (53% and 50%, respectively), while fewer than 30% practiced
in the other northwestern counties (Table 3). Three patients were referred for
psychological or psychiatric evaluation. During 2022, OHA referred no
physicians to the Oregon Medical Board for failure to comply with DWDA
reporting requirements.
Since 2020, the DWDA provides an exemption to the statutory waiting periods
for patients expected to live fewer than 15 days after the time of their first oral
request for medication. In 2022, 109 patients (25% of DWDA prescription
recipients) were granted exemptions.
Prescribing physicians were present at time of death for 36 (13%) of the patients
who ingested DWDA medications. Thirty-seven patients (13%) had other health
care providers present, and volunteers were present for 51 deaths (18%). Data
on time from ingestion to death are available for 165 DWDA deaths (59%)
during 2022.* Among those patients, time from ingestion until death ranged
from three minutes to 68 hours, with a median time of 52 minutes (Table 1).
The medications prescribed to DWDA patients (since 2013) are shown in
Figure 3 (see also Table 1). More than 70% of ingestions in 2022 involved the
drug combination DDMAPh, which consists of diazepam, digoxin, morphine
sulfate, amitriptyline, and phenobarbital. The drug combination DDMA,
consisting of diazepam, digoxin, morphine sulfate, and amitriptyline,
accounted for 28% of ingestions. Table 4 shows the duration from ingestion to
death by medication prescribed for all known cases. Median time until death
was somewhat shorter after DDMAPh (42 minutes) than after DDMA (49
minutes). All drug combinations have shown longer median times until death
than the barbiturates secobarbital and pentobarbital, which are no longer
readily available.
*
Includes all reports, not just those from licensed health care providers.
Oregon Death with Dignity Act | DWDA Process
9

Figure 3: Medication used in DWDA ingestions, 2013-2022
10
Oregon Death with Dignity Act | DWDA process
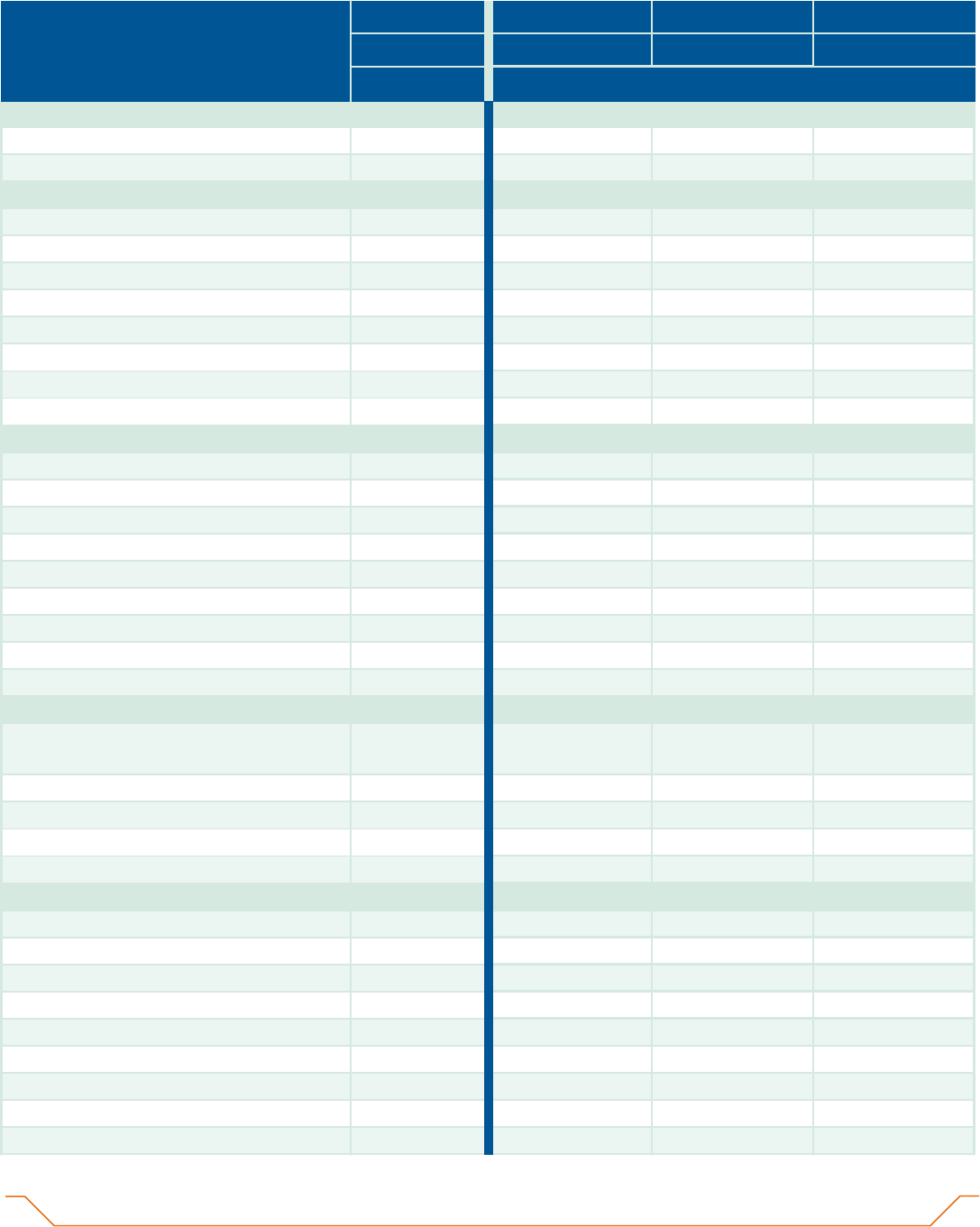
Table 1. Characteristics and end-of-life care of 2,454 DWDA patients who have died
from ingesting a lethal dose of medication as of January 20, 2023, Oregon, 1998-2022
Characteristics
2022 2021 1998-2020 Total
=
(N=278)
=
(N=255)
=
(N=1,921)
=
(N=2,454)
N
(%)
1
N
(%)
1
N
(%)
1
N
(%)
1
Sex
Male
138 (49.6) 140 (54.9) 1,012 (52.7) 1,290 (52.6)
Female
140 (50.4) 115 (45.1) 909 (47.3) 1,164 (47.4)
Age
18-34
1 (0.4) 1 (0.4) 11 (0.6) 13 (0.5)
35-44
3 (1.1) 2 (0.8) 36 (1.9) 41 (1.7)
45-54
12 (4.3) 13 (5.1) 109 (5.7) 134 (5.5)
55-64
27 (9.7) 32 (12.5) 340 (17.7) 399 (16.3)
65-74
90 (32.4) 76 (29.8) 586 (30.5) 752 (30.6)
75-84
91 (32.7) 84 (32.9) 522 (27.2) 697 (28.4)
85+
54 (19.4) 47 (18.4) 317 (16.5) 418 (17.0)
Median years (range)
75 (29-99) 75 (28-101) 72 (25-102) 73 (25-102)
Race and ethnicity
White
267 (96.0) 242 (94.9) 1,849 (96.5) 2,358 (96.3)
African American
1 (0.4) 0 (0.0) 1 (0.1) 2 (0.1)
American Indian
2 (0.7) 1 (0.4) 3 (0.2) 6 (0.2)
Asian
5 (1.8) 6 (2.4) 26 (1.4) 37 (1.5)
Pacific Islander
0 (0.0) 0 (0.0) 1 (0.1) 1 (0.0)
Other
0 (0.0) 0 (0.0) 6 (0.3) 6 (0.2)
Two or more races
1 (0.4) 0 (0.0) 8 (0.4)
9 (0.4)
Hispanic (any race)
2 (0.7) 6 (2.4) 22 (1.1) 30 (1.2)
Unknown
0 0 5 5
Marital status
Married (including Registered Domestic
129 (46.7) 116 (45.8) 881 (46.1) 1,126 (46.1)
Partner)
Widowed
46 (16.7) 51 (20.2) 423 (22.1) 520 (21.3)
Never married
22 (8.0) 22 (8.7) 158 (8.3) 202 (8.3)
Divorced
79 (28.6) 64 (25.3) 450 (23.5) 593 (24.3)
Unknown
2 2 9 13
Education
8th grade or less
5 (1.8) 1 (0.4) 23 (1.2) 29 (1.2)
9th-12th grade, no diploma
8 (2.9) 7 (2.8) 79 (4.1) 94 (3.9)
High school graduate/GED
59 (21.3) 61 (24.2) 407 (21.4) 527 (21.7)
Some college
51 (18.4) 51 (20.2) 387 (20.3) 489 (20.1)
Associate degree
18 (6.5) 15 (6.0) 175 (9.2) 208 (8.5)
Bachelor's degree
61 (22.0) 62 (24.6) 460 (24.1) 583 (24.0)
Master's degree
58 (20.9) 35 (13.9) 232 (12.2) 325 (13.4)
Doctorate or professional degree
17 (6.1) 20 (7.9) 142 (7.5) 179 (7.4)
Unknown
1 3 16 20
Oregon Death with Dignity Act | Table 1
11

12
Oregon Death with Dignity Act | Table 1
Characteristics
2022 2021 1998-2020 Total
=
(N=278)
=
(N=255)
=
(N=1,921)
=
(N=2,454)
N
(%)
1
N
(%)
1
N
(%)
1
N
(%)
1
Residence county / region
2
Clackamas
21 (7.6) 21 (8.2) 192 (10.1) 234 (9.6)
Deschutes
17 (6.1) 27 (10.6) 85 (4.5) 129 (5.3)
Jackson
17 (6.1) 12 (4.7) 133 (7.0) 162 (6.6)
Lane
32 (11.5) 26 (10.2) 207 (10.8) 265 (10.8)
Marion
23 (8.3) 13 (5.1) 185 (9.7) 221 (9.0)
Multnomah
72 (25.9) 58 (22.7) 414 (21.7) 544 (22.3)
Washington
33 (11.9) 21 (8.2) 193 (10.1) 247 (10.1)
Other northwest counties
31 (11.2) 48 (18.8) 293 (15.3) 372 (15.2)
Southern Oregon
18 (6.5) 19 (7.5) 144 (7.5) 181 (7.4)
Central Oregon / Columbia Gorge
8 (2.9) 6 (2.4) 31 (1.6) 45 (1.8)
Eastern Oregon
3 (1.1) 4 (1.6) 33 (1.7) 40 (1.6)
Out of state
3 (1.1) 0 (0.0) 0 (0.0) 3 (0.1)
Unknown
0 0 11 11
End-of-life care
Hospice
Enrolled
254 (91.4) 248 (97.3)
1,713
(90.8)
2,215
(91.5)
Not enrolled
24 (8.6) 7 (2.7) 174 (9.2) 205 (8.5)
Unknown
0 0 34 34
Insurance
Private
43 (20.5) 41 (21.9) 768 (44.5) 852 (40.2)
Medicare, Medicaid or Other Govt.
167 (79.5) 145 (77.5) 938 (54.4)
1,250
(58.9)
None
0 (0.0) 1 (0.5) 18 (1.0) 19 (0.9)
Unknown
68 68 197 333
Underlying illness
Cancer
178 (64.0) 158 (62.0)
1,420
(73.9)
1,756
(71.6)
Lip, oral cavity, and pharynx
6 (2.2) 3 (1.2) 41 (2.1) 50 (2.0)
Digestive organs
45 (16.2) 36 (14.1) 378 (19.7) 459 (18.7)
Pancreas
16 (5.8) 9 (3.5) 125 (6.5) 150 (6.1)
Colon
5 (1.8) 8 (3.1) 98 (5.1) 111 (4.5)
Other digestive organs
24 (8.6) 19 (7.5) 155 (8.1) 198 (8.1)
Respiratory and intrathoracic organs
32 (11.5) 24 (9.4) 303 (15.8) 359 (14.6)
Lung and bronchus
31 (11.2) 23 (9.0) 284 (14.8) 338 (13.8)
Other respiratory and intrathoracic
1 (0.4) 1 (0.4) 19 (1.0) 21 (0.9)
organs
Melanoma and other skin
0 (0.0) 5 (2.0) 44 (2.3) 49 (2.0)
Mesothelial and soft tissue
7 (2.5) 6 (2.4) 34 (1.8) 47 (1.9)
Breast
13 (4.7) 12 (4.7) 129 (6.7) 154 (6.3)
Female genital organs
17 (6.1) 15 (5.9) 106 (5.5) 138 (5.6)
Prostate
14 (5.0) 16 (6.3) 89 (4.6) 119 (4.8)
Urinary tract
6 (2.2) 9 (3.5) 54 (2.8) 69 (2.8)

= = = =Characteristics
2022 2021 1998-2020 Total
(N=278) (N=255) (N=1,921) (N=2,454)
N
(%)
1
N
(%)
1
N
(%)
1
N
(%)
1
-Cancer, continued-
Eye, brain, central nervous system
14 (5.0) 5 (2.0) 59 (3.1) 78 (3.2)
Brain
14 (5.0) 5 (2.0) 53 (2.8) 72 (2.9)
Eye and central nervous system
0 (0.0) 0 (0.0) 6 (0.3) 6 (0.2)
Thyroid and other endocrine
0 (0.0) 1 (0.4) 7 (0.4) 8 (0.3)
Ill-defined, secondary, and unspecified
sites
8 (2.9) 6 (2.4) 50 (2.6) 64 (2.6)
Lymphoma and leukemia
9 (3.2) 16 (6.3) 86 (4.5) 111 (4.5)
Other cancers
7 (2.5) 4 (1.6) 40 (2.1) 51 (2.1)
Neurological disease
27 (9.7) 35 (13.7) 207 (10.8) 269 (11.0)
Amyotrophic lateral sclerosis
15 (5.4) 22 (8.6) 146 (7.6) 183 (7.5)
Other neurological diseases
12 (4.3) 13 (5.1) 61 (3.2) 86 (3.5)
Heart/circulatory disease
32 (11.5) 29 (11.4) 105 (5.5) 166 (6.8)
Respiratory disease [e.g., COPD]
27 (9.7) 19 (7.5) 109 (5.7) 155 (6.3)
Endocrine/metabolic disease [e.g.,
diabetes]
4 (1.4) 5 (2.0) 19 (1.0) 28 (1.1)
Gastrointestinal disease [e.g., liver
disease]
4 (1.4) 3 (1.2) 17 (0.9) 24 (1.0)
Infectious disease [e.g., HIV/AIDS]
2 (0.7) 0 (0.0) 14 (0.7) 16 (0.7)
Other illnesses
4 (1.4) 6 (2.4) 30 (1.6) 40 (1.6)
DWDA process
Outlived 6-month prognosis
16 (5.8) 11 (4.3) 77 (4.0) 104 (4.2)
Referred for psychiatric evaluation
3 (1.1) 2 (0.8) 69 (3.6) 74 (3.0)
Patient informed family of decision
3
257 (95.5) 238 (95.6)
1,731
(95.9)
2,226
(95.8)
Patien
t died at
Home (patient, family or friend)
255 (91.7) 240 (94.1)
1,773
(92.6)
2,268
(92.6)
Assis
ted living or foster care facility
18 (6.5) 13 (5.1) 92 (4.8) 123 (5.0)
Nursing home
0 (0.0) 2 (0.8) 18 (0.9) 20 (0.8)
Hospital
1 (0.4) 0 (0.0) 4 (0.2) 5 (0.2)
Hospice facility
1 (0.4) 0 (0.0) 3 (0.2) 4 (0.2)
Ot
her
3 (1.1) 0 (0.0) 25 (1.3) 28 (1.1)
Unknown
0 0 6 6
4
Lethal medication
DDMAPh
199 (71.6) 99 (38.8) 8 (0.4) 306 (12.5)
DDMA
77 (27.7) 145 (56.9) 315 (16.4) 537 (21.9)
DDMP-2
1 (0.4) 8 (3.1) 194 (10.1) 203 (8.3)
DDMP-1
0 (0.0) 1 (0.4) 71 (3.7) 72 (2.9)
Secobarbital
1 (0.4) 0 (0.0) 860 (44.8) 861 (35.1)
Pentobarbital
0 (0.0) 0 (0.0) 386 (20.1) 386 (15.7)
Phenobarbital
0 (0.0) 0 (0.0) 65 (3.4) 65 (2.6)
Other
0 (0.0) 2 (0.8) 22 (1.1) 24 (1.0)
Oregon Death with Dignity Act | Table 1
13

14
Oregon Death with Dignity Act | Table 1
Characteristics
2022 2021 1998-2020 Total
=
(N=278)
=
(N=255)
=
(N=1,921)
=
(N=2,454)
(%)
1
(%)
1
N N
(%)
1
N
(%)
1
N
End-of-life concerns
Less able to engage in activities making
life enjoyable
247 (88.8) 233 (91.4) 1,728 (90.0) 2,208 (90.0)
Losing autonomy
240 (86.3) 236 (92.5)
1,740 (90.6) 2,216 (90.3)
L
oss of dignity
6
172 (61.9) 174 (68.2) 1,320 (73.7) 1,666 (71.7)
Burden on family, friends/caregivers
129 (46.4) 136 (53.3) 914 (47.6)
1,179 (48.0)
L
osing control of bodily functions
124 (44.6) 122 (47.8) 831 (43.3)
1,077
(43.9)
I
nadequate pain control, or concern about
it
87 (31.3) 69 (27.1) 530 (27.6) 686 (28.0)
Financial implications of treatment
17 (6.1) 20 (7.8) 88 (4.6) 125 (5.1)
Health care provider present (collected
since 2001)
(N=278) (N=255) (N=1,849) (N=2,382)
When medication was ingested
Prescribing physician
44 (24.4) 47 (28.5) 287 (29.0) 460 (28.2)
Other provider, prescribing physician
not present
30 (16.7) 36 (21.8) 433 (43.8) 581 (35.6)
Volunteer
55 (30.6) 47 (28.5) 102 (10.3) 273 (16.7)
No provider or volunteer
51 (28.3) 35 (21.2) 166 (16.8) 318 (19.5)
Unknown
98 90 861 1
,
049
At time of death
Prescribing physician
36 (12.9) 37 (14.5) 265 (14.5) 338 (14.3)
Other provider, prescribing physician
not present
37 (13.3) 42 (16.5) 439 (24.0) 518 (22.0)
Volunteer
51 (18.3) 44
(17.3) 111 (6.1) 206 (8.7)
No provider or volunteer
154 (55.4) 132 (51.8)
1,011 (55.4) 1,297 (55.0)
Unknown
0 0 23 23
7
Complications
(N=278) (N=255) (N=1,921) (N=2,454)
Difficulty ingesting/regurgitated
5 5 33 43
Seizures
0 0 3 3
Other
1 1 16 18
None
66 71 777 914
Unknown
206 178 1,092 1,476
Other outcomes
Regained consciousness after ingesting
DWDA medications
0 1 8 9
Timing of DWDA event
Duration (weeks) of patient-physician
relationship
Median 5 5 12 10
Range
0 - 1083 0 - 940 0 - 2138 0 - 2138
Patients with information available
276 253 1,903 2,432
Patients with information unknown
2 2 18 22
5

l
= = = =
Characteristics
2022 2021 1998-2020 Total
(N=278) (N=255) (N=1,921) (N=2,454)
N
(%)
1
N
(%)
1
N
(%)
1
N
(%)
1
Duration (days) between first request and
death
Median
30 30 45 41
1 - 1859 1 - 1095 1 - 1503 0 - 1859
Patie
nts with information available
278 255 1,919 2,452
Patients with information unknown
0 0 2 2
Duration (minutes) between ingestion and
unconsciousness
Median 5 5 5 5
Range
1 - 300 1 - 45 1 - 240 1 - 300
Patients with information available
150 149 1,005 1,304
Patients with information unknown
128 106 916 1,150
Duration between ingestion and death
Median (minutes)
52 33 30 30
Range
3 min - 68 hrs 2 min - 24 hrs 1 min - 104 hrs 1 min - 104 hrs
Patients with information available
165 158 1,043 1,366
Patients with information unknown
113 97 878 1,088
N indicates the number of patients.
1 Unknowns are excluded when calculating percentages.
2 Other northwest counties: Benton, Clatsop, Columbia, Lincoln, Linn, Polk, Tillamook, and Yamhill.
Southern: Coos, Curry, Douglas, Josephine, Klamath, and Lake.
Central/Columbia Gorge: Crook, Gilliam, Hood River, Jefferson, Sherman, Wasco, and Wheeler.
Eastern: Baker, Grant, Harney, Malheur, Morrow, Umatilla, Union, and Wallowa.
3 First recorded in 2001. Since then, 97 patients (4.1%) have chosen not to inform their families, and 42
patients (1.8%) have had no family to inform. Information is unknown for 19 patients.
4 DDMAPh is a combination of diazepam, digoxin, morphine sulfate, amitriptyline, and phenobarbital.
DDMA is a combination of diazepam, digoxin, morphine sulfate, and amitriptyline.
DDMP is a combination of diazepam, digoxin, morphine sulfate, and propranolol. DDMP-1 contains 10g
of morphine sulfate; DDMP-2 contains 15g.
Phenobarbital is dispensed as a combination of phenobarbital, chloral hydrate, and morphine sulfate.
5 Affirmative answers only (“Don’t know” included in negative answers). Categories are not mutually exclusive.
6 First asked in 2003. Data available for 2,325 patients.
7 Information about complications is reported only when a physician or another health care provider is present at
time of death. Due to the high number of unknowns for this item, percentages are not calculated.
15
Oregon Death with Dignity Act | Table 1
Range

Table 2. Number of DWDA prescription recipients, DWDA deaths, and
attending physicians, 1998-2022
Year
Prescription
recipients
DWDA deaths
Attending
physicians
1998 24 16 n/a
1999 33 27 n/a
2000 39 27 22
2001 44 21 33
2002 58 38 33
2003 68 42 42
2004 60 37 40
2005 65 38 40
2006 65 46 41
2007 85 49 46
2008 88 60 60
2009 95 59 64
2010 97 65 59
2011 114 71 62
2012 116 85 62
2013 121 73 62
2014 155 105 83
2015 218 135 106
2016 204 139 101
2017 218 158 92
2018 261 178 108
2019 296 193 113
2020 373 259 142
2021 384 255 132
2022 431 278 146
Total 3,712 2,454
Oregon Death with Dignity Act | Table 2
16
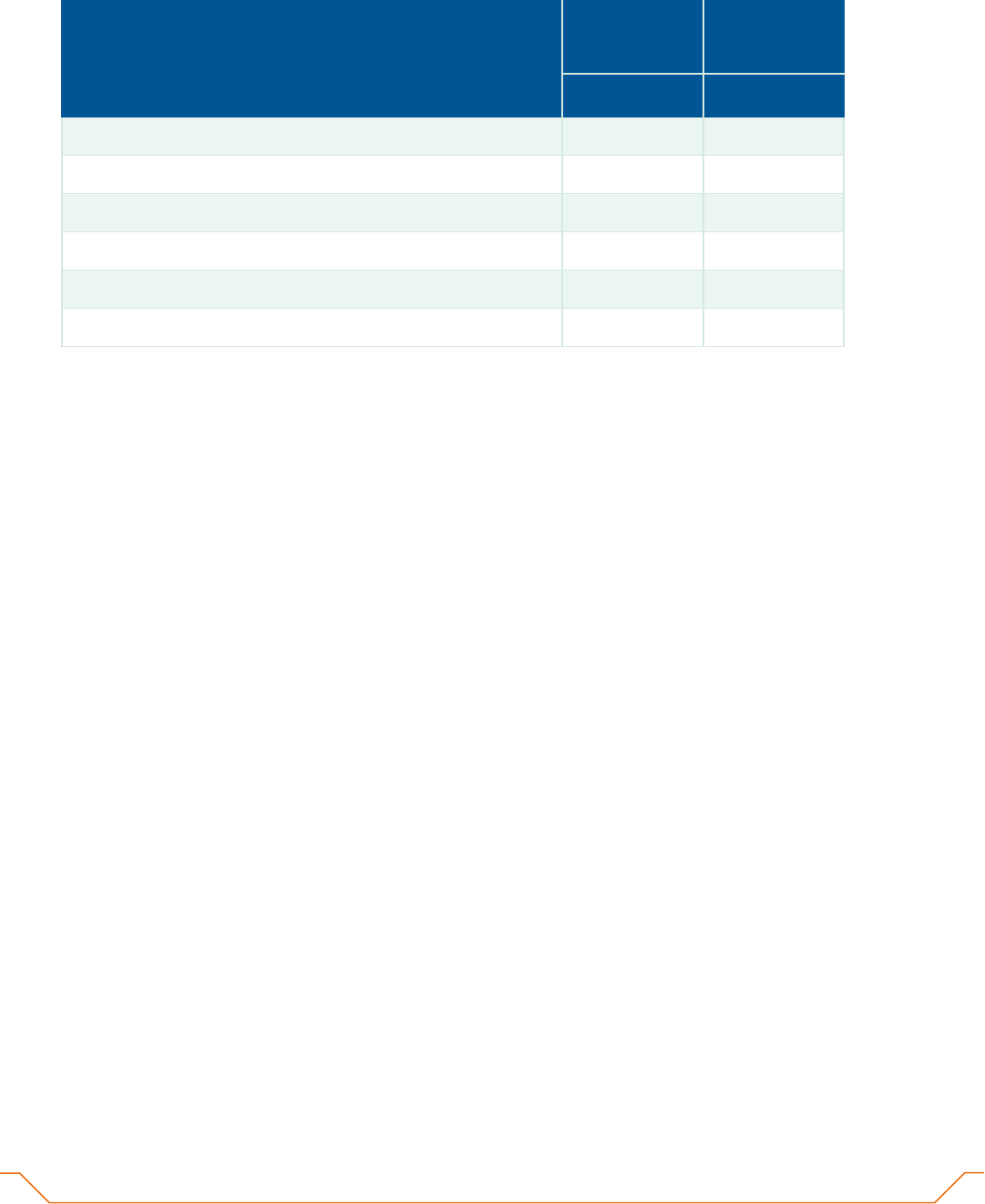
Table 3. Primary location of practice, DWDA physicians, 2022
2
Region
Attending
physicians
Consulting
physicians
N
(%)
1
N
(%)
1
Metro counties (Clackamas, Multnomah, Washington)
78 (53.4) 112 (50.2)
Northwest Oregon (excludes Metro counties)
38 (26.0) 60 (26.9)
Southern Oregon
21 (14.4) 35 (15.7)
Central Oregon / Columbia Gorge
9 (6.2) 16 (7.2)
Eastern Oregon
0 (0.0) 0 (0.0)
Unknown
0 1
1 Unknowns are excluded when calculating percentages.
2 Northwest
Oregon: Benton, Clatsop, Columbia, Lane, Lincoln, Linn, Marion, Polk, Tillamook, and Yamhill.
Southern Oregon: Coos, Curry, Douglas, Jackson, Josephine, Klamath, and Lake.
Central / Columbia Gorge: Crook, Deschutes, Gilliam, Hood River, Jefferson, Sherman, Wasco and Wheeler.
Eastern Oregon: Baker, Grant, Harney, Malheur, Morrow, Umatilla, Union and, Wallowa.
17
Oregon Death with Dignity Act | Table 3

-
Table 4. Duration between ingestion and death, DWDA deaths, 2001-2022
1 Secobarbital has been unavailable for DWDA use since 2019; penobarbital since 2015.
2 DDMA is a combination of diazepam, digoxin, morphine sulfate, and amitriptyline.
3 DDMAPh is a combination of diazepam, digoxin, morphine sulfate, amitriptyline, and phenobarbital.
4 DDMP is a combination of diazepam, digoxin, morphine sulfate, and propranolol. DDMP-1 contains 10g of morphine sulfate; DDMP-2 contains 15 g.
5 Phenobarbital is dispensed as a combination of phenobarbital, chloral hydrate, and morphine sulfate.
6 Patients who regained consciousness after ingestion are not considered DWDA deaths, and are not included in the other columns in this table.
NOTE: Table includes all reported durations, not just those from licensed providers. Complete information not available before 2001. Unknown values are
excluded when calculating percentages.
Oregon Death with Dignity Act | Table 4
18
Drug (%) Total
Unknown
duration
Median
(minutes)
Mean
(minutes)
Range
Regained
consciousness
6
Secobarbital
1
793 403 390 (100.0) 294 (75.4) 69 (17.7) 27 (6.9) 25 137 2 min - 83 hrs 5
DDMA
2
537 201 336 (100.0) 190 (56.5) 140 (41.7) 6 (1.8) 49 78 1 min - 19 hrs 1
Pentobarbital
1
384 156 228 (100.0) 188 (82.5) 31 (13.6) 9 (3.9) 20 97 1 min - 104 hrs 0
DDMAPh
3
306 124 182 (100.0) 110 (60.4) 64 (35.2) 8 (4.4) 42 105 5 min - 68 hrs 0
DDMP-2
4
203 98 105 (100.0) 46 (43.8) 36 (34.3) 23 (21.9) 85 254 2 min - 47 hrs 2
DDMP-1
4
72 47 25 (100.0) 12 (48.0) 7 (28.0) 6 (24.0) 77 223 10 min - 21 hrs 0
Phenobarbital
5
65 43 22 (100.0) 4 (18.2) 13 (59.1) 5 (22.7) 73 439 20 min - 72 hrs 0
Other
24 6 18 (100.0) 7 (38.9) 8 (44.4) 3 (16.7) 71 237 10 min - 24 hrs 1
TOTAL
2,384 1,078 1,306 (100.0) 851 (65.2) 368 (28.2) 87 (6.7) 30 129
1 min - 104 hrs
9
Known duration <1 hour 1-6 hours >6 hours

