
Inside
Science Series
Introduction to the
Nervous System, Part 2
Commonplaces
A Little Black Book of
Texts for Teaching
Medical Writing
Around the
Career Block
Growth of Performance
Improvement CME Presents
Challenges, Opportunities
for Medical Writers
2014 AMWA
Annual Conference
Shake, Rattle, and Write
in Memphis
Practical Matters
Soft Skills: The Critical
Accompaniment to
Technical Skills
Volume 29 Number 2 / Summer 2014
THE OFFICIAL JOURNAL OF THE
AMERICAN MEDICAL WRITERS ASSOCIATION,
THE RESOURCE FOR MEDICAL COMMUNICATORS
WWW.AMWA.ORG
The AMWA Annual Conference is the ultimate resource for
medical communicators around the world, offering educational
and networking opportunities beyond compare in the field.
JOIN US
www.amwa.org/events_annual_conference
Registration opens in early July.
Early bird registration rates
available through August 30.
ELECTRONIC EDITION

Join the Discussions
www.amwa.org/forum.asp
in the
AMWA Online
Community
Forums
Ask a question
Share a resource
Connect with peers
❯❯
➔
Order at amwa.org
Member discount on Self-Study Modules.
On sale now: Basic Grammar and Usage ($150.00)
and Sentence Structure and Patterns ($125.00)
Sale date extended through: July 31, 2014.
On sale now:
Basic Grammar and Usage:
Original Price $199; Sale Price $150
Sentence Structure and Patterns:
Original Price $159; Sale Price $125
Sale extended through July 31, 2014
AMWA
SELFSTUDY
MODULES
Order at amwa.org
Learn at your own pace
Basic Grammar
and Usage
Flo Witte, PhD, ELS
An Essential Skills Workshop of the
American Medical Writers Association
Flo Witte, PhD, ELS
Sentence Structure
and Patterns
An Essential Skills Workshop of the
American Medical Writers Association

SCIENCE SERIES
Introduction to the Nervous System, Part 2: The Autonomic
Nervous System and the Central Nervous System
� Agnella Izzo Matic
COMMONPLACES
My Little Black Book of Texts for Teaching Medical Writing
� Lora Arduser
AROUND THE CAREER BLOCK
Not for the Fainthearted: Growth of Performance
Improvement CME Presents Challenges, Opportunities for
Medical Writers
� Don Harting
2014 AMWA ANNUAL CONFERENCE PREVIEW
Shake, Rattle, and Write in Memphis � Lori Alexander
2014 SWANBERG AWARD
� J. Patrick Barron
PRACTICAL MATTERS
Soft Skills: The Critical Accompaniment to
Technical Skills
� Kelleen Flaherty
MELNICK ON WRITING
Spice Up Your Lead: Get the Lead Out � Arnold Melnick
FREELANCE FORUM
� Brian Bass, Lori De Milto, Debra Gordon, and Elizabeth L. Smith
How Do You Keep Track of Business Expenses for
Tax Purposes?
Tips for Tracking Time
Tips for Creating Job Numbers
SOCIAL MEDIA
Five Social Media Gurus to Follow � Cynthia L. Kryder
TECH TALK
Password Management: Staying Safe and Sane
� Laura Mizoue
Tech Notes: Wired Magazine Study
� Jeanne McAdara-Berkowitz
Contents
V29 N2
SUMMER
2014
51
56
62
66
69
70
73
74
76
78
76
84
66

Contents
EDITOR Victoria J. White, MA, ELS
EDITORIAL BOARD Peggy Boe, RN
Tracey Fine, MS, ELS
Randall Fritz, DVM, ELS
Douglas Haneline, PhD
Cynthia L. Kryder, MS, CCC-Sp
Peggy Robinson, ELS
Barbara Snyder, MA
Deb Whippen
SECTION EDITORS
Around the Career Block Hilary Graham, MA
Commonplaces Lora Arduser, PhD
Conference Coverage Amy Karon, DVM, MPH, MA
Find Michelle A. Kraft, MLS, AHIP
Media Reviews Evelyn B. Kelly, PhD
Practical Matters Julie Ravo
Regulatory Insights Peggy Boe, RN
Jennifer Grodberg, PhD, RAC (US)
Science Series Randall Fritz, DVM, ELS
Social Media Cynthia L. Kryder, MS, CCC-Sp
Tech Talk Jeanne McAdara-Berkowitz, PhD
REGULAR CONTRIBUTORS
Freelance Forum Brian Bass
Melissa L. Bogen, ELS
Sherri Bowen, MA, ELS
Lori De Milto, MJ
Cathryn Evans
Debra Gordon, MS
Donna Miceli
Phyllis Minick
Elizabeth L. Smith
In the Service of Good Writing Laurie Endicott Thomas, MA, ELS
Melnick on Writing Arnold Melnick, DO
EDITOR EMERITUS Lori Alexander, MTPW, ELS
EDITOR IN MEMORIAM Ronald J. Sanchez
2013–2014 PRESIDENT Brian Bass
EXECUTIVE DIRECTOR Susan Krug, CAE
GRAPHIC DESIGNER Amy Boches, biographics
ADVERTISING: Contact Tima Good at [email protected]; (717) 505-9701,
ext 127. All advertising is subject to acceptance by AMWA and should be for
products and services relevant to professional medical communicators. AMWA is not
responsible for the content of advertising and does not endorse any advertiser or its
products or services.
SUBSCRIPTION: The AMWA Journal is published quarterly. Subscription is included
with AMWA membership. Nonmember subscriptions cost is $75 per year.
CONTACT: American Medical Writers Association, 30 West Gude Drive, #525,
Rockville, MD 20850-4347. Phone: (240) 238-0940; Fax: (301) 294-9006;
E-mail: [email protected].
AMWA Journal is in the MLA International Bibliography and selectively indexed in
the Cumulative Index to Nursing and Allied Health Literature (CINAHL) print index,
the CINAHL database, and the Cumulative Index of Journals in Education (CIJE).
The opinions expressed by authors contributing to the Journal do not necessarily
reect the opinions of AMWA or the institutions with which the authors are
aliated. The association accepts no responsibility for the opinions expressed by
contributors to the Journal.
©2014, American Medical Writers Association. All rights reserved, worldwide.
ISSN 1075-6361
AMWA JOURNAL MISSION STATEMENT
The AMWA Journal expresses the interests, concerns, and
expertise of members. Its purpose is to inspire, motivate,
inform, and educate them. The Journal furthers dialog
among all members and communicates the purposes,
goals, advantages, and benets of the American Medical
Writers Association as a professional organization.
80 FIND
Making the Most of Google Scholar � Michelle A. Kraft
83 CALENDAR OF MEETINGS
84 SOUNDING BOARD
My Philosophy of Editing: Pruning and Nurturing
to Help Manuscripts Bloom
� Mary E. Knatterud
86 IN THE SERVICE OF GOOD WRITING
Colorless Green Ideas Sleep Furiously
� Laurie Endicott Thomas
88 MEDIA REVIEWS
Review of How the NIH Can Help You Get Funded. An
Insider's Guide to Grant Strategy
� Karen Potvin Klein
89 AMWA NEWS
Your AMWA at Work � Brian Bass
Slate of Candidates for 2014-2015 Election
Annual Financial Report, 2012-2013
� Christine F. Wogan
Quarterly Update on Certication
� Thomas Gegeny and Marianne Mallia
In Memoriam: Joseph H. Bloom
� Barbara C. Good
96 INSTRUCTIONS FOR CONTRIBUTORS
MORE
V29 N2 / 2014
Cover image courtesy of the National Institute on Aging, National
Institutes of Health, Department of Health and Human Services.
AMWA Journal / V29 N2 / 2014 / amwa.org 51
ABSTRACT
An overview of the healthy human nervous system is pre-
sented, covering some important anatomical and functional
characteristics, as well as clinical applications and diseases of
the nervous system. In the first article of this two-part series,
we discussed the basics of nervous system communication,
sensory nervous systems, and motor neurophysiology. This
article will discuss the autonomic nervous system and the cen-
tral nervous system. Many body functions we are not routinely
aware of are controlled by our autonomic nervous system,
which is composed of the sympathetic system, the parasym-
pathetic system, and the enteric system. The neurons of the
autonomic system innervate gland cells, cardiac muscle,
and smooth muscle to regulate physiologic activities such as
sweating, blood pressure, and heart rate. The central nervous
system acts as the communication hub of the body, interpret-
ing incoming neural signals and, if necessary, dispatching
other neural signals to relevant areas of the body. Within one
functional area of the central nervous system, such as audi-
tory perception, there are several distinct, yet interconnected,
structures that carry out different roles to process the incom-
ing neural signals.
AUTONOMIC NERVOUS SYSTEM
Many body functions we are not routinely aware of are con-
trolled by our autonomic nervous system. The neurons of
the autonomic system innervate gland cells, cardiac muscle,
and smooth muscle to regulate physiologic functions such
as sweating, blood pressure, and heart rate. There are three
divisions of the autonomic nervous system: the sympathetic
system, the parasympathetic system, and the enteric system.
Sensory signals are relayed through autonomic neurons to a
higher processing center in the brain, which interprets the
signals and sends a corresponding neural signal to either
increase or decrease a certain function.
The sympathetic and parasympathetic systems act in
opposition to each other, as will be discussed below. The auto-
nomic nervous system is always functioning, and most of the
time a balance is achieved between the sympathetic and para-
sympathetic divisions regarding their influence on bodily func-
tions. At certain times of the day and for certain functions, one
division will have more influence than the other.
Sympathetic System
The phrase “fight or flight” is often used to summarize the
function of the sympathetic nervous system. Essentially, the
sympathetic nervous system acts to maximize the resources
used by the body when presented with a stressful or threaten-
ing situation. For instance, blood vessels constrict in less criti-
cal organs such as the skin and gastrointestinal tract to make
more blood available in muscles for exertion. The sympathetic
system also increases heart rate and heart contraction force
and relaxes and opens lung airways. At the same time that
these functions increase, less survival-critical functions such as
digestion decrease. Most sympathetic neurons release a neu-
rotransmitter called norepinephrine, which along with its close
relative epinephrine can bind to two types of receptors on
receptor organs: alpha and beta adrenergic receptors.
The neurons that control the sympathetic system arise pri-
marily from the spinal cord and ganglia (masses of neuron cell
bodies) that lie outside of the spinal cord. Many of the func-
tions influenced by the sympathetic system can be activated
individually and in a graded fashion. This is helpful when exer-
cising at the gym, so that your heart rate and breathing rate
increase, but your pupils don’t dilate and the hair on your skin
doesn’t stand on end as if ready for a fight.
By Agnella Izzo Matic, PhD / Principal, AIM Biomedical, Evanston, IL
Introduction to the Nervous System, Part 2:
The Autonomic Nervous System and the
Central Nervous System
SCIENCE SERIES
feature

52 AMWA Journal / V29 N2 / 2014 / amwa.org
Parasympathetic System
The parasympathetic system counterbalances the sympa-
thetic system and puts the body into a “rest and digest” mode
to conserve energy. When the parasympathetic system is exert-
ing influence, there is an increase in salivation and secretion
of digestive enzymes and a decrease in heart rate and airway
diameter. The neurons that transmit information for the
parasympathetic system mostly originate in the brainstem,
although elimination functions are influenced by neurons
that originate in the lowest (sacral) portion of the spinal cord.
Almost all parasympathetic neurons release a neurotransmit-
ter called acetylcholine, which can bind to two types of recep-
tors on the effector organs: muscarinic receptors and nicotinic
receptors.
Humans can voluntarily control some of the parasympa-
thetic impulses that are received, most notably urination and
defecation. In contrast, there is very little voluntary control
over sympathetic impulses. Certain functions are influenced
by the sympathetic system but not by the parasympathetic
system, including sweating, blood vessel dilation, and release
of epinephrine by the adrenal medulla.
Clinical Applications
Many pharmaceuticals act on the autonomic nervous
system, with wide-ranging effects. Albuterol, used to dilate
airways in patients with asthma, binds to beta-adrenergic
receptors found in the sympathetic system. Atenolol, used
to reduce abnormally rapid heart rates, blocks the action
of the sympathetic system at beta-adrenergic receptors.
Pilocarpine, used to treat dry mouth from cancer treat-
ment, as well as glaucoma, binds to muscarinic receptors
in the parasympathetic system. Numerous other agents
have a direct or indirect effect on the autonomic nervous
system. Pharmaceuticals often have side effects that mani-
fest through the autonomic nervous system.
Enteric System
The third and least well-known division of the autonomic
nervous system is the enteric system, which is a local ner-
vous system for the digestive system. Although, as was just
discussed, the digestive system is under sympathetic and
parasympathetic control, the local enteric nervous system is
influential in how food is processed and can act independently
of the sympathetic or parasympathetic system. The enteric
system is composed of various networks of neurons located
within the walls of the digestive tract. The enteric neurons
allow digestive functions to continue without the input of sym-
pathetic or parasympathetic signals. These neurons respond
to changes in the local environment to control gastrointestinal
(GI) motility, fluid retention, electrolyte exchange, and diges-
tive secretions. The enteric system has many connections with
the central nervous system, so that there is local and global
control of the digestive process.
CENTRAL NERVOUS SYSTEM
Think of the central nervous system (CNS) as the communica-
tion hub of the body: Neural signals arrive, are interpreted by
the CNS, and if necessary, other neural signals are dispatched
to relevant areas of the body. Within one functional area of the
CNS, such as auditory perception, several distinct yet inter-
connected structures carry out different roles to process the
incoming neural signals.
Spinal Cord
One of the most important functions of the spinal cord is to
serve as a relay station for neural signals passing between the
brain and peripheral neural structures. However, neural cir-
cuits that terminate in the spinal cord can also execute func-
tions such as normal walking movements and motor reflexes to
withdraw from painful stimuli without the influence of neural
signals from the brain. In cross-section, the organization of the
spinal cord is seen to be preserved throughout its length, with
white matter around the outside and gray matter on the inside.
The cell bodies of neurons make up the gray matter, which
roughly resembles a butterfly in a cross-sectional (horizontal)
view. Within the gray matter, the dorsal (toward the back) horn
of the spinal cord carries the cell bodies of somatosensory neu-
rons (eg, touch, pain) relaying information from the periphery.
The ventral (toward the belly) horn of the spinal cord is com-
posed of motor neurons that send signals out to muscles. The
lateral horn comprises autonomic neurons that connect to
internal organs. Signals enter and exit the spinal cord through
the roots of spinal nerves located between the vertebrae
(Figure 1). The dorsal and ventral roots of the spinal nerves
merge just outside the spine to form a whole spinal nerve that
contains sensory, motor, and autonomic neurons.
The white matter of the spinal cord largely carries the
axons of neurons within the spinal cord and is organized into
columns and tracts based on function. The dorsal columns
carry somatosensory information toward the brain. The lateral
columns contain nerves that transmit signals from the brain
(more specifically, the cortex) to the spinal motor neurons. The
ventral columns carry neural signals in both directions. Pain
and temperature information is carried from the periphery
to the brain; motor information is carried from several brain
structures to the spinal cord motor neurons.

AMWA Journal / V29 N2 / 2014 / amwa.org 53
Clinical Applications
Because the spinal cord contains neurons that control and
coordinate many physiologic functions, an injury to the
spinal cord can affect a variety of systems with a range of
severity. Most spinal cord injuries are caused by a sudden
blow to the spine that breaks the vertebrae. Some inju-
ries can heal completely and some result in permanent
paralysis. Spinal cord injuries are classified by the vertebral
level at which they occur, and this level dictates the likely
impairment(s) that will occur from the injury; for instance,
an injury in the sacral region of the spine will commonly
affect bowel and bladder function.
Brainstem
The brainstem is the physical juncture between the brain
and the spinal cord and is located at the base of the skull.
The brainstem is made up of the medulla, the pons, and the
midbrain, each of which plays a different role in the CNS.
Brainstem functions can be broadly categorized into three
groups: information throughway, cranial nerve functions, and
vital function control. The medulla is the section of the brain-
stem closest to the spinal cord, and it regulates vital physi-
ologic functions such as breathing rate, heart rate, and blood
vessel diameter. The medulla also acts as a crossing point for
many axons passing between the spinal cord and the contralat-
eral (opposite) side of the brain.
The pons is involved in motor control and conscious-
ness level, including sleep. The pons also acts as a major relay
point for information passing between multiple brain centers.
The midbrain serves as a throughway for motor nerve axons
that are traveling from the cerebral cortex to the spinal cord.
The midbrain also contains the superior and inferior colliculi,
which are collections of neurons that play critical roles in the
visual and auditory senses, respectively.
The brainstem also contains the axons and cell bodies of
many head and neck neurons that are involved in sensory and
motor functions. Most of the cranial motor and sensory nerves
enter the brainstem at the pons. These nerves include the
motor nerves that control facial expressions, eye movements,
and chewing. In this sense, the brainstem can be viewed as
an extension of the spinal cord, which houses axons and cell
bodies of sensory and motor neurons originating below the
neck. Because the brainstem plays a critical role in several basic
bodily functions and senses, any trauma to this region, includ-
ing stroke, can be extremely debilitating or life-threatening.
Limbic System
The limbic system has been frequently described as the “emo-
tional brain” because of the large part it plays in originating
and regulating our emotions and behavior. The limbic system
is not as anatomically discrete as other sections of the brain; it
is organized more by functional relationships and neural con-
nections. As a result, reports differ on which structures are
included in the limbic system.
If you imagine the brain as a sphere, the limbic system is
located toward the middle of this sphere. The hypothalamus
(Figure 2) is a very small structure that controls functions such
as body temperature, water regulation, and circadian rhythm.
It can also influence endocrine hormone release from the pitu-
itary gland. The hypothalamus is involved in regulating sexual
satisfaction, fear, and aggression.
The amygdala is another major portion of the limbic
system and is largely a behavior awareness area. It coordinates
behavior and autonomic responses to the external environ-
ment. Early research indicated that the amygdala is involved
with emotional responses to fear and anxiety. More recent
studies have linked the amygdala to attention and a general
ability to define a stimulus and evoke an appropriate response.
The amygdala also helps form memories of emotional events.
The hippocampus is most well-known for its role in learn-
ing and memory, although it also plays a role in understand-
Figure 1. The spinal cord within the vertebral column. Notice the
gray matter in the middle of the spinal cord, which is colored
black and resembles a buttery shape. Surrounding the gray
matter is the white matter, which is primarily composed of
neuron axons. The roots of spinal neurons enter and exit the
spinal cord through openings between adjacent bony vertebrae.
In this image, the ventral (belly) side of the spinal cord is facing
the viewer. The image is courtesy of the National Institute of Arthritis
and Musculoskeletal and Skin Diseases, National Institutes of Health,
Department of Health and Human Services.
Spinal cord
Nerve roots
Vertebra
Intervertebral
disk

54 AMWA Journal / V29 N2 / 2014 / amwa.org
ing the body’s spatial position. The hippocampus consolidates
short-term memories of experienced events into long-term
memories. When a lesion occurs in the hippocampus, a person
can’t form new long-term memories but can usually access
memories that were consolidated before lesion formation. The
hippocampus also aids with spatial memory and navigation,
allowing people to remember where they have been or how to
get somewhere.
Cerebellum
The cerebellum, meaning “little brain,” is a spherical structure
that is estimated to contain 50% of the total neurons in the
brain. The cerebellum plays a major role in coordinating move-
ment, but it cannot initiate motor function by itself. Fast move-
ments, such as running and typing, are smoothly executed
under the control of the cerebellum. The cerebellum influences
the timing of coordinated movements and makes corrections
to monitored motor signals. The cerebellum can do so because
it receives motor information about what should happen and
sensory information about what is happening and compares
the two inputs to see if they agree.
When muscle loads change, the cerebellum compensates
by changing the force of muscle contraction. The cerebellum
also relays information to the motor cortex to plan the next
movement in a sequence so that the movement is smoothly
executed. Motor learning happens in the cerebellum, both
learning new skills and learning from previous movement
errors.
Cerebral cortex
If we go back to our analogy of the brain as a sphere, the
cerebral cortex would correspond to the outer shell covering
the top approximately three-fourths of the sphere. However,
the surface of the cortex is not smooth but rather has folds,
called sulci, in which more than two-thirds of the cortical
surface resides.
The cerebral cortex is often referred to as “gray matter”
because of the gray color of the tissue, which is largely due to
the presence of neuron cell bodies. The functional portion of
the cortex is approximately 2 to 4 mm thick in humans, and
most of it is composed of six morphologically distinct layers
of neurons. The cortex is organized into right and left hemi-
spheres, which are divided by a longitudinal fissure.
The cerebral cortex is often classified by physiologic func-
tion. For instance, there is an auditory cortex responsible for
perceiving sound, a somatosensory cortex responsible for
touch perception, a visual cortex responsible for seeing, and a
motor cortex responsible for executing voluntary movements.
Each cortical section is subdivided. The primary cortical area is
involved in the direct perception of a stimulus or in executing
a movement. The secondary cortical area (or associated area)
is tasked with interpreting the signals delivered to the primary
sensory cortex or, in the case of motor cortex, selecting the vol-
untary movements to execute.
In the somatosensory cortex, body areas that are more sen-
sitive to touch (eg, fingers and lips) compose a larger portion
of the brain than body areas that are less touch sensitive. The
two hemispheres of the somatosensory cortex receive infor-
mation almost exclusively from the opposite side; ie, touch
information from the left hand will be transmitted to the right
somatosensory cortex. Neurons in the visual cortex are highly
activated by high-contrast edges (light-dark) in images, with
Figure 2. A rendering of an adult human brain within the skull.
The image shows a cross-sectional view through the middle of the
brain in the sagittal plane (parallel with the ssure that separates
the right and left hemispheres). Several major anatomical struc-
tures are labeled, including the brainstem, portions of the limbic
system (amygdala, hippocampus), the cerebellum, and the cere-
bral cortex. The image is courtesy of the National Institute on Aging,
National Institutes of Health, Department of Health and Human Services.

AMWA Journal / V29 N2 / 2014 / amwa.org 55
different neuron locations responding preferentially to differ-
ent orientation angles of the edge/bar. Stereo vision aids in
depth perception and is achieved by mixing the input from
both eyes into each hemisphere of the visual cortex.
Similar to the somatosensory and visual cortices, the audi-
tory cortex contains a topographical map corresponding to
different acoustic frequencies at different cortical locations.
Some areas of the auditory cortex are suited to process fre-
quencies found in speech, whereas others are specialized to
extract information about variations in amplitude (loudness)
or timing. The motor cortex receives inputs from the spinal
cord and brainstem on the contralateral side of the body. The
topographical organization of the motor cortex largely mirrors
that of the somatosensory cortex, with a larger representation
for areas with fine movements, such as the hands and face. It
appears that the motor cortex acts to execute one functional
movement by a neural circuit, rather than each area of the
cortex corresponding directly to a single muscle.
In addition to well-defined sensory and motor cortices,
there are many association areas of the cortex that receive and
process information from other cortical and subcortical struc-
tures. The association cortices process complex information,
compare information from different sensory cortices, extract
related information, and plan any necessary responses. For
instance, Wernicke’s area is associated with language compre-
hension, whereas a separate area, Broca’s area, is associated
with speech and language expression. (There are other cortical
areas involved to a lesser degree in language skills.)
Association area functions have been determined mostly
through lesion/deficit studies in humans and animals. The
parietal association cortex is concerned with body awareness
and external stimuli that act on the body. The temporal asso-
ciation cortex aids in facial and complex image recognition
and is thought to participate in long-term memory. The frontal
association cortex, also known as the prefrontal area, is largely
responsible for personality expression and executive functions,
such as judgment, reasoning, and working memory.
Clinical Applications
The cortex is not a static entity, but rather has plasticity,
which is the ability to change and develop in response to
its environment and inputs. The cortex can be modified in
response to a change in sensory or motor system inputs
(increase or decrease). For instance, when a lesion on the
retina causes focal vision loss, the corresponding location
on the topographic visual cortex map will regain function
with inputs from areas neighboring the retinal lesion. Similar
changes to lesions have been seen in other sensory cortices.
CONCLUSION
The overview of the nervous system provides a brief look at the
complex communication and regulation that takes place in
humans. Although much is known about neuron function and
sensory systems, there is so much more that research has yet to
uncover.
Author disclosure: The author notes that she has no commercial associ-
ations that may pose a conflict of interest in relation to this article.
Author contact: [email protected]
GLOSSARY
ganglion (pl. ganglia) – Mass of neuron cell bodies.
gray matter – Tissue in the central nervous system that is
mostly composed of cell bodies and is gray
in color.
plasticity – Changes in synapses and neural circuits due
to changes in the neural environment or inputs.
sulcus (pl. sulci) – A fold on the outer surface of the
brain.
white matter – Tissue in the central nervous system that
is mostly composed of myelinated nerve fibers and is
white in color.
RESOURCES
Davis KL, Charney D, Coyle JT, Nemeroff C, eds.
Neuropsychopharmacology – 5th Generation of Progress.
Philadelphia, PA: Lippincott, Williams & Wilkins; 2002.
Guyton AC, Hall JE. Textbook of Medical Physiology. 12th
ed. Philadelphia, PA: W.B. Saunders; 2010.
Kandel ER, Schwartz JH, Jessell TM, Siegelbaum SA,
Hudspeth AJ, eds. Principles of Neural Science. 5th ed.
New York, NY: McGraw-Hill; 2012.
Purves D, Augustine GJ, Fitzpatrick D, et al, eds.
Neuroscience. 5th ed. Sunderland, MA: Sinauer
Associates; 2012.
Speert D, ed. Brain Facts: A Primer on the Brain and
Nervous System. 7th ed. Washington, DC: Society for
Neuroscience; 2012.

I
teach a graduate class in science and medical writing in
the professional writing program at UC. The students
in our graduate degree program come from a variety of
backgrounds. Many of them know they want a career in writ-
ing or editing, but have not pinpointed a specific field in
which they would like to work.
Most of our students go into workplace positions rather
than academic positions. My general goals for the class are to
1) develop their critical analysis skills to inform their writing
skills and 2) hone their writing skills. As such, I designed the
course so the students will learn to:
• Explaintheconventionsofscienticandmedicalwriting
• Producewritinginavarietyofformsspecictoscientic
and medical writing and for specific purposes and
audiences
• Evaluatethedifferencesbetweenonlineandprint
scientific and medical writing
• Analyzepopulardiscourseaboutscienceandhealth
• Deneanddiscussmajorissuesofethicsandhowthey
affect science and health writing
• Becomeadeptatresearchingmedicalandscientic
subjects
• Acquireabasicmedicalandsciencevocabulary
My list is the result of numerous years spent teach-
ing and studying medical communication as well as work-
ing with medical professionals to write and design texts for
patients and the general public. I don’t use all the texts in the
following list in a term; it represents the bank of resources,
my little black book if you will. Here I have divided resources
into the categories of critical analysis and production. This
division highlights how I approach the class: I ask the stu-
dents to critically think about the rhetorical implications of
medical, science, and health writing then to apply these
lessons to the production of such documents. Using princi-
ples from rhetoric, the art of effective or persuasive speaking
My Little Black Book of Texts for
Teaching Medical Writing
By Lora Arduser, PhD / Assistant Professor, Professional Writing, University of Cincinnati, OH
People who teach medical writing in colleges and univer-
sities and practitioners of medical writing share common
interests, knowledge, and practices, but we often lack the
opportunity to exchange ideas and share knowledge. This
new section is designed to be a space for doing just that. We
named the section “Commonplaces,” a word that can refer
to a place where writers collect ideas and information (a
commonplace book is an idea hundreds of years old) and a
community space such as a commons that can be used for
discussion.
Here is how “Commonplaces” will work. Each issue, you
will hear from a teacher/student or practitioner on a par-
ticular topic, and in subsequent issues, similar themes will
be addressed from a different perspective. In this issue, for
example, Lora Arduser, an assistant professor of professional
writing at the University of Cincinnati, will talk about a set
of key texts for students who take medical writing courses. In
upcoming issues, we expect to feature key resources that may
be emphasized in the field. Other topics ahead may include
theories of empowerment and writing, designing shared deci-
sion-making tools; the role of the hospitalist in medical com-
munication; and audience analysis.
Our hope is that the dialogue between academics and
practitioners in these pages will cross what is often charac-
terized as a divide between theory and practice. In so doing,
we can open up the conversation about medical communi-
cation between people working in the industry and people
teaching in academic institutions.
We encourage you to e-mail us (JournalEditor
@amwa.
org) with ideas for upcoming topics and let us know if you
are interested in writing for the section. With your help, we
will try to keep it from being commonplace.
Commonplaces: A New Section of the AMWA Journal
CommonplaCes
56 AMWA Journal / V29 N2 / 2014 / amwa.org

or writing, can help future medical writers become strate-
gic communicators who can produce well-written and well-
designed documents and persuasively engage an audience.
Critical Lens Resources
Accommodating Science: The Rhetorical Life of Scientific
Facts. Journal Article.
Jeanne Fahnestock (1986). Written Communication,
Volume 3, pages 275–296.
Fahnestock investigates genres written for scientific audiences
versus those written for nonscientific audiences.
A Field of Expertise, the Organization, or Science Itself?
Scientists’ Perception of Representing Research in Public
Communication. Journal Article.
Maja Horst (2013) Science Communication, Volume 35,
page 758.
This article looks at the role of scientist as spokesperson, “rep-
resenting science as both ‘speaking on behalf of’ science and
symbolically ‘standing for’ science and its organizations.” The
author draws on literature from the field of organizational
communication, a subfield of communication studies that
analyzes the role of communication in organizational contexts,
to argue that science communication should be considered as
an activity linked with perceptions of identity and organiza-
tional culture.
Forms as Boundary Genres in Medicine, Science, and
Business. Journal Article.
Susan L. Popham (2005). Journal of Business and Technical
Communication, Volume 19, Issue 3, pages 279–303.
Popham’s article analyzes medical treatment forms as genres
to argue that medical forms represent a “commingling of the
business, science, and medical professions in ways that show
evidence of tension and conflict between the disciplines.”
Health and the Rhetoric of Medicine. Book.
Judy Z. Segal (2005). Carbondale: Southern Illinois University
Press.
Segal’s book uses rhetorical theory to investigate the persuasive
elements of clinical and public medical discourse.
Realms of Rhetoric in Health and Medicine. Journal Article.
Colleen Derkatch and Judy Segal (2005). University of Toronto
Medical Journal, Volume 83, pages 138–142.
Derkatch and Segal introduce rhetorical theory into the study
of health and medicine and suggest ways that a rhetorical per-
spective can offer insight into medical research and practice.
The authors argue that an awareness of rhetorical principles in
medicine can provide medical professionals with new perspec-
tives on familiar problems of human interaction in health care
contexts.
Rhetoric of Healthcare: Essays Toward a New Disciplinary
Inquiry. Book.
Barbara Heifferon and Stuart C. Brown, eds. (2008). Creskill,
NJ: Hampton Press.
This collection looks at the role of rhetoric in various health
care and medical discourses and examines what rhetoric can
contribute to the fields of medicine and health.
Women Will Get Cancer: Visual and Verbal Presence in a
Pharmaceutical Advertising Campaign About HPV.
Journal Article.
Jamie Landau (2011). Argumentation and Advocacy, Vol. 48,
pages 39–54.
This article discusses Merck’s 2006 “Tell Someone” direct-to-
consumer advertising campaign, which was created to educate
the public about the link between the human papillomavirus
and cervical cancer. The author uses the concepts of presence
and absence, which are verbal or visual strategies for making
persuasive arguments, to analyze two videos from this cam-
paign that aired across major US television networks.
Writing Resources
Style Guides
AMA Manual of Style: A Guide for Authors and Editors, 10th
Edition. Book.
Iverson C, Christiansen S, Flanagin A, et al. New York, NY:
Oxford University Press; 2007.
Publication Manual of the American Psychological
Association, 6th Edition. Book.
Washington, DC: American Psychological Association; 2009.
The CSE Manual for Authors, Editors, and Publishers, 8th
Edition. Book.
Council of Science Editors. Chicago, IL: University of Chicago
Press; 2014.
Reporting, Editing, and Publication of Scholarly Work in
Medical Journals. Web page.
International Committee of Medical Journal Editors.
www.icmje.org. Updated December 2013.
COMMONPLACES
AMWA Journal / V29 N2 / 2014 / amwa.org
57

Writing Guides
AMWA Toolkit for New Medical Writers. Web page.
www.amwa.org/toolkit_new_med_writers
The toolkit provides information on medical writing as a
career, opportunities in medical writing, getting started
in the field, and other useful information.
CDC’s Guide to Writing for Social Media. Web page.
www.cdc.gov/socialmedia/tools/guidelines/pdf/
guidetowritingforsocialmedia.pdf
This CDC guide offers guidance on using social media for
promoting health messages. The guide focuses on Facebook,
Twitter, and text messages (short message service, or SMS).
CDC’s Health Communication Digest. Web page.
www.cdc.gov/healthcommunication/sciencedigest/
index.html
The CDC’s Health Communication Science Digest provides
access to recently published articles and reports relevant for
the public health communication community. Abstracts and
PDF copies of most articles are available through the digital
object identifier (DOI) hyperlink included with each citation.
CDC’s Simply Put: A Guide to Creating Easy to Understand
Materials. Web page.
www.cdc.gov/healthliteracy/pdf/simply_put.pdf
Simply Put provides guidance for translating complicated sci-
entific and technical information into communication materi-
als general audiences can understand.
Creating Patient Education Materials. Web page.
BioMedical Library at University of Minnesota
Maintained by: Katherine Chew [email protected]
http://hsl.lib.umn.edu/biomed/help/creating-patient-
education-materials#toc20622
The page provides lists of many relevant articles, books,
videos, and illustrations.
A Field Guide for Science Writers: The Official Guide of the
National Association of Science Writers. Book.
Deborah Blum, Mary Knudson, and Robin Marantz Henig,
eds. (2006). New York, NY: Oxford University Press.
The guide presents material on effective science writing. The
book combines practical how-to advice about writing on
science and medical topics in general and covers a range of
workplaces students could find themselves in.
Genres in Scientific and Technical Rhetoric. Journal Article.
Carolyn R. Miller and Jeanne Fahnestock (2013). Poroi:
An Interdisciplinary Journal of Rhetorical Analysis and
Invention, Volume 9, Issue 1.
Miller and Fahnestock discuss differences and difficulties with
defining genres and their relevance to science and technology.
They provide an outline of the issues and questions.
Health Writer’s Handbook. Book.
Barbara Gastel (2004). Ames, IA: Blackwell Publishing.
The book is written for the new medical writer. It gives
guidance on selecting topics and gathering and analyzing
information, and provides an overview of ethical and legal
issues, and how to build a career in medical writing. I use
the first section that includes resources for gathering
information and strategies for interviewing medical
professionals and patients.
The Illusion of Certainty and the Certainty of Illusion:
A Case Study of Misunderstandings in Scientific Articles.
Journal Article.
Tom Lang (2013). AMWA Journal, Volume 28, Issue 3,
pages 105–109.
Lang discusses “analytical editing,” which involves the critical-
thinking skills necessary to edit a scientific article. These skills
are questioning the assumptions, documentation, and impli-
cations of the research. To illustrate the analytical editing pro-
cess, Lang provides an example of a singe sentence as
a case study. He shows how the sentence raises important
issues about meaning, measurement, statistical analyses,
presentation of data, and interpretation of results.
Judging the Quality of Medical Literature . Journal Article.
Teresa L. Rogstad (2009). AMWA Journal, Volume 24, Issue 4,
pages 176–181.
Rogstad states that medical writers need to be able to evaluate
the quality of the articles they use as information sources or
choose to cite in their own writing.
COMMONPLACES
58 AMWA Journal / V29 N2 / 2014 / amwa.org

COMMONPLACES
Khan Academy Stats Tutorials. Web page.
www.khanacademy.org/math/probability/descriptive-
statistics
Most of my students have backgrounds in the humanities,
so I try to find approachable resources on statistics. The
Khan Academy, a nonprofit organization that offers free
educational resources, has several videos about statistics.
Medical Tables, Graphics and Photographs: How They Work.
Journal Article.
Alan G. Gross (2007) Journal of Technical Writing and
Communication, Volume 37, Issue 4, pages 419–433.
The author’s examination of samples from four medical
journals—the Lancet, the New England Journal of Medicine,
JAMA: the Journal of the American Medical Association, and
the Journal of Laboratory and Clinical Medicine—reveals
that one-fifth of the space of articles in medical science is
devoted to an average of three tables and three flow charts,
graphs, or photographs. Noting the importance of visuals in
medical articles, Gross argues that we need to develop a
coherent vocabulary for talking about tables and visuals.
The Non-Designer’s Design Book.
Robin Williams (2008). Berkeley, CA: Peachpit Press.
All students in our program are required to take technol-
ogy and design courses, but students often take our medical
wiring course first. Williams’ text covers the basic principles
of good design and can help the students when executing
assignments such as creating a website or brochure.
Nude Mice and Other Medical Writing Terms You Need to
Know. Book.
Cynthia L. Kryder (2009).
Nude Mice is a language resource for students with little or
no background in science and medicine.
Online FDA Regulations: Implications for Medical Writers.
Journal Article.
Rita C. Tomlin (2008), Technical Communication Quarterly,
Volume 17, Issue 3, pages 289–310.
Tomlin argues that the availability of online Food and Drug
Administration (FDA) regulations contributes to a change in
the organizational role of medical writers. This shift is from a
peripheral role to a central role. As such, Tomlin argues that
the curricula for medical writers should include instruction
in persuasion, collaboration, strategic and project manage-
ment, the drug development process, and the location and
interpretation of FDA regulations.
Occupational Handbook Description. Web page.
www.bls.gov/ooh/media-and-communication/technical-
writers.htm
Technical writers, also called technical communicators, pre-
pare instruction manuals, journal articles, and other sup-
porting documents to communicate complex and technical
information more easily. They also develop, gather, and dis-
seminate technical information among customers, designers,
and manufacturers.
PubMed Tutorial. Web page.
www.nlm.nih.gov/bsd/disted/pubmedtutorial/cover.html
To help students learn how to research medical and scientific
topics and publications, I ask them to complete the PubMed
tutorial. The tutorial teaches students about PubMed’s scope
and content and Medical Subject Headings (MeSH). It also
teaches them how to build a search, manage search results,
and save search strategies.
The Science Writers’ Everything You Need to Know to Pitch,
Publish, and Prosper in the Digital Age. Book.
Thomas Hayden and Michelle Nijhuis, eds. (2013).
Philadelphia, PA: Da Capo Press.
The book is an all-around good resource and touches on
topics that many other texts also cover, such as ethics and
how to find article topics. I use the short chapter “By the
Numbers: Essential Statistics for Science Writers” to start our
class discussions on reading statistics.
AMWA Journal / V29 N2 / 2014 / amwa.org
59

20 Tips for Interpreting Scientific Claims. Web page.
www.nature.com/news/policy-twenty-tips-for-interpreting-
scientific-claims-1.14183
William J. Sutherland, David Spiegelhalter, and Mark
Burgman
This list will help nonscientists to critically assess informa-
tion provided by scientific resources. Items on this list include
issues of statistical power and the inherent imprecision of
measurement.
US Government Photos and Images. Web page.
www.usa.gov/Topics/Graphics.shtml - Health_and_Nutrition
For some of our class assignments, students are directed to
locate and use images. USA.gov has some resources that are in
the public domain or US government works and may be used
without permission or fee.
US Department of Health and Human Service’s Plain
Language: A Promising Strategy for Clearly Communicating
Health Information and Improving Health Literacy. Web page.
www.health.gov/communication/literacy/plainlanguage/
PlainLanguage.htm
This Web page discusses plain language and health literacy. It
also provides links to numerous other resources on the topics.
Writing in the Health Professions. Book.
Barbara A. Heifferon (2005). New York: Pearson Longman.
This textbook is aimed at medical professionals such as nurses,
but the chapters on audience analysis, ethics, and project
management are useful to professional writing students.
Writing Online Style Guide. Web page.
http://writingspaces.org/wwsg/title
The Writing Spaces Web Writing Style Guide was created as a
crowdsourcing project of Collaborvention 2011: A Computers
and Writing Unconference.
Writing Science in Plain English. Book.
Anne Greene (2013). Chicago, IL: University of Chicago Press.
The short guide (124 pages) offers 12 principles for writing
complex information based on readers’ needs. The principles
include understanding the importance of audience analysis,
the need to tell a story, and proper uses of the active and
passive voices.
Writing in the Sciences. Exploring Conventions in Scientific
Discourse. Book.
Ann M. Penrose and Steven B. Katz (2010). New York: Pearson.
I assign three chapters of this textbook: Science as a Social
Enterprise, Considering Ethics in Scientific Communication,
and Communicating with Public Audiences.
Author disclosure: The author notes that she has no commercial associ-
ations that may pose a conflict of interest in relation to this article.
Author contact: ar[email protected]
COMMONPLACES
60 AMWA Journal / V29 N2 / 2014 / amwa.org

AMWA Journal / V29 N2 / 2014 / amwa.org
61
Build Your Passion for Writing
into a Profession
NEW, ONLINE
MASTER OF SCIENCE IN PROFESSIONAL WRITING
New York University is an affi rmative action/equal opportunity institution. ©2014 New York University School of Continuing and Professional Studies.
Job Number: a1314-0595
Product: MS Professional Writing
Size: 8.5” x 11”
Bleed: .25
Color/Space: 4/c
Pub/Issue Date: AMWA (American Medical Writers Assoc.)
Summer Issue (mails June 1)
Date 4/10/14
Artist: pw
Proof #:1
Note: pu a1314-0594
NYU-SCPS Offi ce of Strategic Marketing and Communications
Information Sessions: Wednesday, June 11 and Wednesday, July 9, 6–8 p.m.
Kimmel Center, 60 Washington Square South, New York, NY
For event information and to R.S.V.P. visit scps.nyu.edu/graduate-events21a
To learn more about graduate programs,
visit us at: scps.nyu.edu/mspw1a or call 212-998-7100
For information and to apply: scps.nyu.edu/gradinfo21a
Curriculum Offered Completely Online
Complete the Program in Just Three Semesters of Full-Time Study
The 36-credit M.S. in Professional Writing, o ered by the NYU School of Continuing and Professional Studies (NYU-SCPS),
provides students with the opportunity to develop their writing, technical skills, and knowledge of communications in high-
demand fi elds including:
Study online with professionals who are industry leaders, and with peers from across the country and around the world.
Build an e-portfolio that will provide a comprehensive sampling of your work and will serve as an invaluable asset for
your future as a professional writer.
• Health Professions
• Digital Media
• Information Professions
• Business
• Proposals & Grants
• Finance
• Science
• Technical Writing
• Promotional Writing

62 AMWA Journal / V29 N2 / 2014 / amwa.org
A
lexandra Howson, PhD, CCMEP, belongs to a rare
new breed of medical writers. Howson serves cli-
ents who provide physicians with the newest, most
complicated, and most expensive form of continuing medical
education (CME) today. Howson’s clients deliver instruction
via the performance improvement format, called PI-CME for
short. These highly customized learning projects often require
cooperation among half a dozen organizations, 2 or 3 years to
design and complete, and budgets of more than $1 million.
PI-CME is “a fairly complex beast,” Howson, an AMWA
member trained in medical sociology at the University of
Edinburgh, says in her soft Scottish accent. The many clinical
and research stakeholders involved, and the frequent require-
ment for institutional review board approval, make PI-CME “a
bit like doing a research project. It’s not for the fainthearted.”
After a slow start, PI-CME is finally gaining more accep-
tance nationwide as a learning format. The number of physi-
cians who participated in a PI-CME activity more than tripled
from 2011 to 2012 (Table 1). Although the more traditional live
meetings, self-paced Internet modules, and regularly sched-
uled events like hospital grand rounds remain far more pop-
ular, PI-CME now draws more physician participants than
Internet searching and learning activities, according to annual
figures published last year by the Accreditation Council for
Continuing Medical Education (ACCME).
1
Responding to criticism about the effectiveness of tradi-
tional CME, in 2005 the American Medical Association (AMA)
approved both PI-CME and Internet search as novel learn-
ing formats worthy of earning continuing education credits.
Around the same time, AMA officials began to tout PI-CME,
in particular, as the most powerful way to not just educate
clinicians but also improve patient and community health
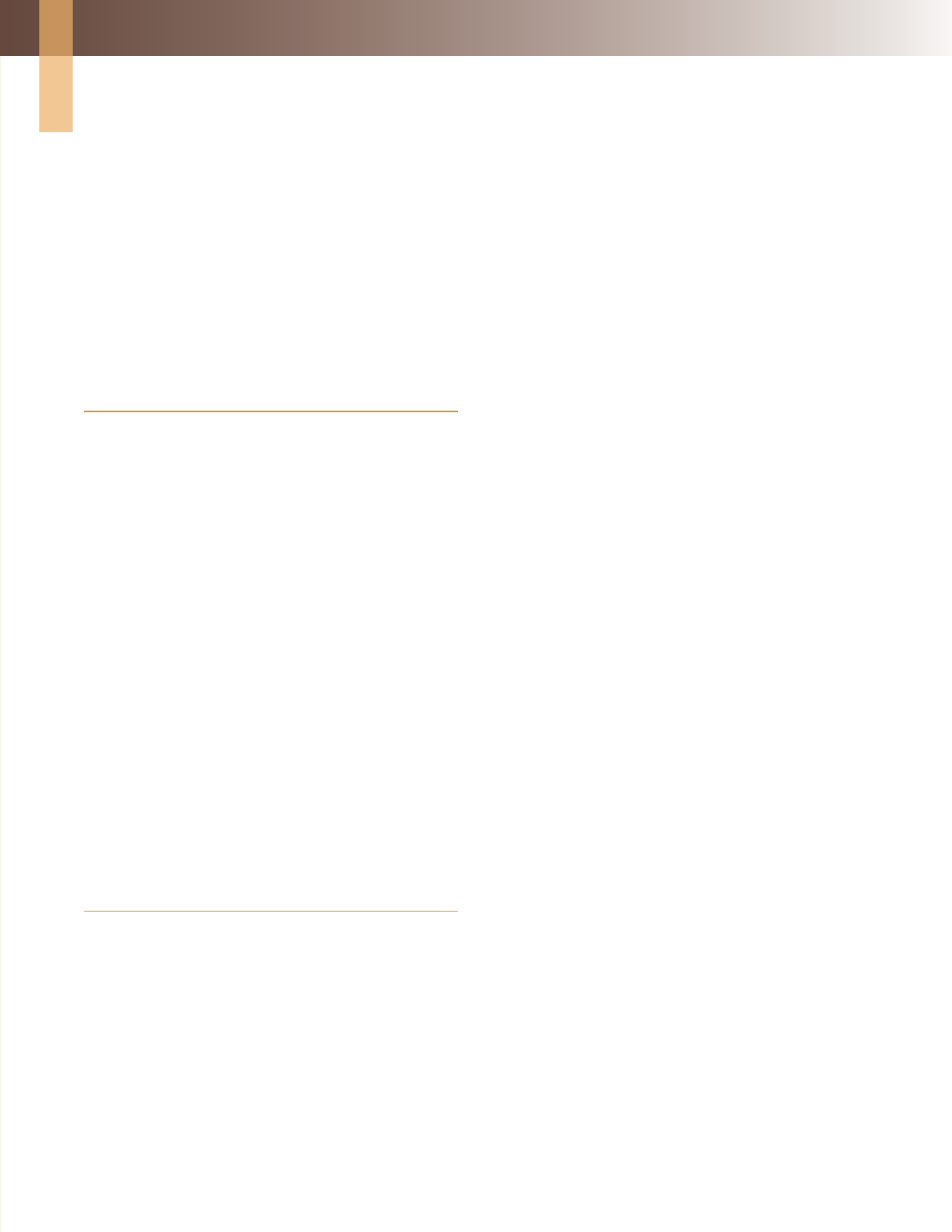
(Figure 1). Proponents even claimed PI-CME would become
“the core of the new CME.”
2
However, Internet search enjoyed
explosive growth from the start, drawing more than 50,000
physicians in its first year, compared to only 3,000 for PI-CME.
Until about 2010, CME providers struggled to find an audi-
ence for activities that use PI-CME’s unusual and highly struc-
tured format. The Internet searching and learning format
was much simpler—learners just needed to identify a rele-
vant practice-related question, find the answer online from a
trusted source, apply the new knowledge to patient care, and
demonstrate what they had learned. There was no requirement
to demonstrate an improvement in patient care. PI-CME sets a
higher standard. Barriers to uptake among physicians included
a general lack of familiarity with the concept, challenges in
shifting from knowledge-based to performance-based out-
come measurements, and time constraints on both teachers
and learners. PI-CME also suffered from a reputation of being
too expensive for education companies to develop, per capita,
compared to other formats.
“It took the CME community awhile to warm up to this
conceptually and learn how to do it right,” explains Mila
Kostic, director of the Office of Continuing Medical Education
within the Perelman School of Medicine at the University of
By Don Harting MA, ELS, CCMEP / Freelance medical writer, Downingtown, PA
Not for the Fainthearted:
Growth of Performance Improvement CME Presents Challenges,
Opportunities for Medical Writers
AROUND THE CAREER BLOCK
Year Internet Search PI-CME
2010 75,844 29,371
2011 92,114 44,275
2012 108,856 141,860
Table 1: Growth in Physician Participation
in CME Activities
Source: ACCME 2012 Annual Report
feature
AMWA Journal / V29 N2 / 2014 / amwa.org 63
Pennsylvania in Philadelphia. Attrition remains a common
problem, as physicians often start a PI-CME activity with the
best intentions, but then don’t finish. Time-consuming and
tedious data entry continues to be a key barrier to participa-
tion by physicians. Adds Kostic: “This has been a growth and
learning opportunity for all of us, as educators.”
GROWTH DRIVERS
Technically, nonphysicians may also participate in PI-CME,
but as a practical matter, few do: ACCME data from 2012 show
that physicians outnumber nonphysicians by a ratio of 15:1.
Diverse factors appear aligned to drive increased physician
participation in the future. Kostic, a fellow of the Alliance for
Continuing Education in the Health Professions (ACEHP),
predicts the ACCME’s 2013 annual report—to be released this
summer—will show continued growth. Major drivers include:
• Popularity among medical specialties. Of the eight catego-
ries of membership within the ACEHP, the medical specialty
category is where PI-CME enjoys the strongest foothold in
physician participation. Nearly 80% of physicians who took
part in PI-CME activities nationwide in 2012 did so through
nonprofit physician membership organizations, according
to ACCME data.
• Popularity among hospital executives. PI-CME seems a nat-
ural fit within larger hospitals and groups of hospitals, where
the culture of continuous quality improvement already
has deep roots. According to ACCME data, 57% of the 631
PI-CME activities offered nationwide last year were offered
by hospitals and health care delivery systems.
• Federal mandates. Beginning in 2015, the Centers for
Medicare and Medicaid Services’ Physician Quality
Reporting System will impose penalties for nonreporting
of performance data. Meanwhile, the Affordable Care Act
requires health plans and insurance issuers to show how
health outcomes are being improved in several ways, includ-
ing quality indices. These are the same types of quality data
used to drive and evaluate PI-CME activities.
• Electronic medical records (EMRs). Used properly, these
can be a powerful resource for an intervention that uses the
PI-CME format. Every EMR system requires creation of a
database, and once the database exists, it can be searched to
inform physicians how their patients are doing on many out-
come variables. These patient care data can then be used to
set a baseline, plan an intervention, and measure the results.
These three steps are common to all PI-CME activities.
• Publications in the medical literature. Outcomes data from
performance improvement initiatives were previously lim-
ited mostly to nonmedical journals; for example, a PI-CME
study of improved diabetes care at the Joslin Clinic was pub-
lished by an educational journal in 2011.
4
More recently,
however, medical specialty journals not just in diabetes,
5
but also in therapeutic areas as diverse as leukemia,
6
lung
cancer,
7
and osteoporosis
8
have begun accepting and pub-
lishing PI-CME outcomes reports. As physicians read these
articles in journals that cover their specialty areas, accep-
tance of the PI-CME format may continue to grow.
• Word of mouth. PI-CME does require significant time and
effort upfront, but once this initial investment is made, phy-
sicians often begin to feel a sense of ownership. According
to Kostic, they find the outcomes deeply rewarding because
they can actually see how their actions are improving
patient care.
ROLES FOR MEDICAL WRITERS
Gregory Liptak, president of a small, for-profit company out-
Level 1: Participation
Level 7: Community Health
Level 6: Patient Health
Level 5: Performance
Level 4: Competence
Level 3: Learning
Level 2: Satisfaction
Performance
Improvement
CME
Traditional
CME
Figure 1. High-Level Outcomes. PI-CME is designed to produce
measurable improvements not just in physician competence, but
also patient outcomes and community health. This graphic, pro-
vided with permission from Intelligent Medical Decisions Inc, refers
to the now-familiar hierarchy of CME outcomes rst described in a
2009 landmark article by Moore et al.
3

64 AMWA Journal / V29 N2 / 2014 / amwa.org
side Philadelphia, started out as a medical writer about 8 years
ago, and worked on traditional CME projects. He worked his
way up to the position of director of medical education at a
medical education company before leaving to team up with
business partners to form Intelligent Medical Decisions, which
specializes in PI-CME.
Liptak vividly recalls a time about 5 years ago when he
faced a daunting PI-CME writing challenge in diabetes.
Physicians enrolled in the activity had been instructed to
review the records of their patients with diabetes and measure
their performance against a nationally approved standard for
quality care: hemoglobin A1C goal attainment rates. It became
Liptak’s job to write what was essentially a customized gap
analysis for each physician, indicating where his or her perfor-
mance met the standard, and where it fell short. These analy-
ses were prepared after all participating physicians had entered
their patients’ records into a database.
“For each section of the report that dealt with a diabetes
performance metric,” Liptak recalls, “the medical writer’s job
was to go into the guidelines, provide a very concise summary
that was highly relevant to that particular measure, and add
language to the visual display of data that showed the provider
that the current status was not within the guidelines and pro-
vide an explanation as to why.”
Today, while he no longer carries the title of medical writer,
Liptak frequently writes the grant proposals that make new
PI-CME projects possible. He also expects his next hire to be a
medical writer.
“Good writing is critical for these programs,” Liptak says.
“You need to be able to communicate at the front end about
what you are measuring, and on the back end, for publica-
tion.” Liptak advises medical writers who would like to work
on PI-CME projects to gain a working knowledge of the many
national organizations that develop and publish quality stan-
dards for medical practice.
Working from her home office in the foothills of the
Cascade Mountains overlooking Seattle, Howson has devel-
oped a subspecialty: helping her clients prepare PI-CME out-
comes data for publication in peer-reviewed journals. She
advises freelance medical writers and editors who are starting
out in this complex field to ask many questions at the outset,
as a way to gather detailed knowledge of the various stakehold-
ers involved and a clear vision of how they are meant to work
together.
Alexandra Howson’s advice to medical writers: Ask
many questions at the outset to form a clear vision
of how all the various stakeholders in a performance
improvement continuing medical education project
are supposed to work together.
[ ]
Stakeholders Involved in REMEDIES (Risk Evaluation
and Mitigation Strategies: An Employer-Driven CME
Initiative for Ecacy and Safety)

AMWA Journal / V29 N2 / 2014 / amwa.org 65
It is common for a PI-CME initiative to produce enormous
amounts of raw outcomes data, Howson says. The write-up
then begins to resemble a clinical study report, though on
a much smaller scale, and the medical writer’s job becomes
one of sifting through piles of documentation in search of a
compelling story angle.
“Someone with a keen eye, some time, and some
tenacity can help turn those data into a piece of gold,”
Howson says.
A former Boy Scout, Don Harting enjoys exploring the ever-
changing landscape of continuing education in the health
professions. He tweets daily using the handle @CME_Scout.
Author disclosure: The author notes that he has no commercial
associations that may pose a conflict of interest in relation to this
article.
Author contact: [email protected]
References
1. ACCME 2012 Annual Report. www.accme.org/news-publications/
publications/annual-report-data/accme-annual-report-2012.
Published July 25, 2013. Accessed May 9, 2014.
2. Kahn N, Bagley B, Tyler S. Performance Improvement CME:
Core of the New CME. Vol Spring. Chicago, IL: American Medical
Association; 2007.
3. Moore DE, Jr., Green JS, Gallis HA. Achieving desired results
and improved outcomes: integrating planning and assessment
throughout learning activities. J Contin Educ Health Prof. Winter
2009;29(1):1-15.
4. Brown JA, Beaser RS, Neighbours J, Shuman J. The integrated Joslin
performance improvement/CME program: a new paradigm for
better diabetes care. J Contin Educ Health Prof. 2011;31(1):57-63.
5. Stowell S, Baum HB, Berry CA, et al. Impact of performance-
improvement strategies on the clinical care and outcomes
of patients with type 2 diabetes. Clin Diabetes. January 2014
2014;32(1):18-25.
6. Sekeres MA, Stowell SA, Berry CA, Mencia WM, Dancy JN.
Improving the diagnosis and treatment of patients with
myelodysplastic syndromes through a performance improvement
initiative. Leuk Res. Apr 2013;37(4):422-426.
7. Hirsch FR, Jotte RM, Berry CA, Mencia WA, Stowell SA, Gardner AJ.
Quality of care of patients with non-small-cell lung cancer: a report
of a performance improvement initiative. Cancer Control. Jan 2014;
21(1):90-97.
8. Greenspan SL, Bilezikian JP, Watts NB, et al. A clinician performance
initiative to improve quality of care for patients with osteoporosis.
J Womens Health (Larchmt). Oct 2013;22(10):853-861.
EXAMPLES OF PERFORMANCE
IMPROVEMENT INITIATIVES
1. REMEDIES (Risk Evaluation and Mitigation
Strategies: An Employer-Driven CME Initiative
for Ecacy and Safety). This is a mixed-
methods educational program including live,
Web-based, interactive, and performance
improvement (PI) activities. Physicians who
complete the program may earn up to 24.5
continuing education credits, of which 20 come
from the PI component. In addition, learners
may earn a certicate of compliance with
FDA educational requirements for prescribing
extended-release opioid analgesics.
2. Performance Improvement Strategies in Multiple
Sclerosis. Now in its third year, this initiative
is designed to help health care professionals
assess their clinical practice methods according
to current evidence and expert consensus.
Physicians who complete the activity may earn
credit toward maintenance of certication
(MOC) requirements set by the American Board
of Psychiatry and Neurology and 20 continuing
education credits from the American Medical
Association (AMA).
3. Advanced Clinical Management of Diabetes
and Its Complications. Completed in 2012, this
PI program was designed to give physicians
the chance to assess their current practice by
submitting data on patients with diabetes and
receiving condential reports on how their
performance compared to quality standards
established by the American Diabetes
Association and the AMA. Participants could
earn up to 20 continuing education credits from
the AMA and help satisfy MOC requirements set
by the American Board of Internal Medicine.

66 AMWA Journal / V29 N2 / 2014 / amwa.org
By Lori Alexander, MTPW, ELS / 2013–2014 Annual Conference Administrator
Shake, Rattle, and Write in Memphis
Shake your medical communication blues, rattle your pen
(laptop?), and write your ticket for professional development
at the AMWA Annual Conference in Memphis! Whether you’re
a newbie or veteran medical communicator, you will gain valu-
able knowledge and skills at this year’s conference. And with
this year’s location, you’re bound to have more fun than ever
after conference hours.
The Wonder of the Conference Program
This year’s conference program offers open sessions on a wide
variety of topics, from the practical advice in “Put on Your
Own Oxygen Mask First: Getting (and Staying) Organized”
to an overview of the latest in medical science in “Organ on
a Chip and Other Exciting New Advances in Non-animal
Biotechnology.” Nearly 60 roundtables provide a similar range
of diverse topics for medical communicators at every career
level, from beginning to experienced. Twelve posters have been
accepted for display, with presenters from all over the coun-
try—and world. (Poster abstracts are planned for the September
issue of the Journal.)
Rounding out the program are three Intensive Seminars,
the session format that debuted last year. The goal of Intensive
Seminars is to provide a more robust learning experience in
a particular topic, especially one that is outside the expertise
of typical AMWA members. This year, the planned Intensive
Seminars focus on how to combine cognitive science and
common sense to make effective presentations; leading, man-
aging, and writing in a global virtual environment, with best
practices for effective virtual meetings; and strategies for creat-
ing online health content for readers with limited literacy that
is relevant, motivating, and actionable. Intensive Seminars are
2 hours and 45 minutes long (with a 15-minute break), are lim-
ited to 40 to 50 attendees, and cost $40.
You’re the Boss: Personalize Your Program
This year, it will be easier than ever to find the events of most
2014 AMWA ANNUAL CONFERENCE PREVIEW
© Jack Kenner

AMWA Journal / V29 N2 / 2014 / amwa.org 67
interest to you. We are again using tracks to categorize ses-
sions according to broad topics, such as freelance, regulatory
writing, social media/technology, etc, and this year workshops
have also been assigned to these tracks. We also have devel-
oped “Track Facts”—simple reference guides that include all
sessions within each track—not just open sessions and work-
shops, but roundtables and posters too! The new Track Facts,
coupled with the Schedule at a Glance, will help you create
your unique program quickly and easily. Track Facts will also
help you demonstrate the value of the annual conference to
your boss or to yourself, if you’re a freelance. Track Facts are
available on the AMWA website at www.amwa.org/events_
annual_conference.
The conference app will also be available in the fall to help
you manage our personal program in your mobile device.
You’ll Never Walk Alone
If you are a new AMWA member or have never attended an
AMWA annual conference, don’t worry about being alone.
Many AMWA members and staff will be on hand to help wel-
come you and guide you. The traditional New to AMWA event
has been enhanced to focus on providing the most relevant
information and resources to new members and first-time
attendees. This event, Navigating AMWA and the Annual
Conference, will feature AMWA staff, chapter leaders, and
conference mentors who will help first-time attendees get the
most out of the conference. The event will be held Wednesday,
4:30 to 6:15 PM.
Burning Love for the Profession
If you are passionate about your profession, the annual con-
ference is the place to learn more about two professional
development opportunities: becoming an AMWA workshop
leader and taking the medical writing certification examina-
tion. Special tables will be available in the registration area,
where you can talk individually to AMWA staff and volunteers
involved in these initiatives. Special brief group talks (10 to 15
minutes) will also be scheduled throughout the day. In addi-
tion, you can learn more about becoming a workshop leader or
a certified medical writer by viewing posters on those topics in
the poster display section.
Can’t Help Falling in Love with AMWA Award
Recipients
The annual conference is also a time to honor AMWA award
recipients, and this year, recipients will be highlighted more
than ever (see box). As mentioned in the last issue of the AMWA
Journal, AMWA awards will be presented in a variety of venues
this year, offering you a greater opportunity to celebrate their
accomplishments with them. Onsite, look for posters describ-
ing the background and achievements of our award winners.
Online, you’ll be able to listen to award winners describe their
AMWA service in brief deskside chats.
You can also become better acquainted with the Alvarez
and McGovern award winners, Rosemary Gibson and Gary
Schwitzer, at the AMWA Meet and Greet Table, which will also
host AMWA members who have written a book. If you’re an
AMWA member and wish to take advantage of an opportunity
to promote your book, sign up for a time to be at the table by
sending an e-mail to [email protected].
Get All Shook Up for the 75th Anniversary
Celebration
Next year marks the 75th anniversary of AMWA, and plans are
underway for a full year of celebrating. Join us Saturday eve-
Week of June 16: Registration brochure available
July 1: Registration opens
August 30: Early registration ends

ning at the closing reception to kick off the celebration
that will culminate in the 2015 Annual Conference in San
Antonio.
Put on Your Blue Suede Shoes for a Tour
No visit to Memphis is complete without a visit to
Graceland. Even if you’re too young to have been an Elvis
fan, Graceland offers a glimpse into a historic time and an
even more historic celebrity. Tours of Graceland, with trans-
portation, will be offered on both Wednesday and Sunday,
starting with pick-up at 9:30 AM at the AMWA hotel (the
Sheraton) and returning between 12:30 and 1 PM. The ticket
price is $40.
For medical communicators, another must-do in
Memphis is a tour of St. Jude Children’s Research Hospital,
which is less than 1 mile from the convention center.
Complimentary tours exclusively for AMWA conference
attendees are being planned for Wednesday.
» Keep up to date on the conference by visiting the AMWA
website (www.amwa.org). Also, learn about more details
as they happen with the AMWA Conference Connector,
the Conference Blog—now available through AMWA’s
home page, Twitter (@AmMedWriters, #amwa14), and
LinkedIn groups.
2014 AMWA AWARD RECIPIENTS
Swanberg Award
J. Patrick Barron
Founder, International Medical Communications Center,
Tokyo Medical University
To be presented at the Sablack Award Lunch
AMWA Fellowships
Lori De Milto, MJ, Delaware Valley Chapter
Joanne McAndrews, PhD, Mid-America Chapter
Deborah Whippen, Florida Chapter
Justina Molzon, US Food and Drug Administration
(honorary fellowship)
To be presented at the Sablack Award Lunch
Golden Apple Award
Thomas Gegeny, MA, ELS, New England Chapter
To be presented at the Sablack Award Lunch
President’s Award
To be named
To be presented at the Opening Session
Eric W. Martin Award
Professional Audience: Art Gertel (with Cindy Hamilton,
Adam Jacobs, Gene Snyder, and Karen L. Woolley) for
“The Global Alliance of Publication Professionals: Update
on a Small Group with a Big Mission”
Public or Health Care Consumer Audience:
Randi Redmond Oster for “A Beautiful Choice: Living, and
Dying, with Dignity”
To be presented at the Closing Session
Student Scholarship
To be named
To be presented at the Welcome Reception
©Mr. Littlehands / CC-BY-SA-2.0
©Thomas R. Machnitzki / CC-BY-SA-3.0
68 AMWA Journal / V29 N2 / 2014 / amwa.org

The Harold Swanberg Distinguished Service Award is presented
each year to “an active member who has made distinguished
contributions to medical communication or rendered unusual
and distinguished services to the medical profession. The 2014
award will be presented to J. Patrick Barron at the annual con-
ference in Memphis, Tennessee. The winner will give an address
at the Sablack Awards Luncheon on October 10. J. Patrick
Barron submitted the following about his background in medi-
cal communication.
I am honored to be selected as this year’s recipient of the
Harold Swanberg Award. When I moved to Japan as a student, I
had no idea my career would lead me to this award.
In 1969, after completing a bachelor’s degree in English
literature at the University of Pennsylvania, I moved to Japan
where neither the country nor I knew that medical writing
existed. However, I began translating medical texts in 1971,
later enrolled in the MPhil/PhD program of the University of
London’s School of Oriental and African Studies, and in 1980
became associate professor of English, St. Marianna University
School of Medicine, in Kawasaki.
In 1975, I proposed a center to enhance the flow of scien-
tific information from Japan to the rest of the world by provid-
ing authors full English-language, medical writing, editing,
and translation support. In 1991, at Tokyo Medical University, I
founded the International Medical Communications Center—
the first of its kind in Japan—to provide these services to all
clinical and academic departments and to educate medical
and PhD students in English for medical purposes, scientific
publications, and publishing ethics. The center became a full
academic department in 2009, the only one in the country
authorized to develop and offer master’s and doctoral pro-
grams in medical communications.
In the new Department of International Medical
Communications, we created a standardized curriculum
to globalize the teaching of English for medical purposes.
The website now contains 18 clinical modules and videos of
physician-patient consultations, reading materials, and self-
assessment tests for medical students. South Korea and several
European countries are now implementing or considering this
program under the aegis of the European Union’s sTANDEM,
a standardized assessment system for English for medical pur-
poses, of which Tokyo Medical University is the only non-Euro-
pean partner.
In the meantime, I started the Medical Interpreters and
Translators Association (MITA) in 1993 and have been vice
chair of the Board of the Japanese Society for Medical English
Education for several years.
In 2005, I started what has become one of the largest web-
sites in the world on scientific publications and career develop-
ment, www.ronbun.jp. My colleagues and I invested more than
5,000 hours making more than 100, 60-minute videos for the
site, which also includes all the instructional materials I have
produced on medical writing and scientific publications during
the past 40 years.
I have been an editorial board member for several journals,
including the Journal of Gastroenterology, Breast Cancer, Haigan
(Lung Cancer), the Journal of Cardiac Surgery, and the Journal
of the Japanese Society for Geriatrics. As an editorial board
member for CHEST, I edited a monthly column called “Medical
Writing Tip of the Month.”
I received the 2005 Inagaki Educational Award for
Educational Achievements from Tokyo Medical University and
the 2007 Albert Soffer Award for Editorial Excellence from the
American College of Chest Physicians. I am also an adjunct
professor at Bundang Hospital, Seoul National University,
South Korea, and a member of the Committee on Publication
Ethics (COPE).
In addition to writing more than 35 peer-reviewed articles,
most on medical writing, medical education, and cardiopulmo-
nary medicine, I have edited and translated several key medi-
cal texts into English, two of which received Japan’s Translation
Publishing Culture Prize.
I retired in 2013 and became the first non-Japanese to be
awarded emeritus status at a Japanese medical school. My
tenure at Tokyo Medical University has been marked by many
successes, but perhaps the most important to me is that the
number of manuscripts published each year by TMU authors
rose from 18 in 1989 to nearly 300 in 2013, an increase more than
4 times the average of all other Japanese medical universities.
To have these activities and accomplishments recognized
by AMWA is, indeed, one of the highest honors I have received.
Thank you.
2014 SWANBERG AWARD
J. Patrick Barron
AMWA Journal / V29 N2 / 2014 / amwa.org
69
Y
ou can write. That’s why they want you. You have
experience writing the types of materials they need:
regulatory documents, continuing medical education
activities, promotional education materials, journal articles.
That’s why they want you. You specialize in the central ner-
vous system or metabolic disorders or cancer, and you know
all the regulations and guidelines and American Medical
Association style rules. That’s why they want you. This expe-
rience and training, and these skills, are the technical profi-
ciencies you possess.
However, it’s only half of what you need to be a “com-
plete professional.” The other half is that constellation of
qualities collectively referred to as “soft skills”: the nontech-
nical characteristics that make a technically talented person
a desirable professional. The term soft skills (in some places
they are referred to as transferable skills) is unfortunate; the
soft implies that they’re not that important when, truth be
told, they are as important as your technical skills.
So what are they? Before they acquired their own titu-
lar status, soft skills were the kinds of things you learned in
kindergarten, scouting, church, team sports, and yes, even
from your parents and teachers. No cheating, killing, lying,
or stealing. The Seven Deadly Sins might be entertaining at
a party, but gluttony and vanity would be looked upon with
disfavor in the workplace. There is no official list of soft
skills. You can find many resources online, but rarely will
two of them have the same set of skills, or group the skills
the same way, or emphasize the same items as the most
important skills.
Soft skills crop up in every job description. That’s usu-
ally the de rigueur part of the job description you gloss over,
since of course “everyone” has those skills: “enthusiasm,”
“ability to work in a fast-paced environment,” “good team-
building skills,” and the ubiquitous “deliver on time and
under budget.” I gloss over these desirable qualities myself
when I read job descriptions, despite the flaws I know I have:
I am not enthusiastic when clients wait 3 months before
signing off on a project; the “fast-paced environment” is
just fine until I get four concurrent assignments; I break out
in hives when directed to role-play during corporate team-
building retreats; and there truly is no such thing as “under
budget” when clients start down the path of “project scope
creep.”
This makes me a bit of a hypocrite to talk about soft
skills, but at least I know what these critically important skills
are, even if I sometimes struggle with manifesting some of
them. So what are they, exactly? Here is a sampling of them.
No one truly possesses of all of them (even if some individu-
als think they do possess them all, which is actually worse
than not possessing some of them). Think about the items
on the list. Can you apply them to yourself? It will probably
be easy to think of people you know who lack some of these
skills. What’s important is being able to recognize if you are
lacking a particular skill. If you can identify your challenges,
you can work to improve them. Note that these skills are uni-
versal; they do not apply only to medical communicators.
Interpersonal skills
Smile, make eye contact, be nice, listen to others, be sensi-
tive, cover your mouth when you sneeze or cough, and prac-
tice good grooming and hygiene.
Etiquette
Turn your mobile phone off during meetings, and never
answer it in a restaurant or when speaking to someone. Lose
the ear buds. Be sincere when saying please and thank you,
and say these things all the time. Be polite.
Positive attitude
Assume your projects will succeed. Conversely, never go into
a project thinking it is doomed to fail.
By Kelleen Flaherty, MS / Assistant Professor, Biomedical Writing Programs, University of the Sciences, Philadelphia, PA
praCtiCal matters
Soft Skills: The Critical Accompaniment
to Technical Skills
70 AMWA Journal / V29 N2 / 2014 / amwa.org

Self-condence
Believe in yourself, and believe in your skills. Recognize your
strengths. Poor self-confidence is obvious to others and will
limit your responsibilities and opportunities for promotion.
Self-confidence is not, however, the same thing as “arrogance.”
Unfortunately, the arrogant are pretty clueless about this.
Work ethic
Work hard. Work full days. Miss work rarely, but avoid “presen-
teeism” if ill. Take your work seriously. Help others even if it’s
not your job. Take on extra responsibilities if you have enough
time. Enjoy your work. Work hard but maintain work-life bal-
ance.
Cultural competency and sensitivity
Recognize that not everyone is like you with regard to age,
country of origin, religion, gender, sexual orientation, physical
ability, political affiliation, or marital and family status.
Time management
Never ever miss a deadline. You often have people working
downstream who require your deliverables before they can
start their work. Do not be late to work or meetings. Do not
procrastinate (you know who you are). You do not have to “just
finish this e-mail” while your colleagues wait for you for lunch.
I heard the movie producer and director Steven Soderbergh
speak once, and he said the greatest thing I ever heard: “If
you’re on time, you’re already late.”
Being a team player
Go on that retreat. Try to role-play without being snarky about
it. Help your teammates, consider and support their ideas,
make suggestions, and help. Serve as a mentor when pos-
sible, and be a respectful mentee when the situation calls for
it. Tolerate and try to help improve the limited competencies
some of your teammates might have, but at the same time do
not tolerate incompetency or toxicity in others.
Written and spoken communication
As a writer, your competency in writing is assumed, but you
also need speaking skills: lucidity, clarity, animation, enthusi-
asm, eye contact, and engagement. And you also should know
when to shut up. This applies to one-on-one interlocution as
well as speaking to a group or an audience.
Critical thinking
Can you assess things legitimately for their merit and accu-
racy? Can you set aside your biases (you have them, everyone
does) when judgment is called for? Can you restrain knee-jerk
responses? Can you listen to opposing views and assess them
for their merits? Can you practice both analytic and holistic
thinking? Do you understand logical fallacies? Can you think on
your feet and reflect and evaluate evidence? Are you scientifi-
cally literate? You need critical-thinking skills to be able to use…
Problem-solving and decision-making skills
Can you assess a problem rationally and critically and evalu-
ate the pros and cons? Can you use both inductive and deduc-
tive reasoning? If you look at the trees, can you back up and
look at the forest? If you tend to see the forest, can you zoom in
to the trees? Can you brainstorm new ideas, even wacky ones?
“Thinking outside the box” may be a cliché, but it is a good skill
to possess. Good problem-solving skills are necessary for…
Negotiation
If you are on a team and everyone agrees with each other, or
you work with a client who loves everything you pitch, you’re
working in some kind of fantasy dreamland. Business would
slam to a halt without compromise. Dig in your heels when
necessary, but be able to identify the things you can cede to
others and the things that can be acceptably modified to sat-
isfy the parties involved. Be respectful, but be tough.
Conict resolution
Technically under the aegis of problem-solving, conflict resolu-
tion is a type of problem-solving that is interpersonal. Conflicts
can be toxic, affect morale, delay project completion, imperil
deadlines, and lose you your clients. Conflicts need to be iden-
tified and resolved as soon as they appear.
Computational skills
For many of us, avoiding math is a lifelong goal, but you should
be able to understand budgets and cost modeling, basic math,
and statistics commensurate with the type of writing or editing
that you do. If you’re a freelance or entrepreneur, understand
the math associated with running your business.
Ethics
Personal, business, and medical ethical behavior is a must, for
yourself and for those you affiliate with professionally. If you
AMWA Journal / V29 N2 / 2014 / amwa.org
71

PRACTICAL MATTERS
work for a company that alters, withholds, is selective about,
or outright steals data (or that plagiarizes regularly), quit. Quit
even if you don’t have another job. Unethical behavior in medi-
cal communications can result in damage or death to a patient.
Working under pressure
Writing is by default a deadline-driven profession, and there
is nothing like a deadline to ramp up the pressure in one’s
life. Pressure can be compounded by multiple simultaneous
assignments, travel, family demands, and working with dif-
ficult teammates, superiors, clients, or consultants. When the
job description actually mentions “working under pressure,”
they’re not kidding.
Good judgment
In any job, you will be faced with problems and choices, and
you may suddenly find yourself in awkward situations. You
may have to make snap decisions. Does your behavior some-
times reflect bad judgment, such as relaxing too much with a
client or consultant, telling inappropriate jokes, or downing
too many drinks at a reception? Good judgment includes being
a good judge of character. People might not be who you think
they are; they might not be as trustworthy or respectful as they
outwardly appear.
Taking and giving criticism
Criticism is necessary for personal and professional growth.
Criticism can range from positive feedback to scathing
rebukes. Criticism is effective when it is constructive and
respectfully tendered, whether you are on the receiving end
or are doling it out yourself. You have to be open to receiving
it. It might not all be legitimate and might not all be useful,
but listen to it. You will never make it as a medical writer if you
become devastated or infuriated by criticism.
Flexibility
The last thing you want to hear (apart from “we’re going to do
a little role-playing exercise now”) is a client saying “I think we
want to go in a different direction” after you have submitted a
project you have been working on for 3 months. You have to be
able to adapt when project managers quit, new bosses arrive,
or you are suddenly shifted to a new project.
Leadership
You don’t have to be a vice president to be a leader. There are
responsibilities you’re going to have where you are the de facto
leader. It is easy to define a good leader: He or she simply pos-
sesses all the soft skills. A good leader listens and is compas-
sionate, transparent, fair, inclusive, and respectful and avoids
top down management. And, at least in my opinion, he or she
will never make you role-play.
No one has all the soft skills. You are deluding yourself if
you think you do. Individuals who are confident that they pos-
sess all these qualities are arrogant and serve as toxic speed
bumps on teams or in management. It is important that you
recognize where you have challenges and try to improve them.
I know my failings: I can be uncooperative and stubborn at
times, I procrastinate too much, and I can get snarky and sar-
castic when pushed. I’m dismal at math, and by all that is holy
I will resist role-playing until I draw my last breath. Sometimes,
to get what I need, I have to take the “ask for forgiveness rather
than permission” route, but if that’s what it takes to yield a
flawless product, I’ll do it. So much for my leadership skills.
But recognizing where I am deficient in soft skills does help me
to develop and strengthen them and become a better profes-
sional.
Think hard about each of these skills. Don’t do the “job
description glossover.” Make a table. Write an example of
one thing you do right for each, and one thing you do wrong,
however minor. Think about the qualities and flaws of other
people. There’s a reason certain coworkers annoy you, and it’s
very rarely because they don’t write well or don’t know AMA
style. It’s because they interrupt you when you are speaking,
are always late to meetings, are reading e-mail on their mobile
phones during meetings, or they are arrogant or insulting. Or
they make you role-play.
Author disclosure: The author notes that she has no commercial associ-
ations that may pose a conflict of interest in relation to this article.
Author contact: k.fl[email protected]
RESOURCES
Fisher R, Ury WL, Patton B. Getting to Yes: Negotiating
Agreement Without Giving In. Revised edition, 2011. NY:
Penguin Books.
Gallo A. How to work with someone you hate [blog post.]
Harvard Business Review website, January 30, 2012. http://
blogs.hbr.org/2012/01/how-to-work-with-someone-you-h/
Haden J. 8 qualities of remarkable employees. Inc., February
21, 2012. www.inc.com/jeff-haden/the-8-qualities-of-
remarkable-employees.html
Zimmerman, E. Smartphones should know their place
at work. New York Times, March 10, 2012. www.nytimes.
com/2012/03/11/jobs/etiquette-for-using-personal-
technology-at-work-career-couch.html
72 AMWA Journal / V29 N2 / 2014 / amwa.org

S
orry, I had to revive an old heteronym to grab your eye!
If we go by sound, that head should read Spice Up Your
Leed: Get the Led Out. Any of us writers who have been
exposed to newspaper journalism know the rule: Your lead (leed)
should contain the five W’s: who, what, when, where, and why.
(Random thought: We don’t have this kind of trouble with heed and
head—or with read or read !) The purpose was to give the reader the
gist of the article (without details) in the first paragraph, so that the
reader could quit at that point and still know the main points of
the article.
Yes, like a lot of my readers, I learned those five w’s early in my
career. And, I might add, I can still turn out a formal news story with
that pattern when I need to. We also know that feature stories (or
magazine articles) are a different thing. They don’t have to conform
to that rule. Occasional attention-grabbers—known colloquially
as “the hook”—add a little spice to your work to make it attractive,
readable, and interesting.
Sometimes the hook is the title, sometimes the lead following it,
and often both together. Here are some examples.
The title as hook
Writing with Suspenders This: ( ), That: — —, and The
Other Things: , ,
Sharp...but Dull
Title is Vital
This is a Complaint
Times, They Are A-changin’
The title as a question
Good Ole Days?
Have You Ever Seen...the Singular?
Two attention-grabbing leads
“First, I will advise you: Do not write a speech.”
“Years ago, it was easier. Most students didn’t know
the answer.”
Or, familiar song lyrics, familiar book quotes or jokes -- used to
create curiosity
“Your lips tell me no-no, but there’s yes-yes in your eyes”
“Someone once said that a camel was a horse put
together by a committee.”
Or, a combination of head and lead
By Arnold Melnick, DO / Aventura, FL
Spice Up Your Lead:
Get the Lead Out
MELNICK ON WRITING
Some newspapers carry a heading in addition to the
columnist's name (and maybe picture). In some instances, that
title is written by the columnist, and in others it is a regular news
headline added by the newspaper itself. Other publications
use a regular news headline written by the newspaper itself.
Fortunately for me, for all of the more than 160 signed columns
I have written in the past few years, I have been allowed to write
my own heading (title, not a newspaper headline). By this, I
was able many times to create a point with the heading and a
counterpoint with the lead—and together create an attention-
getting mechanism—a written hook. Some examples:
For a column on people who are brilliant in their field but
turn out to be boring speakers, my head was “Sharp…Dull” and
the tie-in lead, hoping to make the reader curious, was “How can
that be? Isn’t that an oxymoron?” A much duller lead could have
been “It is important for the physician not to discharge a patient
until he is certain that all her questions had been answered.”
For a column on the most important question a physician
can ask a patient, I titled it “Your Most Important Question,” and
the lead was “All right, Mrs. Brown, that about does it. I’ll see you
in three weeks.”
For a column headed “Listen to the Patient,” the lead was: “A
red light means STOP. A flashing red light means STOP! LOOK!
LISTEN!”
On a column about a newspaper article on patient care:
“What can you expect to learn about patient care from the Wall
Street Journal?”
All instances of eye-catching titles or clever leads, or both,
must be followed with an intelligent segue to the serious matter
of the article. In other words, once you have captured their
attention, quickly go to the meat of your column.
Remember, that your column—no matter how important it
may be, or how good you think it is—must first be seen by the
reader and then read. Thus, sometimes you have to think ahead
about attracting attention to it and then corral your readers.
My advice: Try to get away from the lead, that is, the heavy,
formal, stilted leads and go to something more attractive—and
interesting—to the reader. So heed my words and use your head,
read this column again and after it has been read, spice up your
lead by getting the lead out of it.
AMWA Journal / V29 N2 / 2014 / amwa.org
73

I use QuickBooks Pro from Intuit for all my business book-
keeping and timekeeping, and have been using this soft-
ware (upgraded versions, of course) since 1993. I love it and
highly recommend it. When a business expense comes in
(eg, monthly Internet fee), I log it into accounts payable
using the appropriate class designation. When I write the
check, the expense automatically attributes to the class,
so when I run my quarterly report, the expense is appro-
priately reported. I use this same process when I receive
invoices from writers and editors on my team, assigning
them as direct expenses to the appropriate job number.
That takes care of the expense side of my balance sheet.
On the ever-more-important income side of the balance
sheet, I use the estimating function in QuickBooks to pre-
pare estimates for every assignment. Then, when it comes
time to invoice, I simply identify the project by its job
number and turn the estimate into an invoice. QuickBooks
allows me to invoice for 100% of the total estimate, for a
percentage of the total estimate, or for any amount or per-
centage per line item, which makes “progress invoicing”
a snap. The sent invoice goes automatically into accounts
receivable, where I can track it until payment is received. I
then use QuickBooks to record received payments.
Because I track all my company’s business finances
in one place, it’s simple to prepare for my quarterly and
year-end meetings with my accountant. I am busy enough
running my business, so I am glad managing my business
finances doesn’t get in the way of making sure I have plenty
of money to manage.
—Brian Bass
I start by never using cash for anything and only using my
corporate credit card. This way I always have a receipt.
With American Express, you can also see all your expenses
by category.
My business is set up as a subchapter S corporation. I
have two bank accounts—regular checking and payroll—
with automatic transfers set up each month from regular
checking to payroll, from payroll to my home checking
account, and from regular checking to my 401K. Again,
keep it paperless.
I track everything in QuickBooks, and I use it for invoic-
ing and accepting payments. I used to manage it all myself,
downloading everything from the bank and American
Express, but about a year or so ago I hired a bookkeeper.
Her hourly rate is far lower than mine, and she’s far better
at it than me. She also pays my payroll taxes (which is all
done electronically), handles quarterly filings, and provides
me with a spreadsheet each year showing how much to pay
myself, taxes, etc. I use the online version of QuickBooks,
so my accountant and bookkeeper can access it and main-
tain it.
I do stick my receipts in a folder, then just store each
year’s.
I don’t have to do anything at tax time; my accoun-
tant can access income and expenses (by category) from
QuickBooks. She e-mails me any questions, tells me how
much I should put into my retirement fund, and files
everything.
Yes, I pay for these services, but it costs far less than it
would for me to do it myself, and I have peace of mind that
the experts are handling what they do best, while I handle
what I do best (writing and running my business).
— Debra Gordon
In our business, this is very easily accomplished, without
fancy programs or software. We have a corporate check-
ing account for all corporate business deposits and expen-
ditures. We use a corporate-only major credit card for all
expenses (travel and meal expenses generally). Office
supplies are billed to a corporate account at Staples or
Office Depot.
Whenever we do need to do reimbursements for out-
of-pocket expenses (mileage, hotel porters, maids, tolls,
etc), the check stub is used to divide the funds into various
categories to be applied to the appropriate expense item.
Brian Bass Elizabeth L. SmithDebra GordonLori De Milto
freelanCe forum
How do you keep track of business expenses for tax purposes?
Q
A
74 AMWA Journal / V29 N2 / 2014 / amwa.org

We use a certified public accountant who set up our system
20 years ago (with minor modifications over the years), so he
can easily calculate income and expenses for tax purposes.
Our business spreadsheet (which we still do by hand) balances
each month with our corporate bank checking statement. We
do not have a great deal of major business expenses, so the
system works for us. It is a simple system, one that takes us less
than an hour each month to record all business income and
expenses.
—Elizabeth L. Smith
TIPS FOR TRACKING TIME
Whether you bill hourly or by the project, it is crucial that you
track your time so you know how much time you spend on a
project. I prefer a software approach to tracking it manually
on a spreadsheet.
In my pre-Mac days, I used TraxTime, available at www.
spudcity.com/traxtime/ for $39. It is extremely simple to use.
You add the project, then punch in and punch out as you’re
working on it. You can run reports to see how many hours you
spent on it, or across all projects that day, week, or year.
Now that I’m a Mac person, I use OfficeTime, available at
www.OfficeTime.net for $47. (A Windows version is available
at the same price. iPhone and iPad apps are also available.)
It works similarly to TraxTime but also enables you to track
expenses, sync with iCal, and invoice right from the app. It
also creates pretty graphics from your data.
One of the best features of both programs is a reminder
box that pops up when you haven’t been typing but haven’t
logged out. It asks you if you still want to count the time that’s
passed. In other words, it keeps you from cheating!
—Debra Gordon
Track how you’re spending your time (per client, per project,
and on administration) by putting a small notebook next
to your computer. When you start working, note the client,
project, and time. When you stop, note the time. Do this for
every client and every project you work on, and also note the
amount of time you spend on administrative tasks.
At the end of each day, transfer your times onto a weekly
work log, either on paper (stored in a three-ring binder) or on
your computer. The work log should have rows for each day
and the weekly total, and columns for total hours, billable
hours, client (with room to track time for multiple clients),
and administration.
This method lets you quickly see whether you are spend-
ing too much or too little time on each client and on admin-
istrative tasks, and how much you’re actually working (eg, not
surfing on the Web or talking to family or friends) during your
hours in the office.
—Lori De Milto
TIPS FOR CREATING JOB NUMBERS
Assigning a job number to every project makes it simple to
track the job from start to finish. Job numbers serve several
important purposes. They provide a logical way to save all the
files related to each project. They also enable you to track the
project financially including your estimates, invoices, and any
expenses you may have that are related to the job. Another
important function of job numbers is providing a way for you
to track down a job you did long ago. There’s no right or wrong
way to assign job numbers, but here are a few tips for creating
job numbers that may prove helpful down the line.
Tip #1: Consider how many projects you work on during the
year. If you don’t work on many projects throughout the year, a
job number might serve as simply a name for the project so you
can identify it. You could call it “1,” or “01,” or almost anything
else, and that would probably suffice. You could even give it a
name if you prefer, like “Product X CSR” or “Gary.” But if you
work on a lot of projects during the year, you might want a
slightly more sophisticated numbering system.
Tip #2: Consider what is most important to identifying the
job. If you work with a lot of clients, you might want to create a
job numbering system that identifies the client associated with
the project. You might prefer to use a numbering system that
identifies the product on which you’re working. Or, you might
want a numbering system that identifies both the client and
the product.
Tip #3: Consider what will be most helpful in tracking down
the job. Regardless of the type of job numbering system you
use, it’s important to have a master job number list. This way,
you can cross-reference to the master list when you’re search-
ing for a particular project. If you’re most likely to remember
the client for whom you did a certain project, using a number-
ing system that identifies the client first and a master list that
groups job numbers by client would be best for you. If you’re
most likely to remember when you did a particular project (eg,
“Last fall, I think…”), then a numbering system that reflects
the month or season and a master list that groups job numbers
the same way would be best. Adding a year to your numbering
system might also be helpful.
Tip #4: Consider what is most important to your success.
Logging in a certain number of projects for a particular client
might be the key to knowing whether you are having a good
year. If so, a job numbering system that identifies the client and
the number of projects you have done for that client might be
helpful. If you track projects by the month or season, you might
want to marry that with the number of projects to create your
job numbering system. If the sheer number of projects you log
in a given year is indicative of income, then a simple number-
ing system that counts the number of projects might work best
for you.
Remember, there’s no right or wrong way to create a job
numbering system. Use these tips to create a system that works
best for you.
—Brian Bass
FREELANCE FORUM
AMWA Journal / V29 N2 / 2014 / amwa.org
75

I
think most of us could benefit from greater knowledge
and understanding of social media. I know I could.
The problem is wading through the array of informa-
tion clamoring for our attention online to find people who
really know what they are talking about when it comes to
social media marketing. To make that task easier, I’ve com-
piled an alphabetical list of five online influencers who are
well known as experts in marketing and social media. These
people are passionate about social media, and I eagerly con-
sume the ideas, strategies, and tactics they share on their
blogs and in their books. Now, if only I could put all of their
wonderful ideas into practice. Start following any of them
and you will probably feel the same!
Seth Godin (www.sethgodin.com). Godin is an author,
entrepreneur, and marketer who writes about marketing,
leadership, and the ways ideas spread. His book, Permission
Marketing, which launched 15 years ago, focused on con-
necting brands and consumers through online marketing
campaigns that first sought the consumer’s permission to
engage, that is, to opt-in to receive marketing messages. At
the time, the idea of seeking consumers’ permission was
revolutionary and not very well received by direct market-
ers, as you can imagine. Today, opting-in is the standard on
the Internet. Godin has written numerous books, includ-
ing Unleashing the Ideavirus, Tribes, Purple Cow, and All
Marketers Are Liars. He offers a variety of content for free, as
downloadable PDFs, on his website. Godin is also the cre-
ator of Squidoo (www.squidoo.com), a platform that enables
users to create custom Web pages called lenses on various
topics of interest.
Neal Schaffer (nealschaffer.com). Schaffer is a social
media consultant and adviser who delivers a wide range
of social media tips, with a focus on LinkedIn. You’ll find
useful content on either one of his websites: Maximize
Your Social http://maximizeyoursocial.com and Maximize
Social Business http://maximizesocialbusiness.com. He
is the author of Maximize Your Social: A One-Stop Guide to
Building a Social Media Strategy for Marketing and Business
Success, a useful book if you are struggling to design a social
media strategy for your business. He also has written two
other highly regarded social media books: Maximizing
LinkedIn for Sales and Social Media Marketing, and Windmill
Networking: Understanding, Leveraging, and Maximizing
LinkedIn.
By Cynthia L. Kryder, MS, CCC-Sp / Medical Communications Consultant, Phoenixville, PA
Five Social Media Gurus to Follow
SOCIAL MEDIA
76 AMWA Journal / V29 N2 / 2014 / amwa.org

Mari Smith: (www.marismith.com). Dubbed “the Pied
Piper of Facebook,” Smith is considered to be a global leader
in social media strategy and THE top Facebook marketing
expert in the world. Dun & Bradstreet identified her as one
of the most influential small business people on Twitter
1
and Forbes named her as one of the top ten influencers
online.
2
She is author of The New Relationship Marketing
and coauthor of Facebook Marketing: An Hour A Day. Smith
has made social media her specialty and her website is filled
with content you can use to develop relationships and build
your social media network.
Michael Stelzner. Another leading voice in social media,
Stelzner is the founder of Social Media Examiner (www.
socialmediaexaminer.com), the world’s largest online
social media magazine. He also is one of the driving forces
behind the Social Media Success Summit, a live, online con-
ference with presentations by some of the world’s leading
social media influencers. He has written the books Launch:
How to Quickly Propel Your Business Past the Competition
and Writing White Papers: How to Capture Readers and
Keep Them Engaged. He hosts the Social Media Marketing
Podcast show (https://itunes.apple.com/us/podcast/
social-media-marketing-podcast/id549899114), designed
to help businesses thrive with social media.
Gary Vaynerchuk (http://garyvaynerchuk.com/).
Vaynerchuk used social media to propel his family’s liquor
store in New Jersey from a $3 million business into a $45
million enterprise. In the process, he created Wine Library
TV (http://tv.winelibrary.com) and built a loyal commu-
nity of wine lovers. In 2009, Vaynerchuck and his brother
launched VaynerMedia, to help Fortune 500 companies find
their social voices and build their digital brands. He is the
author of three books: Crush It!: Why Now is the Time to Cash
in on Your Passion, The Thank You Economy, and Jab Jab Jab
Right Hook: How to Tell Your Story in a Noisy Social World.
Author disclosure: The author notes she has no commercial associa-
tions that may pose a conflict of interest to this article.
Author contact: [email protected]
References
1. Luther D. The most influential small business people on Twitter.
D&B Credibility Insights blog. June 2011. http://blog.dandb.com/
2011/06/20/most-influential-small-business/. Accessed May 5, 2014.
2. Shaughnessy H. Forbes. Who are the top 50 social media
power influencers 2013? April 2013. www.forbes.com/sites/
haydnshaughnessy/2013/04/17/who-are-the-top-50-social-media-
power-influencers-2013/2/. Accessed May 5, 2014.
SOCIAL MEDIA
AMWA Journal / V29 N2 / 2014 / amwa.org
77

78 AMWA Journal / V29 N2 / 2014 / amwa.org
A
decade ago, Bill Gates declared that the password
would soon be dead.
1
Instead, passwords have con-
tinued to proliferate, and there doesn’t seem to be a
good alternative on the horizon. For most people, passwords
have become an integral and frustrating part of daily life.
Better off dead. Despite continued high profile data
breaches that underscore the need to protect online infor-
mation, most Internet users manage their passwords poorly.
This is hardly surprising. Creating and recalling dozens of
complex, individual passwords is a formidable and oner-
ous task. To simplify matters, people often write down their
passwords, store them in insecure places, or choose weak
ones that are easy to remember. In 2013, 123456 and pass-
word were still the two most common passwords.
2
One of the
worst habits is password reuse. A 2012 study found that most
adults in the United Kingdom were using the same password
at multiple (or even all) websites.
3
Although there isn’t a perfect solution to the password
management problem, implementing some fairly simple
measures can help mitigate risk.
Train your brain. Consider using a passphrase instead of
a password. Passphrases are usually long and sufficiently
complex, but are easy to type and remember. It’s important,
however, to avoid phrases that can be easily guessed, such as
popular quotes, movie titles, and song lyrics. For these rea-
sons, some experts suggest inventing a lie or using a nonsen-
sical sentence. Others suggest using a series of common but
unrelated words (eg, correct horse battery staple),
4
or using
person-action-object statements, such as “Bill Gates swal-
lowing a bicycle.”
5
Creating a visual or story that goes with
the words can aid memorization.
Although passphrases can help you memorize long
strings of characters, they do not address the problem of
remembering which one goes with which account. One
solution is to create a strong base password, and then apply
a rule that incorporates elements of the website to which
it belongs. This enables generation of custom passwords
linked to a specific website and only requires remembering
the password core and formula. One problem with this strat-
egy is that different websites often have different charac-
ter requirements (length, allowable symbols, etc), so it may
be difficult to create a base password and rule that can be
applied across the board. Moreover, hackers are well aware
of the common techniques for creating and obfuscating
passwords, so the formula must be clever.
One password to rule them all. An alternative to memoriz-
ing all of your passwords is to have a software program do it
for you. Password managers like OnePassword and LastPass
store encrypted login information for all of your accounts
behind a single master password. There are many types of
programs to choose from, and most offer basic services that
are free or available for a nominal fee. Many password man-
agers will evaluate the strength of existing passwords and
can also generate long, random passwords for you. Some
offer additional features such as filling out forms automati-
cally or tracking other bits of data such as personal iden-
tification, bank account, or credit card numbers. Because
creating a single point of failure creates a major vulnerability,
some password managers also offer a two-factor authentica-
tion system that uses biometrics or a hardware device.
Don’t forget the reset button. Even highly complex, unique
passwords won’t be effective if hackers can simply change
By Laura Mizoue, PhD / Research Specialist, Howard Hughes Medical Institute, Department of
Chemistry and Biochemistry, University of Colorado, Boulder, CO
teCh talk
Password Management:
Staying Safe and Sane

AMWA Journal / V29 N2 / 2014 / amwa.org
79
them on the fly. The challenge questions used for retriev-
ing or resetting forgotten passwords are often based on per-
sonal information that can be easily guessed or found online
(What is your favorite color? What is your mother’s maiden
name?). One work-around is to use false or counterintui-
tive answers, such as “pizza” instead of your mother’s actual
maiden name.
6
Of course, this adds to the amount of infor-
mation that must be remembered.
Unfortunately, no password is unbreakable, and hack-
ing techniques are only going to improve with time. By vary-
ing your passwords, however, you can at least reduce the
likelihood that a hacker breaking into one site can use that
information to gain access to your other accounts. Although
it’s difficult to know how effectively companies are protect-
ing your private information, a good password management
system can help ensure that you aren’t the weakest link.
Author disclosure: The author reports that she has no commercial
associations that may pose a conflict of interest in relation to this
article.
Author contact: [email protected]
References
1. Gruener W. Bill Gates: The password is dead. Tech Guru Daily website.
www.tgdaily.com/technology/5166-bill-gates-the-password-is-dead.
Published November 16, 2004. Accessed May 11, 2014.
2. Doel K. “Password” unseated by “123456” on SplashData’s annual
“Worst Passwords” list. Splashdata website. http://splashdata.com/
press/worstpasswords2013.htm. Published 2013. Accessed March 7,
2014.
3. Adults’ media use and attitudes report. Ofcom website. http://
stakeholders.ofcom.org.uk/binaries/research/media-literacy/adult-
media-lit-13/2013_Adult_ML_Tracker.pdf. Published April 2013.
Accessed March 3, 2014.
4. Munroe R. Password Strength. XKCD website. http://xkcd.com/936/.
Published August 10, 2011. Accessed March 2, 2014.
5. Blocki J, Blum M, Datta A. Naturally rehearsing passwords. arXiv
website. http://arxiv.org/pdf/1302.5122.pdf. Published September 9,
2013. Accessed March 8, 2014.
6. ‘What everyone needs to know’ about today’s cyberthreats. NPR
website. www.npr.org/2014/01/14/262387292/what-everyone-needs-
to-know-about-todays-cyberthreats. Published January 14, 2014.
Accessed March 2, 2014.
TECH TALK
Wired Magazine: Study Finds Widespread
Vulnerabilities in Hospital Equipment, Medical
Devices, and Electronic Health Records
A 2-year internal study by a Midwestern health care
network identied a disturbing and extensive lack
of security that could potentially leave nearly every
aspect of the health care system open to hackers.
Vulnerabilities were found in medical devices such as
drug pumps for insulin and pain management, im-
plantable cardioverter-debrillators (ICDs), CT scan-
ners, and robotic surgical systems; hospital storage
and climate control systems including refrigeration
units that store blood and pharmaceuticals; and
medical record and image-archiving systems. Many
of these systems lacked rigorous authentication
protocols for allowing access and reconguration,
and many were connected to intranets or even the
Internet, leaving them wide open to manipulation.
The study was conducted in about 100 hospitals,
health clinics, and pharmacies by Scott Erven, head
of Information Security at the Essentia Health
network. To their credit, Essentia Health leader-
ship decided to publicize the ndings of the study,
recognizing that the problem is likely rampant
throughout the nation and around the world.
For more in-depth coverage, please read the full
story in Wired. www.wired.com/2014/04/hospital-
equipment-vulnerable/
— Jeanne McAdara-Berkowitz
TECH NOTES
Even highly complex, unique
passwords won’t be effective
if hackers can simply change
them on the fly.

W
e all do it, even though some of us may hesitate
to admit it. We search Google and its more aca-
demic cousin Google Scholar for medical infor-
mation. According to a 2010 survey, the three most popular
databases among science researchers are PubMed, Web of
Science, and Google Scholar.
1
Google Scholar may not have the scholarly reputation of
the other two, but it requires no subscription (unlike Web of
Science), is easy to use, and can even yield results not avail-
able in PubMed. When searched effectively, Google Scholar
can be an important and helpful resource to supplement
information found in other academic literature databases. As
with any database, the key to searching Google Scholar effec-
tively and efficiently is to understand what it can and cannot
do (Table 1) and to use some of its unique properties.
Google Scholar will retrieve published and unpub-
lished literature, conference papers, technical reports, dis-
sertations, pre-prints, drafts, patents, abstracts, and many
By Michelle A. Kraft, MLS, AHIP / Senior Medical Librarian, Cleveland Clinic Alumni Library, Cleveland, OH
Table 1: Comparison of Academic Literature Databases
Database Features Google Scholar PubMed Web of Science
Controlled vocabulary No Yes (MeSH) No
Period covered ? 1946 may have some older
material
1900-
Publications covered ? ~5600 journals 12,000 journals & 150,000
conference proceedings
Update frequency Google says several times a
week, but updates to some
existing records take more
than 6 months.
Daily Weekly
Citation counts Yes No Yes
Export to reference
software
1 record at a time Yes Yes
Alerts Yes Yes Yes
Truncation symbols No Yes Yes
Provides search limits
(date, publication type,
age, etc.)
Limited. Date, journal name,
author
Extensive. Can limit by age group,
humans, animals, type of article
such as guidelines, randomized
control trial, meta analyses
Yes
Searches full text Yes No No
Boolean Searching (and,
or, not)
Yes Yes Yes
find
80 AMWA Journal / V29 N2 / 2014 / amwa.org
Making the Most of

other document types. It finds these items from publisher
sites, online repositories, professional societies, and universi-
ties. Google Scholar provides a way to track article citations
and follow the links to citing articles. Searchers with college or
university library privileges can add links to their institutions
(under “library links” in the settings area of Google Scholar).
The library links are added to search results, making it easy to
gain access to articles that normally require a fee but are paid
for through library subscriptions.
Although Google Scholar has the ability to retrieve a lot of
resources from very diverse areas, it does not search the “deep
web” that consists of sites that require logins, have pay walls,
or are otherwise buried deep in university
repositories or websites.
Document Retrieval
Google Scholar lists results by date or accord-
ing to “relevancy,” which it determines
through its own algorithm. Although Google
does not disclose the exact nature of the algo-
rithm, it uses information within the full text
of the article, author, and journal informa-
tion, and the number of times an article has
been cited by other journals to help build the
list of relevant results. Other databases, such
as PubMed, rely on their indexing systems,
which use controlled vocabulary terms, in
addition to author and journal names, article titles, and other
article information, to build the list of relevant results. The lack
of information about the Google Scholar algorithm is one of its
downsides, as it is easier to create effective searches by know-
ing how a database retrieves articles.
Term Mapping
One key difference between Google Scholar on the one hand
and PubMed and other scientific databases on the other hand,
relates to the issue of “term mapping” and how synonyms are
handled. Google Scholar does not use controlled vocabulary
to index items. Google Scholar finds items only if the speci-
fied terms actually appear within the full text of the article
or abstract. There are no subject terms added to increase
retrieval.
This can have positive and negative implications. Web
searchers and authors tend to use terms common to their pro-
fessions or every day language in their articles and search strat-
egies, not the indexing terms in controlled vocabulary. The use
of familiar language makes it easy and can yield some good
results. It does, however, limit the ability for people to find
articles that use alternative spellings or synonyms. By contrast,
PubMed maps popular key words and terms to Medical Subject
Heading (MeSH) controlled vocabulary index terms (Figure 1).
Google Scholar has not developed a way to map similar terms.
Therefore, to retrieve all relevant articles on breast cancer, for
example, Google Scholar searchers might also need to include
the terms tumor and neoplasm. For medical communicators,
this term mapping issue can be important in many situations,
such as preparing systematic reviews or meta-analyses or iden-
tifying gaps in the research literature.
Truncated Words
Google Scholar does not recognize truncation symbols. It uses
“automatic stemming,” which means it looks at the word and
adds any additional letters on the end of that word. The word
jump would also include the terms jumps, jumped, and jump-
ing. Unfortunately, searching by the shortened root of the word
does not get all variants. Searching for the term surge will not
retrieve surgery, surgeries, or surgeon. Google Scholar search-
ers must not only include possible variants and synonyms for
terms and include them in their search strategy but also be
aware that automatic stemming might require them to use
additional terms.
Boolean Operators
Google Scholar uses Boolean operators, but there are some
things to be aware of. Scholar automatically adds the word
AND between search terms or sets of search terms in parenthe-
ses. The searcher must deliberately type the word OR between
terms or sets of parentheses. Additionally, the Boolean term
Figure 1. Example showing how PubMed maps words entered into the search box to
nd synonyms. A search for breast cancer will retrieve articles that have been indexed
under the medical subject heading term breast neoplasm.
Search Details
Query Translation:
"breast neoplasms"[MeSH Terms] OR ("breast"[All Fields] AND
"neoplasms"[All Fields]) OR "breast neoplasms"[All Fields] OR
("breast"[All Fields] AND "cancer"[All Fields]) OR "breast
cancer"[All Fields]
PubMed
breast cancer
Search
FIND
AMWA Journal / V29 N2 / 2014 / amwa.org
81

OR must be in all capital letters or it will be ignored. Somebody
doing research on cancer may want their search strategy to
look like this: cancer OR neoplasm OR tumor.
Google Scholar does understand parentheses that are used
in search statements. Much like in addition and multiplication
problems, the parentheses force Google Scholar to combine
search terms in a specific way. For example, someone look-
ing for information on colon cancer might want to type colon
AND (neoplasm OR cancer OR tumor). If the searcher does
not use parentheses and capitalized Boolean terms, then he
or she might get articles about the colon as well as articles on
other types of cancer, cluttering their results on colorectal neo-
plasms. Searchers who don’t want any articles on rectal cancer
can use the minus symbol (hyphen) to eliminate the word
rectal. The search phrase would look like this: colon (neoplasm
OR cancer OR tumor) -rectal. (There are dangers, of course, in
such a strategy. The word rectal could be mentioned briefly in
an article that otherwise would meet the searcher’s needs.)
Google Scholar’s advanced search function enables searchers
to look for specific authors, publications, titles, date ranges,
and subject areas. Any search result can be turned into an
automated e-mail alert to be notified of new papers.
Limitations
Unlike other databases, Google Scholar does not actually con-
tain any full text articles or abstracts. Instead, it data mines
websites and uses its algorithms to display the search results.
Therefore if the information that Google Scholar finds is incor-
rect, then the search results will be incorrect. In the past,
Google Scholar’s server has had some problems correctly
identifying authors, titles, and journals. The article “Google
Scholar’s Ghost Authors” by Peter Jasco describes how Scholar’s
crawling techniques misidentified many authors of articles as
“subscribe” or, in the case of a Lancet article, “fabricated the
first initials and the last name of the first author from the sub-
title of another paper and the second author’s name from the
title of a third paper.”
2
While it appears Scholar has addressed
some of the indexing issues, it still seems to have problems. As
recently as February 2013, blogger Karen Blakeman reported
Google Scholar erroneously listed an author as “MA Lib”
instead of the correct author K. Fraser.
3
Since Google Scholar
factors the number of times a paper has been cited to help
build the list of relevant results, Google Scholar’s ghost authors
may affect search results.
Citation searching is a helpful way to supplement a Google
Scholar subject search. Simply click on the “cited by” link to
see the authors who cited that specific work. Although the cita-
tion searching is helpful, it is important to know that this can
be easily manipulated artificially. In the article, “Manipulating
Google Scholar Citations and Google Scholar Metrics: simple,
easy and tempting,” researchers reported that they could arti-
ficially increase an article’s display rank by uploading fake
papers to the Web that are discovered by Google’s Web crawl-
ers. Their experiment resulted in an increase of 774 citations
for 129 papers.
4
While there hasn’t been a documented case
of somebody manipulating citations to increase their article’s
ranking, it is important to be aware of as other databases such
as PubMed, Web of Science, and Scopus are not as vulnerable
to this type of manipulation.
Several recent studies have found that searching Google
Scholar can be helpful and yield interesting and relevant
results. For quick clinical research, Google Scholar can be quite
effective. A study of nephrologists seeking information for clin-
ical questions found “Google Scholar returns twice as many
relevant articles as PubMed and provides greater access to
free full-text articles.”
5
Scholar may be effective for quick clini-
cal questions, but it may not be as effective for other search
queries. The authors of an article in Systematic Reviews found
Google Scholar’s article retrieval “too low” to be used as a
single database for conducting systematic reviews.
6
No database is perfect; every database has its strengths and
weaknesses when it comes to indexing, structure, and cover-
age. To find comprehensive information on a subject, search-
ers must look at a variety of databases. Because each database
is created differently, it is essential to know how those differ-
ences affect searching and to adjust the search strategy accord-
ingly. Google Scholar is a very helpful database and can serve
as a great additional tool for retrieving articles.
Author disclosure: The author notes that she has no commercial associ-
ations that may pose a conflict of interest in relation to this article.
Author contact: kraftm@ccf.org
References
1. Hightower C, Caldwell C. Shifting Sands: science researchers on Google
Scholar, Web of Science, and PubMed, with implications for library
collections budgets. Issues in Science and Technology Librarianship 2010.
www.istl.org/10-fall/refereed3.html. Accessed February 4, 2014.
2. Jasco P. Google Scholar's ghost authors. Library Journal 2009; http://
www2.hawaii.edu/~donnab/lis670/lj_print.pdf. Accessed February
4, 2014.
3. Blakeman K. Google Scholar author fail. 2013; www.rba.co.uk/
wordpress/2013/02/04/google-scholar-author-fail/.
4. Lopez-Cozar ED, Robinson-Garcia N, Torres-Salinas D. Manipulating
Google Scholar citations and Google Scholar metrics: simple, easy and
tempting. 2012. http://arxiv.org/abs/1212.0638
5. Shariff SZ, Bejaimal SA, Sontrop JM, et al. Retrieving clinical evidence: a
comparison of PubMed and Google Scholar for quick clinical searches.
J Med Internet Res. 2013;15(8):e164.
6. Bramer WM, Giustini D, Kramer BM, Anderson P. The comparative recall
of Google Scholar versus PubMed in identical searches for biomedical
systematic reviews: a review of searches used in systematic reviews.
Systematic reviews. 2013;2(1):115.
FIND
82 AMWA Journal / V29 N2 / 2014 / amwa.org

AMWA Journal / V29 N2 / 2014 / amwa.org
83
Committee on Publication Ethics North
American Seminar
August 13, 2014
Philadephia, PA
http://publicationethics.org/events
International Society of Managing and
Technical Editors
August 14–15, 2014
Philadephia, PA
www.ismte.org
6th Conference on Open Access
Scholarly Publishing
September 17–19, 2014
Paris, France
http://oaspa.org/
Council for Programs in Technical and Scientific
Communication
September 25–27, 2014
Colorado Springs, CO
www.cptsc.org/
Regulatory Affairs Professionals Society
September 27–October 1, 2014
Austin, TX
www.raps.org
National Association of Science Writers
October 17–21, 2014
Columbus, OH
http://nasw.org
New Horizons in Science
October 19–20, 2014
Columbus, OH
http://casw.org/
Health Literacy Annual Research Conference
November 3–4, 2014
Bethesda, MD
www.bumc.bu.edu/healthliteracyconference/
European Medical Writers Association
November 6–8, 2014
Florence, Italy
www.emwa.org
American Public Health Association
November 15–19, 2014
New Orleans, LA
www.apha.org/meetings/AnnualMeeting/
Calendar of Meetings

M
y philosophy of editing: What a big wide deep
topic, impossible to fully delve into in a few sen-
tences! The roots of those two words (the Greek
philos, beloved or loving, grafted onto sophia, knowledge,
learning, or wisdom, as applied to editus, the past participle
of the Latin verb meaning to publish or produce) are inex-
tricably tangled—tangled like the roots in the bottom of a
too-small terra cotta pot whose out-of-control plant is dying
for some help, in need of being lovingly and knowledgeably
cut apart and then transplanted into larger terrain. As a long-
time author’s editor at two major research-intensive medical
schools (the University of Minnesota in Minneapolis and the
University of Arizona in Tucson), I know that my job entails
loving knowledge or learning or wisdom enough to help cul-
tivate it into publishable form, to organically tend it (perhaps
to uproot parts of it) so that it produces its best flowering in
the appropriate target journal or textbook.
Note that I am not a journal editor, an acquisitions editor,
a rewrite editor, or even a copyeditor; basically, as an author’s
editor, I have no power whatsoever, other than the power
of persuasion. My substantive editing services are available
as a departmental asset that faculty and staff members, fel-
lows, and residents can ask to tap anytime, all at no charge
to themselves or their subdivisions; whether or not to accept
my suggestions is up to them. (They usually do, if their many
expressions of gratitude to me are any indication.)
To try to replant, into the rich soil of the wider scholarly
world, the manuscripts that typically overflow my surgery
department in-box, I don’t need my well-worn gardening
gloves or pointed trowel or watering can. To shake excess dirt
off the page, to divide and reassemble the cuttings so they
thrive, and to send the most healthily pruned specimens off
into the sunlight, I rely on my decades of experience in aca-
demia, on all those years of loving (the never-finished pur-
suit of) knowledge and learning and wisdom. The main tools
of my trade are my well-thumbed dictionaries and reference
books, my favorite journals (including the AMWA Journal,
the flagship New England Journal of Medicine, and College
Composition and Communication), and online research
resources like PubMed. Rather than a pointed trowel, I might
grab a pointed red felt-tip pen for proofs and other graphics-
heavy items that I then scan and send, but I typically wield a
Dell computer cursor, digging into sentences and vigorously
tilling them with bright-red track changes. My workplace
watering can takes the form of a warm-toned cover e-mail
to the lead author, in which I gently spray a light mist of sup-
port over those starkly embedded suggestions to securely
tamp them down, summarizing and explaining my edits, and
even more vitally, encouraging and thanking the author.
I am a writer, too; like nearly all of the authors I edit for,
I know what it’s like to be bruised by clueless, even cruel
reviewers and other uncaring gatekeepers. I want all authors
who seek my input to know that I am on their side, emphati-
cally yet empathetically rooting for the success of their intel-
lectual seedlings, the manuscripts that are the heartfelt
outgrowths of their hard ongoing work. Ultimately, each lead
author and I, as part of the same departmental team, are also
on the reader’s side (and, in the case of medical editing, on
the patient’s side as well).
The copious editorial suggestions that I unabashedly
shower on the near-final drafts of their manuscripts (and
elaborate on in my cover e-mail messages) are all grounded
in sound rhetorical principles and best practices aimed at
the sky of effective, efficient communication, with an unwilt-
By Mary E. Knatterud, PhD / St. Paul, MN
What is your philosophy of editing? We asked readers that question at the end of
Arnold Melnick’s article “Reject, Rewrite, or Edit” in the last issue of the journal.
sounding board
My Philosophy of Editing: Pruning and
Nurturing to Help Manuscripts Bloom
84 AMWA Journal / V29 N2 / 2014 / amwa.org

ing commitment to sow and nurture clarity, conciseness, con-
sistency, and connectedness. While respecting authors’ own
unique voice, I try to make sure that it doesn’t muddy readabil-
ity or trample up-to-date style conventions. Keeping the pri-
mary audience and specific genre firmly in view, I focus always
on painstakingly sharing my rigorous language-oriented
expertise as a wordsmith without inflicting inordinate pain
on the tender egos of my colleagues. Again, if unpersuaded by
any given change I offer up, they have the last word, along with
the byline. “Feel free to ignore any of my suggestions if they’re
not quite what you want or need,” I note in my cover e-mail.
“It is your paper, after all.” (I truly believe that even the most
confident surgeon-scientists have tender egos when it comes
to the personal craft of writing, even with regard to suppos-
edly “objective” research articles. I also believe that the tender
shoots of their manuscripts, whether overgrown or desic-
cated when they first land in my hands, almost always harbor
the promise of profusely blooming somewhere, of reaping the
rewards of publication someday, of somehow sprouting meta-
phoric wings. As lofty as all that sounds, I couldn’t get up in the
morning if I didn’t think what I do matters.)
If I had to distill my philosophy of editing into one word,
it would be kindness, directly and liberally rained down on
authors for the sake of readers and patients alike. Of course, I
show no kindness to grammatical errors, syntactic lapses, fac-
tual mistakes, and other distracting slip-ups but instead con-
sider it a kindness to meticulously weed them out—a kindness
to my authors, their readers, and patients everywhere. In the
epilogue to my 1997 doctoral dissertation, I quoted Aldous
Huxley, and his words still resonate, root and branch, with
me: “It’s a bit embarrassing to have been concerned with the
human problem all one’s life and find at the end that one has
no more to offer by way of advice than ‘try to be a little kinder.’”
Author contact: [email protected]
Mary E. Knatterud is an editor-educator at the University of Minnesota
in Minneapolis with three research-oriented departments: Surgery,
Urologic Surgery, and Otolaryngology. From October 2008 through
May 2014, she was an associate professor in the Department of Surgery
at the University of Arizona in Tucson (a telecommuting faculty posi-
tion based in her home office in St. Paul); before that, she worked at
the University of Minnesota for 30 years, including 21 years in the
Department of Surgery.
Her 1997 doctoral dissertation, First Do No Harm: Empathy and the
Writing of Medical Journal Articles, was published by Routledge (New
York and London) in 2002. Her work on medical communication has
appeared in Archives of Surgery, Science Editor, AMWA Journal, Obesity
Surgery, JAMA, Transplantation, Dialysis & Transplantation, and
Minnesota Physician, among other journals. Her poetry has appeared
in Annals of Emergency Medicine, The Pharos (the Alpha Omega Alpha
Honor Medical Society journal), and Harmony (the Arizona Health
Sciences Center medical humanities magazine), among other
publications.
SOUNDING BOARD
If I had to distill my philosophy
of editing into one word, it would
be kindness, directly and liberally
rained down on authors for the
sake of readers and patients alike.
AMWA Journal / V29 N2 / 2014 / amwa.org
85

86 AMWA Journal / V29 N2 / 2014 / amwa.org
M
edical communications are supposed to make
sense. Thus, one of a medical editor’s most impor-
tant responsibilities is to find and fix nonsensi-
cal sentences. Many different kinds of problems can cause a
sentence to be nonsensical. Some of these problems are syn-
tactical, which means that they arise from some flaw in the
grammatical structure of the sentence. Others are semantic,
which means that they arise from the meanings of the words.
In his 1957 book Syntactic Structures, Noam Chomsky pro-
vided a classic example of a sentence that makes no sense
even though it is grammatically correct:
F
Colorless green ideas sleep furiously.
The sentence is grammatical. It contains a noun phrase
that serves as a subject (colorless green ideas) and a verb
phrase that serves as a predicate (sleep furiously). The noun
in the subject phrase and the verb in the predicate phrase
even agree in number. Yet the phrase colorless green ideas
makes no sense. Ideas have no color. Even if they had a color,
they could not be colorless and green at the same time. Nor
does the predicate make sense. Ideas cannot sleep, and noth-
ing can sleep furiously.
When I am editing someone else’s writing or reviewing
my own, I analyze the sentences for semantic problems of
that kind. Do the noun-verb transactions make sense? Does
each modifier (ie, adjectival and adverbial elements) really
modify its head (the sentence element that it’s supposed to
be modifying)? In particular, I focus on each verb and think
about how it relates to each of its arguments and adjuncts.
The arguments of a verb are the nouns and noun phrases
that stand in some sort of relationship to a verb in a particu-
lar sentence: namely, the subject(s), direct object(s), and
indirect object(s) of the verb. A verb may also have adjuncts.
Adjuncts are sentence elements that are not structurally
necessary. In other words, the sentence would still qualify
as a complete, grammatical sentence if they were left out.
Nevertheless, they can provide some useful information.
Syntactic Structures
The syntactical arguments of a verb include the subject,
direct object, and indirect object. The adjuncts of a verb
include adverbial prepositional phrases and adverbial
clauses.
All verbs can have a subject. However, only transitive
verbs can take a direct object. Note that some verbs can be
used in a transitive or intransitive sense:
A
I eat. (In this sentence, eat is intransitive because there’s
no direct object.)
A
I eat cookies. (Here, eat is a transitive verb because there
is a direct object: cookies.)
The syntactical relationships are easily shown by dia-
gramming the sentence:
A good dictionary will tell you whether a verb can be
used in a transitive sense. If the dictionary lists a particu-
lar verb as only being intransitive, I avoid giving it a direct
object.
Verbs that can take an indirect object are sometimes
called dative verbs:
A
I sang to her.
Verbs that can take a direct and an indirect object are
called ditransitive verbs:
A
I gave him $20.
Laurie Endicott Thomas, MA, ELS
Colorless Green Ideas Sleep Furiously
I
eat
I
cookieseat
sang
I
her
to
gave
I
him
$20

AMWA Journal / V29 N2 / 2014 / amwa.org
87
There are also some tritransitive verbs, such as to trade,
which can take a direct object and two indirect objects:
A
I traded him my peanut butter sandwich for a Twinkie.
Semantic Structures
Linguists have come up with some terminology to describe
the semantic relationships between nouns and verbs. For
example, an agent is an entity that performs an action, and
a patient is an entity that undergoes an action. Note that the
agent of a verb is not necessarily the subject of the sentence.
Nor is the patient always the direct object. When the passive
voice is used, the patient is the subject of the verb and the
agent is in a prepositional phrase, if it is mentioned at all.
A
I broke the window. (Active voice: the agent is the subject
and the patient is the direct object.)
A
The window was broken [by me]. (Passive voice: the
patient is the subject and the agent can even be omitted.)
The table lists some common types of semantic arguments
and adjuncts, sorted according to their syntactical roles. Notice
that some of the arguments are subjects, direct objects, and
indirect objects, whereas the adjuncts are adverbial phrases or
adverbial clauses.
These terms are helpful in thinking about how a verb
relates to the nouns and adverbial elements in the sentence.
However, the boundaries between these terms are sometimes
hazy. For example, it may be hard to decide whether something
is a patient or a theme.
Verb Arguments
Careful writers and good editors think about whether the argu-
ment structure of each verb makes sense. For example, some
kinds of verbs can be performed by only certain kinds of sub-
jects. For example, an animal, an inanimate object, or a natural
event can kill you, but only another human being can murder
you. That’s because the word murder is defined as the unlawful
premeditated killing of one human being by another.
When I am writing or editing, I think about whether the
arguments of each verb make sense. Can the agent of that verb
really perform that action? If there is a direct object, is the verb
really transitive, and does that verb express something that is
really happening to that direct object? For help in making these
decisions, I often turn to the dictionary. Besides providing defi-
nitions of the words involved, dictionaries give you examples
of how those words are used. Often, those examples show the
kind of argument structures that are appropriate for particular
nouns and verbs.
Author contact: [email protected]
Subjects
Agent deliberately performs an action I spoke.
Force or natural cause mindlessly performs an action The wind blew.
Experiencer receives sensory or emotional input They suered.
Direct objects
Patient undergoes an action and changes its state I broke the window.
Theme undergoes an action but is not changed I gave him $20.
Indirect objects
Recipient someone or something that receives ownership I gave him $20.
Beneciary the entity for whose benet the action was per-
formed
I baked her a pie.
Adverbial phrases and clauses
Time when an action occurred The operation was performed on Tuesday.
Location where an action occurred The procedure was performed in the
examination room.
Source or origin where the action originated The foreign body was removed from his ear.
Direction or goal where the action is directed toward She was taken to the hospital.
Instrument something used to perform the action The incision was made with a scalpel.
Manner how some action was carried out The bill was sent to me in error.
Purpose why someone chose to do something She called to remind me about the
meeting.
Cause why an action occurred The ice in the freezer melted because the
power went out.

T
his slim volume begins with a refreshingly candid
assertion: The National Institutes of Health (NIH),
with more than 20 separate institutes and a multitude
of specialized offices, can be byzantine. Where the authors
take that premise, however, is less straightforward.
I was struck by this book’s title for two reasons. First,
this is the first I heard that the NIH could help me. Second,
although Dr Berg is a former “insider” (he used to run the
National Institute of General Medical Sciences), he no longer
works for the NIH. His coauthor is a grant writer and editor
who assists researchers with developing their applications.
Thus, neither one is an “insider.” Perhaps a picky distinction,
but one I returned to as I read the book.
As the opening paragraph suggests, this book has good
points. The Appendix is a 20-page treasure trove of URLs
and Web pages for a plethora of pieces, parts, and institutes
within the NIH. The introduction to the Appendix notes
that updated links and information can be found at Ms
Kienholz’s blog, thereby deftly addressing the top problem in
writing a how-to book about grant applications—timeliness
of information, especially online information. I also liked the
brief introduction, “Essential Steps for Securing NIH Grant
Funding: A Quick Guide to Key Concepts.” The 15 key con-
cepts are each linked to a chapter in the book, allowing read-
ers to browse based on their needs and interests.
And that leads me to a dreaded minefield in writing
about grants—abbreviations. After the “Essential Steps” sec-
tion, there is a four-page list of abbreviations that jumbles
together names of grant mechanisms, institutes, offices, and
miscellaneous terms—some arcane, some basic. It would be
churlish to blame the authors for the existence of all those
abbreviations. But who is the list for? Seasoned investiga-
tors won’t need it, and new ones will find it overwhelming. In
addition, there’s no need to memorize or highlight terms that
seem useful, because (mercifully) they are spelled out in the
text later on.
The first few chapters of the book delve into the struc-
ture of the NIH, which has the effect (as they say in the
newspaper business) of “burying the lede”—that is, keeping
the reader from getting to the good stuff. Nonetheless, as I
trudged through this material, I found a hidden gem: a clear,
two-page explanation of the NIH grant scoring system and
what the terms percentile, payline, and success rate mean.
This is something I’ve wanted to see for ages. But why put
this information before the key tips on how to write effec-
tively (chapters 8 and 9), when inexperienced grant writers
won’t know how to interpret it?
The puzzling organization of this book is its weakest
point. Why tell readers about their eRA Commons account
(the online “in box” for each principal investigator, which
includes self-populated demographic details, application
status updates, and reviewers’ critiques of submitted pro-
posals) on page 46, when it is not defined until page 68?
Why explain the mechanics of a grant review panel (called a
study section) and how to get on one, when less-experienced
investigators still don’t understand how to write for that
audience (again, chapters 8 and 9)? Why say that the project
summary section of a grant application is not “a throw-away
30 lines of text,” without ever saying that the summary is
limited to 30 lines in length? Why discuss the federal budget
process (chapter 5), over which the applicant has little con-
trol, before discussing how to talk to people within the NIH
structure who could help you (chapter 10)?
My biggest source of confusion with this book is who
the authors believed their audience was, since the infor-
mation, its organization, and degree of detail (lots in some
places, none in others) suggests different audiences at dif-
ferent times. This confusion is reflected in the title, where
I began: Few readers will think the NIH exists to help them
get money, rather than to improve public health through
research. A more accurate title would have been “How
Knowing More About the NIH Will Help Your Grant’s Chances
of Funding.” The nuggets tucked away in this book do serve
that purpose, and seasoned grant writers will appreciate
them; less-savvy ones will get lost in the welter of details and
miss the nuggets altogether.
Brevity doesn’t mean a guide to grant writing is subopti-
mal. My favorite is Guide to Effective Grant Writing: How to
Write a Successful NIH Grant Application, by Otto O. Yang,
which is only 100 pages long. But tastes and needs differ; do
some homework into the best guides, and choose based on
your background and needs.
—Karen Potvin Klein, MA, ELS
Karen Potvin Klein is the director of grant development and medi-
cal editing, Translational Science Institute, Wake Forest University
Health Sciences, Winston-Salem, North Carolina.
media reviews
How the NIH Can Help You Get Funded.
An Insider’s Guide to Grant Strategy
Michelle L. Kienholz and Jeremy M. Berg
New York, NY: Oxford University Press, 2014; 188 pp., $29.95
88 AMWA Journal / V29 N2 / 2014 / amwa.org

I
n a my last column, I made a promise to you that the volunteers
and staff at AMWA would continue to work tirelessly to ensure
AMWA remains relevant to our members, to our profession,
and to our industry. If only you could have seen that promise kept
in Bethesda, Maryland, this past April!
Our usual spring Executive Committee (EC) and Board of
Directors (BOD) meetings began in a very unusual way. On April
10, 2014, leaders of the American Medical Writers Association,
the Drug Information Association (DIA), the International Society
for Medical Publication Professionals (ISMPP), and the Society
for Technical Communication (STC) met for the first Medical
Communications Interorganizational Summit. The purposes of the
summit were to recognize the many similarities among the respec-
tive organizations; explore synergies that might benefit the organi-
zations and their members; discuss challenges facing the medical
communications industry, the organizations, and their members;
and identify opportunities to share resources and experiences that
can strengthen the organizations, benefit their members, and serve
their missions.
The participating organizations share certain core beliefs: a
commitment to integrity for the medical communications field
and to being leaders in promoting excellence, both within the
industry and to their members, by providing guidance and con-
tinuing education. All of the participating organizations are
nonprofit, membership-based organizations. They are rich in edu-
cational resources and content, and their members are collectively
involved in all aspects of medical communications.
Summit participants were particularly interested in exploring
how to share educational resources, capitalize on the use of social
media to further their missions, and advocate for best practices
and industry standards that uphold their common commitments
to integrity and excellence. They agreed to reconvene soon via
scheduled teleconferences to address these and other topics war-
ranting deeper discussion.
If this summit was the only reason for us to gather in Bethesda,
that would have been enough. But it was just the beginning. The
EC met to discuss AMWA’s finances, which are outstandingly
healthy, and to continue our strategic work in furthering AMWA’s
mission. The Nominating Committee presented an outstanding
slate of officers, which was then brought to the BOD the next day
for approval. Together, the EC and BOD took the next important
step forward in the certification process, and now we’re on our way
to securing a trademark for the designation successful candidates
will be able to place after their names. I am purposefully holding
off telling you what that designation is until we have cleared the
first hurdle at the US Patent and Trademark Office.
The EC and BOD also took an important step forward in our
commitment to developing a top-notch online education program
that will be second to none and worthy of the AMWA name. Our
staff at headquarters has been empowered to research and pres-
ent recommendations for a learning management system that will
open up the e-learning environment for whatever we want to do.
Online learning was a message heard loud and clear from the med-
ical communicator needs assessment survey AMWA conducted
last year, and we are making progress.
During the BOD meeting, chapter representatives spent a few
hours brainstorming solutions to common chapter challenges. A
lot of innovative solutions were discussed as ideas flowed freely
from chapter to chapter and from table to table. I believe all the
delegates were eager to get home to their chapters to discuss—and,
hopefully, implement—some of the great ideas that were shared.
The EC and BOD then devoted several additional hours to
brainstorming on another very important topic: how to pay for
all the exciting new programs and projects we have planned for
AMWA. As I mentioned earlier, AMWA is in a very healthy financial
state. We have the money we need to enable AMWA to keep doing
the great things we do now. But clearly, AMWA members want and
need more, and the medical communications field demands more
of its leading organization. It’s not a matter of saying “We can’t
afford to do these things.” Rather, it’s a matter of asking “How can
we afford to do these things?” The EC and BOD came up with flip
chart pages filled with ideas, and you will be hearing more about
these exciting developments in the coming months.
At the end of our first full day together, the EC and BOD cel-
ebrated with a little downtime and were treated to brief remarks by
the proposed slate of officers. I made a few brief remarks as well,
which I want to share with you here. I asked the board members to
look at the current EC members and proposed slate of new officers,
and realize we were once all in their shoes. We all started as mem-
bers, became involved at the chapter level, served on the BOD, and
joined the EC. What’s special about EC members is what’s special
about BOD members, is what’s special about many members: We
share a love for and commitment to AMWA. I encouraged every
BOD member to consider service on the EC in their future, just as
I encourage you now to get involved at the chapter level. You’ll be
amazed at where it can take you professionally and personally.
By Brian Bass / 2013–2014 AMWA President
Your AMWA at Work
amwa news
FROM THE PRESIDENT
AMWA Journal / V29 N2 / 2014 / amwa.org
89

Each year, the slate of AMWA officers is chosen by the
Nominating Committee, which consists of the president-
elect (who serves as chair) and six voting members who
are not members of the Executive Committee (EC). The
Nominating Committee receives from AMWA headquarters
the names and biographies of all members meeting the cri-
teria for the three elected offices: president-elect, secretary,
and treasurer. The EC interest form also was sent to quali-
fied candidates, giving them an opportunity to express their
interest in serving in an elected officer position. Members
of the Nominating Committee discuss the potential can-
didates and select one candidate for each position. The
names of these candidates are then presented to the Board
of Directors for approval at its spring meeting.
The following candidates were approved by the Board
of Directors at its spring 2014 meeting:
President-elect Stephen Palmer, PhD, ELS
Secretary Lori Alexander, MTPW, ELS
Treasurer Christine F. Wogan, MS, ELS
President: The president-
elect automatically assumes
the office of president at the
annual business meeting
held during the annual con-
ference of the following year.
The 2014–2015 AMWA presi-
dent will be Karen Potvin
Klein, MA, ELS, GPC. Karen
is director of grant develop-
ment and medical editing in
the Translational Science Institute at Wake Forest University
Health Sciences in Winston-Salem, North Carolina. She
earned an AB in classics from Brown University and an
MA in liberal studies from Wake Forest University. Karen
joined AMWA in 1989 and become a fellow in 2006. Karen
previously served AMWA in the elected office of secre-
tary; as administrator of special projects/communications,
awards, publications, and public relations; as Certification
Commission chair and job analysis panelist; in various
roles on committees and task forces, including chair and
member of the Eric Martin Award Committee, member
of the Budget and Finance Committee, and member of
the Task Force on Partnering with Higher Education; as a
roundtable, workshop and klatch leader; as open session
moderator and panelist; and as peer reviewer, editor, and
author of manuscripts for the AMWA Journal and reviewer
for Essays for Biomedical Communicators: Volume 2 of
Selected AMWA Workshops.
President-elect criteria: The president-elect (1) must have
served on the Executive Committee for a minimum of 2 full
years and (2) must be a current member of the Executive
Committee when his or her name is being considered by the
Nominating Committee.
Nominated for president-
elect is Stephen N. Palmer,
PhD, ELS. Steve is a senior
scientific medical writer at
the Texas Heart Institute
in Houston. He earned a
PhD in social and health
psychology at the State
University of New York
at Stony Brook, where he
also earned his MS. He
holds a BA from Wesleyan University. Steve joined AMWA
in 2002 and become a fellow in 2011. He is currently serv-
ing on the Executive Committee as secretary. His previ-
ous AMWA service includes the following: administrator
of awards, administrator of the annual conference, admin-
istrator of chapters and membership; annual conference
roundtable and klatch leader; open session leader and
speaker; member of many committees, including Medical
Book Awards and Constitution and Bylaws; and, for the
Southwest Chapter, program chair, president, immediate
past president, and board delegate.
amwa news
Slate of Candidates for 2014–2015 Election
90 AMWA Journal / V29 N2 / 2014 / amwa.org
Secretary criteria: The secretary must have served on
the Executive Committee within the 3 years immediately
preceding his or her consideration by the Nominating
Committee.
Nominated for secretary
is Lori Alexander, MPTW,
ELS. Lori is president of
Editorial Rx, Inc, an inde-
pendent medical writing
and publishing company
based in Orange Park,
Florida. Lori received a
bachelor’s degree in English
(concentration in journal-
ism) from the University of New Hampshire and a mas-
ter’s degree in technical and professional writing from
Northeastern University in Boston. Lori joined AMWA
in 1998, received the AMWA President’s Award in 2009,
and became a fellow in 2010. In 2012, she received a spe-
cial award for her 10 years of service as AMWA Journal
editor. Lori’s service to AMWA also includes: administra-
tor of the annual conference (twice); member of numer-
ous AMWA committees, including the job analysis and
item writing committees supporting the development
of medical writing certification; and annual conference
roundtable leader, open session moderator and speaker,
and workshop leader. Lori is a past president of the
Florida Chapter, and she coordinated several chapter
conferences for both the Mid-Atlantic and Florida
chapters.
Treasurer criteria: The treasurer must have served at
least 1 year on the Budget and Finance Committee within
the 5 years preceding his or her consideration by the
Nominating Committee. It is also desirable for the trea-
surer to have served on the Executive Committee before
assuming the office of treasurer.
amwa news
AMWA Journal / V29 N2 / 2014 / amwa.org 91
Nominated for treasurer
is Christine F. Wogan, MS,
ELS. Chris is publications
manager in the Division of
Radiation Oncology at the
MD Anderson Cancer Center
in Houston. She earned a
BA in biology at Swarthmore
College and an MS in bio-
logical sciences at the University of Houston at Clear
Lake. Chris joined AMWA in 1989 and received the AMWA
President’s Award in 2010. She was named a fellow in 2012.
Chris currently serves on the EC as treasurer. Her previ-
ous AMWA service includes the following: administrator of
awards; Journal peer reviewer; annual conference editing/
writing sections chair, workshop leader, open session pan-
elist and moderator, and roundtable leader; and, for the
Southwest Chapter, director-at-large, treasurer, president,
and immediate past president.
Procedure for Additional Nominations
According to AMWA’s bylaws (Article III.2d), additional
nominations for president-elect, secretary, or treasurer
may be made by any member whose dues and special
assessments are current, provided that any such nomina-
tion is submitted in writing to the secretary of AMWA at
least 30 days before the annual business meeting (which
will take place October 11, 2014, at the annual conference
in Memphis, Tennessee). Any individuals so nominated
must meet the criteria outlined in the bylaws (Article
III.1.a through 1.d) for their names to be placed on the
ballot. Such a nomination must clearly state the qualifica-
tions of the candidate, must be signed by 50 members in
good standing as of the date of the receipt of the nomina-
tion, and must be accompanied by a letter from the candi-
date stating that he or she is willing to serve if elected.

amwa news
The American Medical Writers Association (AMWA) operates
on a fiscal year from July 1 to June 30. At the end of the
fiscal year that ended June 30, 2013, AMWA had generated
$1,798,972 in revenue (including $105,199 in net investment
revenue) and $1,622,049 in expenses, for an increase in reve-
nue over expenses of $176,923.
Financial Performance Trends
The organization’s revenue sources for the fiscal years that
ended June 30, 2011, June 30, 2012, and June 30, 2013 (Figure 1),
reflect a stable organization, with more than 90% of revenues
coming from membership, the annual conference, and the cer-
tificate program.
A slight increase in membership dues each year accounts
for the revenue growth in that category. Revenue from the
annual conference remains relatively flat, but revenue from
the certificate program has shown a steady increase. The small
investment income in 2011–2012 reflects the market perfor-
mance during that period.
Expenses for 2012–2013 were lower than those of the previ-
ous year (Figure 2). The rise in expenses during 2011–2012 pri-
marily reflects development costs for the certification program
and a period of transition in which AMWA’s current execu-
tive director came onboard before the departure of the previ-
ous executive director to ensure the organization’s stability. In
2012–2013, despite increased investment in enhanced member
services and educational offerings, overall expenses declined
by 4.5% owing to restructuring of headquarters staff positions.
Major expense categories for AMWA are personnel, pro-
gram services, and supporting services (Figure 3). Personnel
costs reflect compensation for the AMWA headquarters staff.
Program services include the costs of all of the mission-based
activity of the organization, including the annual conference,
membership, the journal, online education, the certificate
program, and the certification program. Supporting services
are defined as administrative costs such as rent, telephone,
network systems and support, board meetings, insurance,
and supplies.
Figure 1. AMWA’s sources of revenue for the scal years that
ended June 30, 2013, June 30, 2012, and June 30, 2011, obtained
from the nancial statements for those years.
$0
$200,000
$400,000
$600,000
$800,000
Membership
Annual
Conference
Certicate
Program
Investments
Other
2010/2011
2011/2012
2012/2013
Figure 2. AMWA’s total expenses for the scal years that ended
June 30, 2013, June 30, 2012, and June 30, 2011, obtained from the
nancial statements for those years.
2010/2011
$0
$200,000
$400,000
$600,000
$800,000
$1,000,000
$1,200,000
$1,400,000
$1,600,000
$1,800,000
2011/2012 2012/2013
$1,523,894
$1,696,526
$1,622,049
By Christine F. Wogan, MS, ELS / 2013–2014 AMWA Treasurer and Publications Program Manager, Division of Radiation
Oncology, The University of Texas MD Anderson Cancer Center
American Medical Writers Association
Annual Financial Report, 2012–2013
92 AMWA Journal / V29 N2 / 2014 / amwa.org

Looking forward, AMWA continues to invest in products
and services that are of value to the medical writing commu-
nity. Our new association management software and web-
site improvements will enhance AMWA’s ability to meet the
needs of our members as well as those of other medical writ-
ers. Development of the certification program and enhanced
online education offerings will require a continued investment
of resources. Financial performance through the second quar-
ter of the current fiscal year (June 1, 2013, through December
31, 2013) is consistent with the budget and is expected to result
in a modest increase in the organization’s reserves.
Reserves
Reserves are the accumulation of funds over years to allow the
organization to withstand an emergency or to invest in new
programs. Unrestricted reserves of 6 to 12 months of annual
operating expenses are a standard target for not-for-profit
organizations. With budgeted annual operating expenses of
$1,816,285 for the current fiscal year (from July 1, 2013, to June
30, 2014), the target for AMWA’s reserves ranges from $908,142
to $1,816,285. AMWA’s current reserve level of $1,337,165 is
comfortably within this target range (Figure 4).
Financial Position
An organization’s financial position is reflected in its asset and
liability holdings (Figure 5). AMWA is well positioned to pay its
obligations and invest for the future. Total assets had grown to
$2,180,832 by June 30, 2013, and the organization’s liabilities
totaled $498,794. The vast majority of AMWA’s assets are liquid,
including cash, CDs, and mutual funds.
Conclusions
AMWA is in a stable financial position. The future of the orga-
nization is dependent on a stable membership base and
growth in our educational offerings. Targeted investment in
these areas began in fiscal year 2012–2013 and will continue
into fiscal 2015–2016.
Acknowledgment
I thank Vickie McCormick of Calibre CPA Group PLLC for provid-
ing the financial data and the 2012–2103 Budget and Finance
Committee members for their invaluable insights in their review of
reports and budgets: Mary Alice Ditzler, Jane Krauhs, Leslie Neistadt,
Judi Pepin, Alison Woo, and Jeanie Woodruff (and ex officio members
Brian Bass, Doug Haneline, and Susan Krug).
Author contact: [email protected]
Figure 3. AMWA’s expenses by major category for the scal
years that ended June 30, 2013, June 30, 2012, and June 30, 2011,
obtained from the nancial statements for those years.
$0
$200,000
$400,000
$600,000
$800,000
2010/2011
2011/2012
2012/2013
Personnel Program Services Supporting Services
Figure 4. AMWA’s unrestricted reserves for the scal years that
ended June 30, 2013, June 30, 2012, and June 30, 2011, obtained
from the nancial statements for those years.
2010/2011
$0
$400,000
$800,000
$1,200,000
$1,600,000
2011/2012 2012/2013
$1,228,779
$1,168,747
$1,337,165
Figure 5. AMWA’s total assets, by major category, and total
liabilities for the scal years that ended June 30, 2013, June 30,
2012, and June 30, 2011, obtained from the nancial statements
for those years.
2010/2011 2011/2012 2012/2013
$2,023,751
$2,131,801
$2,180,832
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$460,185
$626,686
$498,794
Cash CDs Mutual Funds Other Assets Liabilities
amwa news
AMWA Journal / V29 N2 / 2014 / amwa.org 93

During the past quarter, the Certification Commission
has continued to move closer to launching a certification
examination for medical communicators. The first exam
is on target to be given at the 2015 Annual Conference in
San Antonio, Texas.
The commission has completed a draft of the Policies
and Procedures Manual and Candidate Handbook and
will be finalizing these documents in the next quarter.
We anticipate that these materials and the examination
application will be available online in the first quarter
of 2015. The eligibility requirements for applying for the
examination were described previously in the AMWA
Journal [2014;29(1):47].
Bart Harvey, MD, PhD, who chairs the Examination
Development Committee, worked with the commission
this past quarter to define terms and responsibilities for
the committee. There will be seven to nine committee
members who represent a diversity of practice settings
and areas of skill and expertise in medical writing (eg,
regulatory writing, quantitative research methods, man-
uscript editing/writing, education, plain language, and
patient materials). The committee’s duties will include
By Thomas Gegeny, MS, ELS, and Marianne Mallia, ELS / 2014 Certication Commission Co-Chairs
AMWA has learned that Joseph H. Bloom, a long-time member, died June 26, 2013, at the age of
75 in Candler, North Carolina. He was a freelance writer who began his career in Philadelphia
and moved to the green hills of North Carolina in semi-retirement many years later. Joseph
joined AMWA in 1983 and was named a Fellow of AMWA in 1991. He served AMWA as presi-
dent of the Delaware Valley Chapter and was a board delegate from that chapter for a number
of years as well as a workshop leader at many conferences during the 1980s and 1990s. In 1994,
Joseph received the President’s Award, and from 1997 to 1999 he was administrator of chapters
on the Executive Committee. Joseph’s love of grand opera was legendary, and he was able to sing
selections from Wagner’s Die Meistersinger and other operas with aplomb. He is survived by his
wife, two sons, and two stepdaughters.
—Barbara C. Good, PhD
In Memoriam
Joseph H. Bloom
amwa news
Quarterly Update on Certication
Summer 2014
• Makingrecommendationsregardingthecertication
examination “blueprint” (ie, areas of knowledge, skills,
and abilities to be tested).
• Periodicallyreviewingandmakingrecommendations
regarding the list of resources suggested to candidates
for certification examination preparation.
• Developingitemsforinclusioninthecerticationexam-
ination item bank, especially in areas of the examination
blueprint that require additional items.
• Reviewingandprovidingfeedbackregardingproposed
and existing certification examination items.
• Recommendingitemstobeincludedinthecertication
examination.
• Reviewingitemperformanceonthecerticationexami-
nation (ie, item difficulty and item-total correlation) and
recommending any indicated item revisions.
Bart will also work with the consultant testing agency,
as needed, on tasks related to developing the certification
examination.
These are exciting times. Continue to watch for more
information about the certification exam in upcoming
AMWA Updates and in the AMWA Journal.
94 AMWA Journal / V29 N2 / 2014 / amwa.org

Writers Write.
So why not write for the AMWA Journal?
The Journal is seeking volunteers to cover speakers
and Open Sessions at the upcoming Annual
Conference. Volunteer by sending an e-mail to
AMWA Writers Write
for the AMWA Journal.
AMWA Journal / V29 N2 / 2014 / amwa.org
95
Explore New
Online Offerings
http://www.amwa.org/online_offerings
96 AMWA Journal / V29 N2 / 2014 / amwa.org
Unless otherwise noted, submit manuscripts and suggestions for
content to the Journal Editor at Jour[email protected].
FEATURE-LENGTH ARTICLES
Feature-length articles include topical features, original research in
medical communication, and Science Series articles.
Topical Features
The Journal accepts manuscripts on areas of interest to medical
communicators, including topics within such broad categories as
regulatory writing, continuing medical education, patient educa-
tion, medical marketing/advertising, public relations, medical jour-
nal management, publication ethics, health policy, etc. The Journal
especially encourages the submission of articles on the theoretical
underpinnings of specific types of medical communication. AMWA
Journal readers are primarily practitioners (not academicians),
and application of theory to practice is an essential component of
manuscripts. Word Count: 3,000 words (plus an informative abstract
of 250-300 words)
Original Research
The Journal accepts manuscripts reporting original research on
written communication, publication trends, and medical communi-
cators’ productivity and value added. Word Count: 3,000 words (plus
an informative abstract of 250-300 words)
Science Series
The Science Series accepts manuscripts that provide an overview of
a specific anatomic or physiologic topic (eg, body system), disease
or condition, diagnostic method (eg, laboratory tests, imaging
systems), or type of treatment (eg, devices). Submit manuscripts
for the Science Series to Randy Fritz, Science Series Editor, at fritz.
randall@mayo.edu. Word Count: 3,000 words (plus an informative
abstract of 250-300 words)
OTHER TYPES OF ARTICLES
Around the Career Block
The Around the Career Block section accepts manuscripts
that provide advice on career-related issues, profiles of professional
organizations, and first-person accounts of educational experiences.
Career-related Articles
These articles address topics that are relevant to the career
development of medical communicators. Areas of interest include
job hunting, developing a portfolio, interviewing techniques, hiring
guidance, performance evaluation, mentoring programs, perfor-
mance goals, etc. Word Count: 750-1,500 words
Profiles of Professional Organizations
These profiles help readers discover or better understand organiza-
tions that address specialty niches and may therefore be a useful
supplement to AMWA membership. Word Count: 600-1,000 words
First-person Accounts of Educational Programs
These articles provide overviews of educational programs designed
to enhance the knowledge and skills of medical writers and editors.
Word Count: 600-1,000 words
Commonplaces
Commonplaces is a new section devoted to the exchange of ideas
between teachers of medical communication and practitioners.
Contact Commonplaces Editor Lora Arduser (ar[email protected].
edu) with article ideas.
Media Reviews
The Media Reviews section includes reviews of books, CD-ROMs,
and videos that are of practical value or topical interest for medi-
cal writers and editors. Contact Book Reviews Editor Evelyn Kelly
([email protected]) if you wish to submit a book for review or wish
to write a review.
Practical Matters
The Practical Matters section accepts manuscripts that provide
practical guidance to medical writers and editors (at all levels of
experience) for improving the skills involved in their daily
work activities in a variety of medical communication settings.
Word Count: 750-1,800 words
Regulatory Insights
This section provides information of particular interest to commu-
nicators who write or edit documents related to the pharmaceutical
or device industries. Word Count: 750-2,000 words.
Social Media
The Social Media section includes articles focusing on the use
of social media and networking in the medical communication
industry. Send suggestions for topics to the appropriate Social
Media Section Editor: Cynthia L. Kryder ([email protected]),
general social media topics; Mali Schantz-Feld (mschantzfeld@
gmail.com), LinkedIn.
Tech Talk
The Tech Talk section includes articles about technology topics,
that may of interest to biomedical communicators. Word Count:
500-1,000 words.
OTHER SECTIONS
Member Musings
The Member Musings section is a forum for members to share
personal essays (related to medical writing and editing) and
creative work. Word Count: 500-750 words
Sounding Board
The Sounding Board is a forum for members’ opinions on topics
relevant to medical writing and editing. Contact the Journal
Editor to seek approval for the topic before preparing and
submitting a manuscript. Word Count: 750-1,000 words
Letters to the Editor
Letters to the Editor provide an opportunity to comment on topics
published in the Journal. Letters should refer to contents within the
past two issues. Word Count Limit: 500 words
MANUSCRIPT SUBMISSION
Manuscripts are accepted for consideration with the understand-
ing that they have not been published elsewhere and are not under
review elsewhere. Submit the manuscript as an attachment to an
e-mail note to the Journal Editor ([email protected]).
COPYRIGHT POLICY
The authors of manuscripts contained in the AMWA Journal grant
to AMWA exclusive worldwide first publication rights and further
grant a nonexclusive license for other uses of the manuscripts for
the duration of their copyright in all languages, throughout the
world, in all media. Copyright ownership of these articles remains
with the authors. Authors are asked to complete and sign a copy-
right form and submit it with their manuscript. (Forms are available
for manuscripts by a single author or multiple authors.)
Instructions for Contributors
��
For a more detailed version of the Instructions for Contributors, including
detailed content and formatting instructions, please visit www.amwa.org.

Certificate in Medical Writing and Editing
Develop the skills of top medical editors while learning to
organize and write well-structured articles.
Master biostatistics, charts, and computerized research.
Network with medical editors and prospective employers.
Writing and editing on medical topics, whether for professional or general
audiences, requires special knowledge and skills. In the Medical Writing
and Editing Certificate Program, you will learn the rules of scientific
evidence and medical nomenclature necessary for the construction of
academic articles, under the expert direction of senior-level medical
educators, writers, editors, and physicians.
Courses are oered in a time-ecient seminar format, meeting for three
consecutive days, or as three one-day courses.
Apply today.
grahamschool.uchicago.edu/MEAMWA
CLARITY IN.
JARGON OUT.

The AMWA Annual Conference is the ultimate resource for
medical communicators around the world, offering educational
and networking opportunities beyond compare in the field.
JOIN US
www.amwa.org/events_annual_conference
Registration opens in early July.
Early bird registration rates
available through August 30.
