
Guidelines on
Chronic
Pelvic Pain
D. Engeler (chairman), A.P. Baranowski, S. Elneil, J. Hughes,
E.J. Messelink, P. Oliveira, A. van Ophoven, A.C. de C. Williams
© European Association of Urology 2012

2 UPDATE FEBRUARY 2012
TABLE OF CONTENTS PAGE
1. INTRODUCTION 7
1.1 The Guideline 7
1.1.1 Panel composition 7
1.1.2 Publication history 7
1.2 Methodology 7
1.2.1 Level of evidence and grade of guideline recommendations* 8
1.2.2 Formal review 9
1.3 Acknowledgements 9
1.4 References 9
2. CHRONIC PELVIC PAIN 10
2.1 Introduction to chronic urogenital pain syndromes 10
2.2 Pain mechanisms - pain as a disease process 10
2.2.1 Ongoing peripheral visceral pain mechanisms as a cause of CPP 11
2.2.2 Central sensitisation - spinal and higher mechanisms of visceral pain 12
2.2.3 Spinal mechanisms and visceral hyperalgesia 12
2.2.4 Supraspinal modulation of pain perception 12
2.2.5 Higher centre modulation of spinal nociceptive pathways 12
2.2.6 Neuromodulation and psychology 13
2.2.7 Autonomic nervous system 13
2.2.8 Endocrine system 14
2.2.9 Genetics and chronic pain 14
2.3 Clinical paradigms and CPP 14
2.3.1 Referred pain 14
2.3.2 Referred pain to somatic tissues with hyperalgesia in the somatic tissues 14
2.3.3 Muscles and pelvic pain 14
2.3.4 Visceral hyperalgesia 14
2.3.5 Viscero-visceral hyperalgesia 15
2.4 Definitions of CPP terminology 15
2.4.1 Classification 15
2.4.2 Phenotyping 15
2.4.3 Terminology 15
2.4.4 Taxonomy 16
2.5 Classification of CPP syndromes 16
2.5.1 Importance of classification 16
2.5.2 IASP definitions 16
2.5.3 Pain syndromes 19
2.5.3.1 Definition of chronic pelvic pain (CPP) 19
2.5.3.2 Definition of chronic pelvic pain syndrome (CPPS) 19
2.5.3.2.1 Further subdivision of CPPS 19
2.5.3.2.2 Psychological considerations for classification 19
2.5.3.2.3 Functional considerations for classification 20
2.5.3.2.4 Multisystem subdivision 20
2.5.3.2.5 Dyspareunia 20
2.5.3.2.6 Perineal pain syndrome 20
2.6 Conclusions and recommendations: CPP and mechanisms 24
2.7 An algorithm for CPP diagnosis and treatment 24
2.8 References 26
3. UROLOGICAL ASPECTS OF CHRONIC PELVIC PAIN 28
3.1 Prostate pain syndrome (PPS) 28
3.1.1 Introduction 28
3.1.2 Definition 28
3.1.3 Pathogenesis 28
3.1.4 Epidemiology 28
3.1.5 Diagnosis 29
3.1.6 Conclusions and recommendations: assessment/diagnosis PPS 30
3.1.7 Treatment 30

UPDATE FEBRUARY 2012 3
3.1.7.1 Alpha-blockers 30
3.1.7.2 Antibiotic therapy 31
3.1.7.3 Anti-inflammatory drugs 31
3.1.7.4 Opioids 31
3.1.7.5 5-alpha-reductase inhibitors 31
3.1.7.6 Allopurinol 31
3.1.7.7 Phytotherapy 31
3.1.7.8 Pentosan polysulphate 32
3.1.7.9 Muscle relaxants 32
3.1.7.10 Pregabalin 32
3.1.7.11 Botulinum toxin A (BTX-A) 32
3.1.7.12 Physical treatments 32
3.1.7.13 Surgical management 32
3.1.7.14 Psychological treatment 32
3.1.8 Conclusions and recommendations: treatment of PPS 33
3.1.9 References 34
3.2 Bladder pain syndrome (BPS) 38
3.2.1 Introduction 38
3.2.2 Definition 39
3.2.3 Diagnosis 39
3.2.4 Pathogenesis 39
3.2.5 Epidemiology 40
3.2.6 References 40
3.2.7 Association with other diseases 45
3.2.8 Diagnosis 45
3.2.9 BPS in children and males 46
3.2.10 Conclusions and recommendations: assessment and diagnosis BPS 47
3.2.11 References 47
3.2.12 Medical treatment 50
3.2.12.1 References 52
3.2.13 Intravesical treatment 54
3.2.13.1 References 56
3.2.14 Interventional treatments 58
3.2.14.1 References 60
3.2.15 Treatments of limited efficacy and absence of recent publications 62
3.2.15.1 References 62
3.2.16 Non-pharmacological treatments 63
3.2.16.1 References 64
3.2.17 Surgical treatment 65
3.2.18 Conclusions and recommendations: treatment of BPS 67
3.2.19 References 70
3.3 Genital pain syndrome 72
3.3.1 Scrotal pain syndrome 72
3.3.2 Pathogenesis 72
3.3.2.1 Testicular pain syndrome 72
3.3.2.2 Epididymal pain syndrome 72
3.3.2.3 Nerves 72
3.3.2.4 Post-vasectomy pain syndrome 72
3.3.2.5 Post-inguinal hernia repair 73
3.3.2.6 Referred pain 73
3.3.3 Diagnosis 73
3.3.4 Treatment 73
3.3.4.1 Conservative treatment 73
3.3.4.2 Surgery 73
3.3.4.1.1 Microsurgical denervation 73
3.3.4.1.2 Epididymectomy 74
3.3.4.1.3 Orchiectomy 74
3.3.4.1.4 Vaso-vasostomy 74
3.3.5 Conclusions and recommendations: scrotal pain syndrome 74
3.3.6 References 75

4 UPDATE FEBRUARY 2012
3.4 Urethral pain syndrome 76
3.4.1 Definition 76
3.4.2 Pathogenesis 77
3.4.3 Treatment 77
3.4.4 Conclusions and recommendations: urethral pain syndrome 78
3.4.5 References 78
4. GYNAECOLOGICAL ASPECTS OF CHRONIC PELVIC PAIN 79
4.1 Introduction 79
4.2 Clinical history 79
4.3 Clinical examination 79
4.3.1 Investigations 79
4.4 Pain associated with well-defined conditions 80
4.4.1 Dysmenorrhoea 80
4.4.2 Infection 80
4.4.3 Endometriosis and adenomyosis 80
4.4.4 Gynaecological malignancy 81
4.4.5 Injuries related to childbirth 81
4.4.6 Pain associated with pelvic organ prolapse and prolapse surgery 81
4.5 Vaginal and vulvar pain syndromes 81
4.6 Summary 82
4.6.1 Conclusions and recommendations: gynaecological aspects of chronic
pelvic pain 82
4.7 References 83
5. GASTROINTESTINAL ASPECTS OF CHRONIC PELVIC PAIN 85
5.1 Introduction 85
5.2 Clinical history 85
5.2.1 Clinical examination and investigations 85
5.2.2 Diagnostic assessment 85
5.3 Pain associated with well-defined conditions 86
5.3.1 Haemorrhoids 86
5.3.2 Anal fissure 86
5.3.3 Proctitis 86
5.3.4 Constipation 86
5.4 Chronic anal pain syndrome 86
5.4.1 Diagnostic criteria for chronic anal pain syndrome 86
5.4.2 Botulinum toxin in pelvic pain 87
5.4.3 Intermittent chronic anal pain syndrome 87
5.5 Summary 87
5.5.1 Conclusions and recommendations: anorectal pain syndrome 88
5.6 References 89
6. PERIPHERAL NERVE PAIN SYNDROMES 90
6.1 Neuropathic pain 90
6.2 Anatomy 90
6.2.1 The anterior groin nerves 91
6.2.2 The posterior subgluteal triangle nerves 91
6.2.3 Branches of the pudendal nerve 91
6.2.4 Anatomical relations of the pudendal nerve (Figure 13) 91
6.2.5 Afferent nerves and the genitalia 92
6.2.6 Afferents in the autonomic plexus 93
6.3 Etiology of nerve damage 93
6.3.1 Anterior groin nerves - etiology of nerve damage 93
6.3.2 Pudendal neuralgia - etiology of nerve damage 93
6.3.3 Surgery 93
6.3.4 Trauma 93
6.3.5 Cancer 93
6.3.6 Birth Trauma 93
6.3.7 Elderly women 94

UPDATE FEBRUARY 2012 5
6.4 Diagnosis for pudendal neuralgia 94
6.4.1 Differential diagnosis of other disorders 94
6.4.2 Clinical presentation of pudendal neuralgia 94
6.4.2.1 Age 94
6.4.2.2 Sex 94
6.4.2.3 History 94
6.4.2.4 Associated features 95
6.4.2.5 Clinical examination 95
6.4.2.6 Investigations 95
6.5 Management of pain associated with nerve damage 96
6.5.1 Pudendal neuralgia and injections 95
6.5.2 Pudendal neuralgia and surgery 96
6.5.3 Pudendal neuralgia and neuromodulation 96
6.6 Conclusions and recommendations: peripheral nerve pain syndromes 96
6.7 References 97
7. SEXOLOGICAL ASPECTS OF CHRONIC PELVIC PAIN 100
7.1 Introduction 100
7.2 General Considerations 100
7.3 Pelvic floor involvement in sexual function and dysfunction 101
7.4 CPP and sexual dysfunction of the male 101
7.5 CPP and sexual dysfunction of the female 102
7.6 Treatment of sexual dysfunctions and CPP 103
7.7 In summary 103
7.8 Conclusions and recommendations: sexological aspects in CPP 104
7.9 References 104
8. PSYCHOLOGICAL ASPECTS OF CHRONIC PELVIC PAIN 109
8.1 Understanding the psychological components of pain 109
8.1.1 Neurophysiology of pain 109
8.1.2 Sexual abuse and trauma 109
8.1.3 Interpreting psychological differences 109
8.2 Psychological assessment of pain 110
8.3 Psychological issues in the treatment of pain 110
8.4 Female pelvic pain 111
8.4.1 Psychological risk factors in development and maintenance of pelvic pain 111
8.4.2 Psychological assessment of pelvic pain 111
8.4.3 Psychological factors in treatment of persistent pelvic pain 111
8.5 Conclusions and recommendations: psychological aspects of CPP 112
8.6 References 113
9. PELVIC FLOOR FUNCTION AND CHRONIC PELVIC PAIN 116
9.1 Introduction 116
9.2 Function 116
9.3 Dysfunction 116
9.4 Pelvic floor muscles and myofascial pain 117
9.4.1 Muscular aspects 117
9.4.2 Neurological aspects 117
9.4.3 Myofascial trigger points 117
9.5 Diagnostics of pelvic floor muscle function 117
9.5.1 Physical examination 118
9.5.2 Electromyography and pressure measurement (EMG) 118
9.5.3 Imaging 118
9.5.4 Myofascial trigger points 118
9.6 Treatment of pelvic floor muscle pain 118
9.6.1 Pelvic floor muscle exercise 118
9.6.2 Biofeedback and electrostimulation 118
9.6.3 Myofascial trigger point release 119
9.6.4 Botulinum A toxin 119
9.6.5 Pain management 119

6 UPDATE FEBRUARY 2012
9.7 Conclusions and recommendations: pelvic floor function 119
9.8 References 120
10. GENERAL TREATMENT OF CHRONIC PELVIC PAIN 122
10.1 Introduction 122
10.2 Simple analgesics 122
10.2.1 Antidepressants 123
10.2.1.1 Tricyclic antidepressants 123
10.2.1.2 Other antidepressants 123
10.2.2 Anticonvulsants 123
10.2.3 Other agents 124
10.3 Opioids 124
10.4.1 Recommendations for use of opioids in chronic/non-acute urogenital pain 125
10.4.2 Morphine 125
10.4.3 Other opioid agents 125
10.5 Nerve blocks 125
10.6 Transcutaneous electrical nerve stimulation (TENS) 126
10.7 Neuromodulation in pelvic pain syndromes 126
10.8 Summary 126
10.9 Recommendations for the medical treatment of CPP 127
10.10 References 128
11. ABBREVIATIONS USED IN THE TEXT 131

UPDATE FEBRUARY 2012 7
1. INTRODUCTION
1.1 The Guideline
Chronic pelvic pain (CPP) is a prevalent condition which can present a major challenge to health care providers
due to its complex aetiology and poor response to therapy.
Chronic pelvic pain is a multifactorial condition and therefore, quite often, poorly managed. Management
requires knowledge of all pelvic organ systems and their association with other systems and conditions,
including musculoskeletal, neurologic, urologic, gynaecologic and psychological aspects, promoting a
multidisciplinary approach.
The European Association of Urology (EAU) Guidelines Working Group for Chronic Pelvic Pain prepared
this guidelines document to assist urologists and medical professionals from associated specialties, such
as gynaecologists, psychologists, gastroenterologists and sexologists, in assessing the evidence-based
management of CPP and to incorporate evidence-based recommendations into their every-day clinical
practice.
1.1.1 Panel composition
The panel of experts responsible for this document include urologists, a neuro-urologist, consultants in pain
medicine, a gynaecologist, a psychologist, a gastroenterologist and a sexologist.
1.1.2 Publication history
The EAU Guidelines on Chronic Pelvic Pain were first published in 2003 (1) which formed the basis of a
scientific publication in European Urology in 2004 (2). Also, in the 2003 edition the concept of Chronic Pelvic
Pain Syndromes (CPPS) was introduced, which is now referred to as “pain as a disease process”.
Partial updates of the CPP guidelines were published in 2008 and formed the basis for another
scientific publication in European Urology in the year 2010 (3,4).
For this 2012 update the panel focused on:
1. restructuring the text to emphasise the significance of holistic management of CPP;
2. addressing the changes in the management of CPPS based on the concept of pain as a disease
process.
As a result, two new chapters have been added; Chapter 5 ‘Gastrointestinal aspects of chronic pelvic
pain’ and Chapter 7 ‘Sexological aspects of chronic pelvic pain.
A quick reference document presenting the main findings of these CPP guidelines (pocket guidelines) is also
available and has been updated. All texts, alongside scientific publications, can be viewed and downloaded for
personal use at the EAU website: http://www.uroweb.org/guidelines/online-guidelines/.
1.2 Methodology
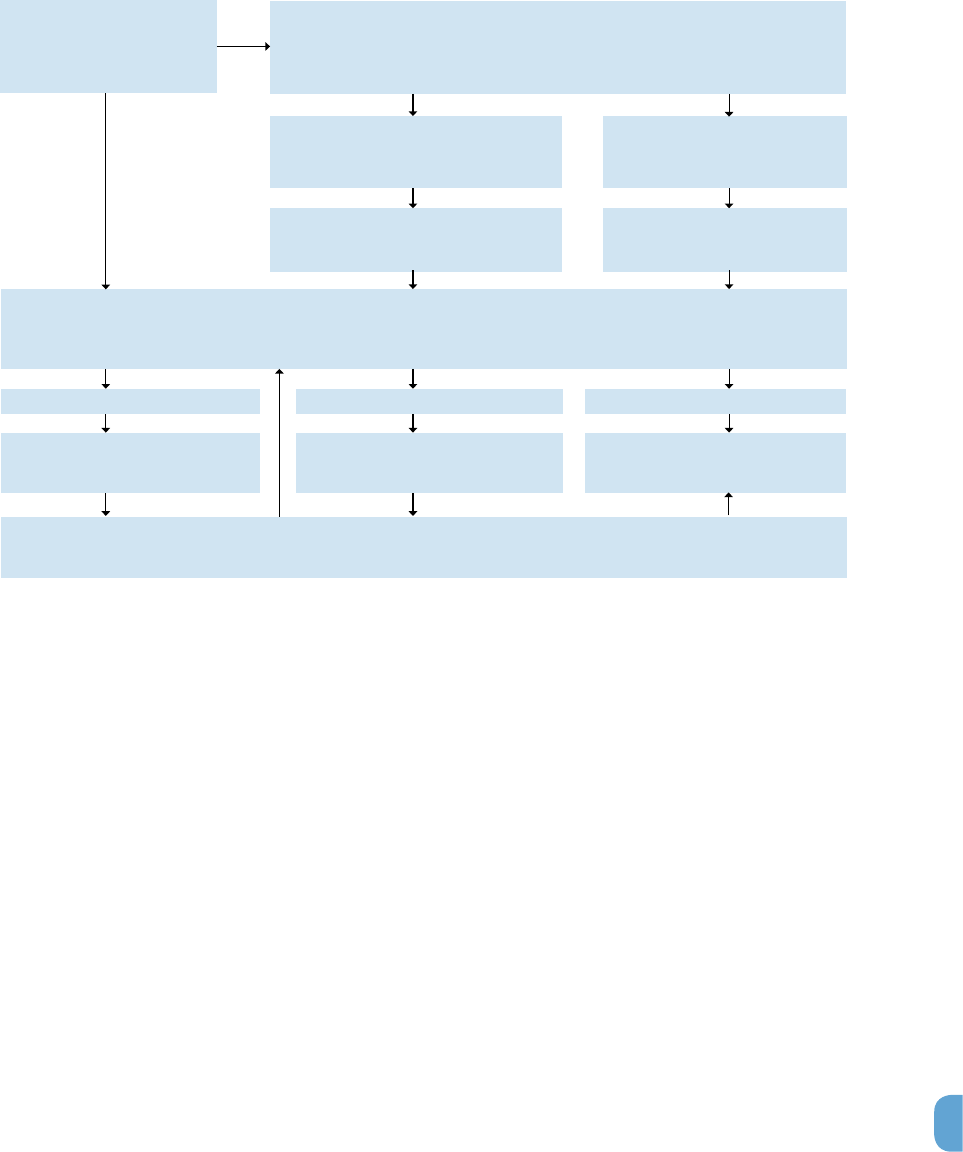
The full text update is based on a systematic review of literature using the Embase and Medline databases,
the Cochrane Central Register of controlled trials and the PsycInfo and Bandolier databases to identify the
best evidence from RCTs, Level of Evidence 1 (LE1), according to the rating schedule adapted from the
Oxford Centre for Evidence-based Medicine Levels of Evidence (Table 1) [5]. Where no LE1 literature could be
identified the search was moved down to the next lower level on the rating scale. Extensive use of free text
ensured the sensitivity of the searches, resulting in a substantial body of literature to scan. Searches covered
the period January 1995 and May 2011 and were restricted to English language publications.

8 UPDATE FEBRUARY 2012
Flowdiagram update procedure
1.2.1 Level of evidence and grade of guideline recommendations*
References used in the text have been assessed according to their level of evidence (Table 1), and
recommendations have been graded (Table 2) according to the Oxford Centre for Evidence-based Medicine
Levels of Evidence (5). The aim of grading recommendations is to provide transparency between the underlying
evidence and the recommendation given.
Table 1: Level of evidence (LE)*
Level Type of evidence
1a Evidence obtained from meta-analysis of randomised trials
1b Evidence obtained from at least one randomised trial
2a Evidence obtained from one well-designed controlled study without randomisation
2b Evidence obtained from at least one other type of well-designed quasi-experimental study
3 Evidence obtained from well-designed non-experimental studies, such as comparative studies,
correlation studies and case reports
4 Evidence obtained from expert committee reports or opinions or clinical experience of respected
Authorities
Modified from Sackett et al. (5)
It should be noted that when recommendations are graded, the link between the level of evidence and grade
of recommendation is not directly linear. Availability of randomised controlled trials (RCTs) may not necessarily
translate into a grade A recommendation where there are methodological limitations or disparity in published
results.
Alternatively, absence of high level evidence does not necessarily preclude a grade A
recommendation, if there is overwhelming clinical experience and consensus. In addition, there may be
exceptional situations where corroborating studies cannot be performed, perhaps for ethical or other reasons
and in this case unequivocal recommendations are considered helpful for the reader. The quality of the
underlying scientific evidence - although a very important factor - has to be balanced against benefits and
IdentificationScreeningEligibilityIncluded
Records identified through
database searching
(n = 9.399)
Records after duplicates
removed
(n = 8350)
Records screened
(n = 8350)
Full-text article assessed
for eligibility
(n = 732)
Studies included
(n = 471)
Records excluded
(n = 7618)

UPDATE FEBRUARY 2012 9
burdens, values and preferences and cost when a grade is assigned (6-8).
The EAU Guidelines Office, do not perform cost assessments, nor can they address local/national
preferences in a systematic fashion. But whenever this data is available, the expert panels will include the
information.
Table 2: Grade of recommendation (GR)*
Grade Nature of recommendations
A Based on clinical studies of good quality and consistency addressing the specific recommendations
and including at least one randomised trial
B Based on well-conducted clinical studies, but without randomised clinical trials
C Made despite the absence of directly applicable clinical studies of good quality
*Modified from Sackett et al. (5)
1.2.2 Formal review
A formal review was carried out prior to publication by a multidisciplinary team of international experts,
covering the different fields of expertise described in these guidelines.
1.3 Acknowledgements
The expert panel should like to express their gratitude to professor Magnus Fall, former chairman and patriarch
of the CPP panel who established the foundation of these guidelines, the current expert panel can now build
on.
Prof. Jan Borovicka, gastro-enterologist at the Kantonsspital St. Gallen, Switzerland, authored Chapter 5
‘Gastrointestinal aspects of chronic pelvic pain’ of this document.
Dr. Yacov Reisman, urologist at the Amstelland Hospital in Amstelveen and sexologist at the Academic Medical
Center in Amsterdam, the Netherlands, authored Chapter 7 ‘Sexological aspects of chronic pelvic pain’.
The CPP panel are most grateful for their assistance and willingness to lend their expertise to the EAU and their
Guidelines Office. Their input greatly enhance these guidelines.
The support provided by research scientist Drs. J. Krabshuis has proved to be highly valuable in enhancing the
methodological quality of this publication.
1.4 References
1. Fall M, Baranowksi AP, Fowler CJ, et al. EAU Guidelines on Chronic Pelvic Pain.
http://www.uroweb.org/guidelines/online-guidelines/
2. Fall M, Baranowski AP, Fowler CJ, et al. EAU Guidelines on Chronic Pelvic Pain. Eur Urol
2004;46:681-689.
http://www.uroweb.org/guidelines/online-guidelines/
3. Fall M, Baranowksi AP, Elneil S, et al. EAU Guidelines on Chronic Pelvic Pain 2010.
http://www.uroweb.org/guidelines/online-guidelines/
4. Fall M, Baranowski AP, Elneil S, et al. EAU guidelines on chronic pelvic pain.
Eur Urol. 2010 Jan;57(1):35-48
http://www.ncbi.nlm.nih.gov/pubmed/19733958
5. Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2009). Produced by Bob
Phillips, Chris Ball, Dave Sackett, Doug Badenoch, Sharon Straus, Brian Haynes, Martin Dawes since
November 1998. Updated by Jeremy Howick March 2009.
http://www.cebm.net/index.aspx?o=1025 [Access date January 2012]
6. Atkins D, Best D, Briss PA, et al; GRADE Working Group. Grading quality of evidence and strength of
recommendations. BMJ 2004 Jun 19;328(7454):1490.
http://www.ncbi.nlm.nih.gov/pubmed/15205295
7. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of
evidenceand strength of recommendations. BMJ 2008;336(7650):924-6.
http://www.ncbi.nlm.nih.gov/pubmed/18436948
8. Guyatt GH, Oxman AD, Kunz R, et al; GRADE Working Group. Going from evidence
torecommendations. BMJ 2008 May 10;336(7652):1049-51.
http://www.bmj.com/content/336/7652/1049.long

10 UPDATE FEBRUARY 2012
2. CHRONIC PELVIC PAIN
2.1 Introduction to chronic urogenital pain syndromes
Over the years much of the focus for CPP has been on peripheral-end-organ mechanisms, such as
inflammatory or infective conditions. However, both animal and clinical research have indicated that many
of the mechanisms for the CPP syndromes are based within the central nervous system (CNS). Although a
peripheral stimulus such as infection may initiate the start of a CPP condition, the condition may become self-
perpetuating as a result of CNS modulation, independent of the original cause. As well as pain, these central
mechanisms are associated with several other sensory, functional, behavioural and psychological phenomena.
It is this collection of phenomena that forms the basis of the pain syndrome diagnosis and individual
phenomena need to be addressed in their own right through multispecialty and multidisciplinary care.
Although ongoing peripheral organ pathology can produce persistent and chronic pain, the main focus of these
guidelines is on CPP syndromes in which no peripheral ongoing pathology (such as infection or neoplastic
disease) is detected. The main exception is when pain is due to peripheral nerve damage, which will be
discussed in chapter 6.
2.2 Pain mechanisms - pain as a disease process
Chronic pelvic pain mechanisms may involve:
1. Ongoing acute pain mechanisms (1) (such as those associated with inflammation or infection) - which
may involve somatic or visceral tissue.
2. Chronic pain mechanisms, which especially involve the CNS (2).
3. Emotional, cognitive, behavioural and sexual responses and mechanisms (3-6).These will be covered
in chapter 8.
Table 3 illustrates some of the differences between the somatic and visceral pain mechanisms. They underlie
some of the mechanisms that may produce the classical features of visceral pain; in particular, referred pain
and hyperalgesia.
Table 3: comparison between visceral and somatic pain
Visceral pain Somatic pain
Effective painful stimuli
Stretching and distension, producing
poorly localised pain.
Mechanical, thermal, chemical and
electrical stimuli, producing well
localised pain.
Summation
Widespread stimulation produces
significantly magnified pain.
Widespread stimulation produces a
modest increase in pain.
Autonomic involvement
Autonomic features (e.g., nausea and
sweating) frequently present.
Autonomic features less frequent.
Referred pain
Pain perceived at a site distant to the
cause of the pain is common.
Pain is relatively well localised but well
recognised.
Referred hyperalgesia
Referred cutaneous and muscle
hyperalgesia is common, as is
involvement of other visceral organs.
Hyperalgesia tends to be localised.
Innervation
Low density, unmyelinated C fibres
and thinly myelinated A∂ fibres.
Dense innervation with a wide range of
nerve fibres.
Primary afferent
physiology
Intensity coding. As stimulation
increases afferent firing increases with
an increase in sensation and ultimately
pain.
Two fibre coding. Separate fibres for
pain and normal sensation.
Silent afferents
50-90% of visceral afferents are silent
until the time they are switched on.
These fibres are very important in the
central sensitisation process.
Silent afferents present, but form a
lower percentage.

UPDATE FEBRUARY 2012 11
Central mechanisms
Play an important part in the
hyperalgesia, viscero-visceral, viscero-
muscular and musculo-visceral
hyperalgesia. Sensations not normally
perceived become perceived and non-
noxious sensations become painful.
Responsible for the allodynia and
hyperalgesia of chronic somatic pain.
Abnormalities of
function
Central mechanisms associated with
visceral pain may be responsible for
organ dysfunction.
Somatic pain associated with somatic
dysfunction, e.g., muscle spasm.
Central pathways and
representation
As well as classical pathways, there
is evidence for a separate dorsal horn
pathway and central representation.
Classical pain pathways.
2.2.1 Ongoing peripheral visceral pain mechanisms as a cause of CPP
In most cases of CPP, ongoing tissue trauma, inflammation or infection is not present (7-10). However,
conditions that produce recurrent trauma, infection or ongoing inflammation may result in CPP in a small
proportion of cases. It is for this reason that the early stages of assessment include looking for these
pathologies (11). Once excluded, ongoing investigations for these causes are rarely helpful and indeed may be
detrimental.
When acute pain mechanisms are activated by a nociceptive event, as well as direct activation of the peripheral
nociceptor transducers, sensitisation of those transducers may also occur, thus magnifying the afferent
signalling. Afferents that are not normally active may also become activated by the change, that is, there may
be activation of the so-called silent afferents. Although these are mechanisms of acute pain, the increased
afferent signalling is often a trigger for the chronic pain mechanisms that maintain the perception of pain in the
absence of ongoing peripheral pathology (see below) (12,13).
There are a number of mechanisms by which the peripheral transducers may exhibit an increase in sensibility.
1. Modification of the peripheral tissue, which may result in the transducers being more exposed to
peripheral stimulation.
2. There may be an increase in the chemicals that stimulates the receptors of the transducers (14).
3. There are many modifications in the receptors that result in them being more sensitive.
In general, the effect of 1 and 2 is to lower the threshold and the effect of 3 is to increase responsiveness to
external stimuli.
Some of the chemicals responsible for the above changes may be released from those cells
associated with inflammation, but the peripheral nervous system may also release chemicals in the form of
positive and inhibitory loops (Table 4) (15).
Table 4: mechanisms in the periphery that affect nociceptor response to a nociceptive stimulus
Nerve growth factor
(NGF)
May activate primary afferents directly, but also indirectly such as through
bradykinin (16). The result is an increase in response of the primary afferents, with
multiple action potentials being generated in response to a stimulus, as opposed
to just one or two. The TrkA-NGF complex formed on the afferent neurons may
also be transmitted centrally where it may alter gene expression. Such long-
term gene modification may underlie some of the mechanisms of chronic NGF-
induced hypersensitivity.
Adenosinetriphosphate
(ATP)
Is thought to be released in increased amounts from certain viscera when
stimulated by noxious stimuli. As well as this increased ATP producing an
increased stimulation of its receptors, when inflammation is present, the ATP
receptors have their properties changed so that there is an increased response
per unit of ATP contributing to the nociceptor activation. ATP is thought to act on
P2X3 purine receptors, which are found on visceral afferents and small-diameter
dorsal root ganglion (DRG) neurons.
Substance P and other
neurokinins (17)
Act on afferent tachykinin receptors, such as TRPV1, which is a transducer for
noxious heat and protons, and are thought to play a primary role in inflammatory
hyperalgesia.

12 UPDATE FEBRUARY 2012
Voltage-gated ion
channels
E.g., tetrodotoxin-resistant sodium channel, NaV1.8 are also implicated in
peripheral sensitisation. These channels open or close in response to changes
in membrane potential. Changes in potassium and calcium voltage-gated
channels may also underlie a part of the mechanism responsible for peripheral
sensitisation.
Second messenger
pathways
Within the primary afferents enable amplification of peripheral messages that they
receive. In general, these pathways are balanced by others that are responsible
for reducing any activation. During chronic pain, these mechanisms may become
imbalanced.
2.2.2 Central sensitisation - spinal and higher mechanisms of visceral pain
There are essentially three processes at the spinal cord level that are involved in central sensitisation (17).
Changes in existing protein activity (post-translational processing) are the earliest (within minutes); however,
changes in genetic transcription of proteins and even structural changes in neuron connectivity may also have
roles to play. These latter changes may occur within days (18).
The chemicals involved in the early phase include several neurotransmitters such as glutamate, substance P,
calcitonin gene-related peptide (CGRP), prostaglandin E2 and brain-derived neurotrophic factor (BDNF) (15).
Increased levels of glutamate, due to recurrent afferent nociceptive fibre activity, remove the magnesium
ion block of N-methyl-D-aspartate (NMDA). This allows calcium ions to enter the secondary afferents with
enhanced depolarisation. Glutamate also binds to amino-methylene-phosphonic acid (AMPA), which may be
another pathway by which it increases intracellular calcium. Other transmitters/modulators released centrally
include: substance P, which acts on neural kinin receptors; PGE2, which binds to endogenous prostanoid
receptors; and BDNF, which acts on tyrosine kinase B receptors and all of these may also increase intracellular
calcium.
The calcium ions act to lower the threshold for second-order neuron firing, with increased signalling being
transmitted to the higher centres. The second important feature of this increase in calcium ions is inpost-
translational processing; this usually involves the addition of phosphate groups to amino acids by kinases.
Phosphorylation can dramatically alter the properties of a protein, typically lowering the threshold at which
channels open, but also, the channels remain open for longer. The result is that a stimulus produces a
magnified evoked response in these neurons.
2.2.3 Spinal mechanisms and visceral hyperalgesia
Central sensitisation (18) is responsible for a decrease in threshold and increase in response duration and
magnitude of dorsal horn neurons. It is associated with an expansion of the receptive field. As a result,
sensitisation increases signalling to the CNS and amplifies what we perceive from a peripheral stimulus.
As an example, for cutaneous stimuli, light touch would not normally produce pain, however, when central
sensitisation is present, light touch may be perceived as painful (allodynia). In visceral hyperalgesia (so called
because the afferents are primarily small fibres), visceral stimuli that are normally subthreshold and not usually
perceived may be perceived. For instance, with central sensitisation, stimuli that are normally subthreshold
may result in a sensation of fullness and a need to void the bladder or to defecate. Stimuli normally perceived
may be interpreted as pain and stimuli that are normally noxious may be magnified (true hyperalgesia) with an
increased perception of pain. As a consequence, one can see that many of the symptoms of the bladder pain
syndrome (BPS) (formally known as interstitial cystitis (IC) and irritable bowel syndrome (IBS)) may be explained
by central sensitisation. A similar explanation exists for the muscle pain of fibromyalgia.
2.2.4 Supraspinal modulation of pain perception
It is important to appreciate that nociception is the process of transmitting to centres involved in perception
information about a stimulus that has the potential to cause tissue damage. Pain is far more complex and
involves activation of the nociceptive pathways but also the emotional response. Pain is defined by the
International Association for the Study of Pain (IASP) as “an unpleasant sensory and emotional experience
associated with actual or potential tissue damage, or described in terms of such damage” (19). The brain may
affect the modulation of pain pathways at the spinal cord level.
2.2.5 Higher centre modulation of spinal nociceptive pathways
It is now well accepted that there are both descending pain-inhibitory and descending pain-facilitatory
pathways that originate from the brain (20).

UPDATE FEBRUARY 2012 13
The midbrain periaqueductal grey (PAG) plays an important part in spinal modulation. It receives inputs from
centres associated with thought and emotion. Projections from the PAG (via several relay systems) to the
dorsal horn can inhibit nociceptive messages from reaching conscious perception by spinal mechanisms. The
PAG and its associated centres may also be involved in diffuse noxious inhibitory control (DNIC). DNIC is when
a nociceptive stimulus, in an area far from the receptive fields of a second nociceptive stimulus, can prevent or
reduce pain from that second area. This is thought to be the mechanism for the paradigm of counter-irritation.
Several neurotransmitters and neuromodulators are involved in descending pain-inhibitory pathways. The main
contenders are the opioids, 5-hydroxytryptamine and noradrenaline.
The pathways and chemicals for the facilitatory modulation are even less well understood, but the mechanisms
are well accepted.
2.2.6 Neuromodulation and psychology
Psychological processes of emotions, thought and behaviour involve networks rather than distinct centres.
Some of these processes are sophisticated and others fundamental in evolutionary terms, and their interaction
with pain processing is complex. As indicated above, many of the areas involved in relevant psychological
processes interact with the PAG, and this is therefore one mechanism by which they may influence pain
transmission at the spinal level.
At the spinal level, visceral nociception is dependent upon a system of intensity coding. In the viscera, primary
afferents for normal sensations and nociception appear to be the same small fibres arriving at the spinal cord,
and the difference between a normal and a noxious message depends upon the number of afferent signals
transmitted to the dorsal horn (as opposed to the dual fibre, A/C fibre for nociception and A for light touch,
seen in somatic tissue). It is thought that psychological modulation can alter intensity coding more easily than
dual-fibre coding, and hence, pain perception.
Various psychological processes affect pain neuromodulation at the higher level. Inhibiting or facilitating both
the nociceptive signal reaching the consciousness and appraisal and interpretation of that signal; they will
also modulate the response to the nociceptive message and hence the pain experience. Further, descending
pathways represent cognitive, emotional and behavioural states at spinal and peripheral levels.
Functional Magnetic Resonance Imaging (FMRI) has indicated that the psychological modulation of visceral
pain probably involves multiple pathways. For instance, mood and attentional focus probably act through
different areas of the brain when involved in reducing pain (21).
This psychological modulation may act to reduce nociception within a rapid time frame but may also
result in long-term vulnerability to chronic visceral pain, through long-term potentiation. This involvement
of higher centre learning may be at both a conscious and subconscious level, and is clearly significant in
the supratentorial neuroprocessing of nociception and pain. Long-term potentiation (22) may also occur at
any level within the nervous system, so that pathways for specific or combinations of stimuli may become
established, resulting in an individual being vulnerable to perceiving sensations that would not normally be
experienced as painful.
Stress is an intrinsic or extrinsic force that threatens the homeostasis of an organism and can be physical
or psychological. Stress induces an adaptive response that involves the endocrine, autonomic nervous and
immune systems, and these systems in turn appear to have feedback loops. Stress can modify the nervous
system by long-term potentiation so that there are long-term actual or potential changes within these
systems. It is this process that may be responsible for the effect of early life and significant adverse life events
associated with chronic pain syndromes. It is through all of these factors that stress can play a significant role
in nociceptive and pain neuromodulation, with the increased experience of pain as well as the more general
effect that stress may have on coping resources (23). Significant adverse life events include, rape, sexual
abuse, sexual trauma and sexual threat, such as during internment or torture. These events may produce long-
term physical changes in the CNS (biological response), as well as having an effect on a patient’s, emotional,
cognitive, behavioural and sexual responses (24-26).
2.2.7 Autonomic nervous system
The role of the autonomic nervous system in chronic pain is poorly understood, however, there is good
evidence that damaged afferent fibres may develop a sensitivity to sympathetic stimulation, both at the site of
injury and more centrally, particularly the dorsal horns. In visceral pain, the efferent output of the CNS may be

14 UPDATE FEBRUARY 2012
influenced by central changes (again, those changes may be throughout the neuraxis), and such modification
of the efferent message may produce significant end-organ dysfunction. These functional abnormalities can
have a significant effect on quality of life (QoL) and must be managed as appropriate.
2.2.8 Endocrine system
The endocrine system is involved in visceral function. Significant life events, and in particular, early life
events may alter the development of the hypothalamic-pituitary-adrenal axis and the chemicals released.
Increased vulnerability to stress may occur following such events and is thought to be partly due to increased
corticotrophin-releasing hormone (CRH) gene expression. Upregulation of CRH has been implicated in several
pain states such as rectal hypersensitivity to rectal distension. This model suggests an action of CRH on mast
cells.
A range of stress-related illnesses have been suggested, with IBS and BPS being examples. There is also
evidence accumulating to suggest that the sex hormones also modulate both nociception and pain perception.
2.2.9 Genetics and chronic pain
An individual who has had one chronic pain syndrome is more likely to develop another. Family clusters of
pain conditions are also observed and animals can be bred that are more prone to an apparent chronic pain
state. A whole range of genetic variations have been described that may explain the pain in certain cases;
many of these are to do with subtle changes in transmitters and their receptors. However, the picture is more
complicated in that development, environment and social factors also influence the situation.
2.3 Clinical paradigms and CPP
2.3.1 Referred pain
Referred pain is frequently observed and its identification is important for diagnosis and treatment. Referral
is usually somatic to somatic, or visceral to somatic. However, there is no reason why pain cannot also be
perceived within the area of an organ with the nociceptive signal having arisen from a somatic area. Referred
pain may occur as a result of several mechanisms but the main theory is one of convergence-projection. In the
convergence-projection theory, as an example, afferent fibres from the viscera and the somatic site of referred
pain converge onto the same second order projection neurons. The higher centres receiving messages from
these projection neurons are unable to separate the two possible sites from the origin of the nociceptive signal
(9,13,27).
2.3.2 Referred pain to somatic tissues with hyperalgesia in the somatic tissues
Hyperalgesia refers to an increased sensitivity to normally painful stimuli. In patients that have passed a renal
stone, somatic muscle hyperalgesia is frequently present, even a year after expulsion of the stone. Pain to
non-painful stimuli (allodynia) may also be present in certain individuals. Somatic tissue hyperaesthesia is
associated with urinary and bilary colic, IBS, endometriosis, dysmenorrhoea, and recurrent bladder infection.
Vulvar pain syndromes are examples of cutaneous allodynia that, in certain cases, may be associated with
visceral pain syndromes, such as BPS. Referred pain with hyperalgesia is thought to be due to central
sensitisation of the converging viscero-somatic neurones. Central sensitisation also stimulates efferent activity
that could explain the trophic changes that are often found in the somatic tissues.
2.3.3 Muscles and pelvic pain
In the urogenital pain syndromes muscle tenderness and trigger points may be implicated as a source of pain.
Central mechanisms are of great importance in the pathogenesis of this muscle hyperalgesia. The muscles
involved may be a part of the spinal, abdominal or pelvic complex of muscles. It is not unknown for adjacent
muscles of the lower limbs and the thorax to become involved. Pain may be localised to the trigger points
but is more often associated with classical referral patterns. As well as trigger points, inflammation of the
attachments to the bones (enthesitis) and of the bursa (bursitis) may be found (28-30).
Certain postures affect the different muscles in different ways, and as a consequence, may exacerbate or
reduce the pain. Stress has been implicated as both an initiator of pelvic myalgia and as a maintenance factor.
As a result, negative sexual encounters may also have a precipitating effect (23).
2.3.4 Visceral hyperalgesia
The increased perception of stimuli in the viscera is known as visceral hyperalgesia, and the underlying
mechanisms are thought to be responsible for IBS, BPS and dysmenorrhoea. The mechanisms involved are
often acute afferent input (e.g., due to infection) followed by long-term central sensitisation.
UPDATE FEBRUARY 2012 15
2.3.5 Viscero-visceral hyperalgesia
Viscero-visceral hyperalgesia is thought to be due to two or more organs with converging sensory projections
and central sensitisation. For instance, overlap of bladder and uterine afferents or uterine and colon afferents.
Figure 1: Predisposing factors, cause, central en peripheral mechanisms
2.4 Definitions of CPP terminology
2.4.1 Classification
Much debate over the classification of CPP has occurred, is ongoing and will continue in the future.
Classification involves three aspects of defining a condition, phenotyping, terminology and taxonomy.
2.4.2 Phenotyping
Phenotyping is describing the condition. For example, chronic bladder pain may be associated with the
presence of Hunner’s ulcers and glomerulation on cystoscopy, whereas other bladder pain conditions may
have a normal appearance on cystoscopy. These are two different phenotypes. The same is true for IBS,
which may be subdivided into that with primarily diarrhoea or that with constipation. Phenotyping is based
upon mechanisms when they are known (e.g., infection, ischaemic, autoimmune, or neuropathic). In the
absence of well-defined mechanisms, describing the condition by its symptoms, signs and, where possible, by
investigations, has been demonstrated to have clinical and research validity in many situations. When pain is
the main symptom and pain as a disease process is considered the cause, the condition is often referred to as
a pain syndrome - a well-defined collection of symptoms, signs and investigation results associated with pain
mechanisms and pain perception as the primary complaint.
2.4.3 Terminology
Terminology is the words that are used within classification, both to name the phenotype and within the
definition of the phenotype. Examples of names for phenotypes associated with the bladder include interstitial
cystitis, painful bladder syndrome or BPS. The EAU, the International Society for the study of BPS (ESSIC),
the International Association for the Study of Pain (IASP) and several other groups now prefer the term
bladder pain syndrome. In the pain syndromes, the role of the nervous system in generating the sensations is
thought to be pivotal, but the term syndrome is also holistic and takes into account the emotional, cognitive,
behavioural, sexual and functional consequences of the chronic pain.
When defining the phenotype, the terminology used in that definition must also be clear and if necessary
defined. One of the most important guiding principles is that spurious terminology should be avoided. Terms
that end in “itis” in particular should be avoided unless infection and or inflammation is proven and considered
Causes
surgery
trauma
infection
Peripheral nerve injury
Abnormal peripheral afferent signalling
Peripheral sensitisation
Increased peripheral afferent
signalling
Central sensitisation
Regional and systemic changes
Referred pain, viscero-visceral hyperalgesia, viscero-somatic hyperalgesia. Trophic, autonomic, endocrine and immunological responses
Abnormal central afferent signalling
Consequences include:
sensory problems
Abnormal central efferent signalling
Consequences include:
changes in organ function
Abnormal central processing
Psychological, behavioural and sexual
consequences
Predisposing factors
genetics
psychological state
recurrent somatic trauma

16 UPDATE FEBRUARY 2012
to be the cause of the pain (7). It must be appreciated that end-organ inflammation may be secondary and
neurogenic in origin and not a primary cause of the pain.
2.4.4 Taxonomy
Taxonomy places the phenotypes into a relationship hierarchy. The EAU approach subdivides CPP into
conditions that are pain syndromes and those that are non-pain syndromes. The latter are conditions that have
well-recognised pathology (e.g., infection, neuropathy or inflammation), whereas the former syndromes do not
and pain as a disease process is the mechanism. Other terms for the non-pain syndromes include “classical
conditions”, “well-defined conditions” and “confusable diseases”. Although the EAU approach deals primarily
with urological conditions, this approach to classification can be applied to all conditions associated with pain
perception within the pelvis; the classification has been developed to include non-urological pain and was
accepted by the IASP for publication in January 2012.
2.5 Classification of CPP syndromes
2.5.1 Importance of classification
It should be obvious to all that a condition cannot be treated unless it is defined. However, the reasons for
classifying CPP go far beyond that.
Clues to the mechanism
As a result of systematic phenotypic and taxonomic classification, similarities and differences between
conditions become clear. Drawing comparisons between the phenotypes of different disorders allows one to
compare disorders such as bladder and bowel pain syndromes, thus facilitating research and treatment.
Guidelines for best treatment options
As conditions become better defined, more specific treatment approaches can be adopted. In particular, there
will be a move away from treatments based upon spurious terms (e.g., antibiotics and non-steroidal anti-
inflammatory drugs for the “-itis” conditions). Generic treatments aimed at groups of conditions will be more
commonplace and based upon research evidence.
Research platform
Only by clearly defining the phenotype being investigated can research be valued or applied in the clinical
situation.
Patient needs
A diagnosis, or name, for a set of symptoms can provide patients with a sense of being understood, as well
as hope for relief. It may therefore help in acceptance of the problem as chronic, resolution of unfounded
fears about its implications (if not life-threatening), and engagement in therapeutic endeavours, as well as in
self-management. However, it may also lead to accessing information of variable quality associated with the
diagnosis or name, and the possibility of generating new concerns about long term consequences or about
appropriateness of treatment.
Remuneration
In certain countries, having a defined condition is necessary for the patient to receive treatment for their
condition.
2.5.2 IASP definitions
Subdividing pain syndromes
There is much debate on the subdivisions of the pain syndromes within the hierarchical taxonomy. The EAU
has led the way in this regard and the guiding principles are as follows (31):
1. The pain syndromes are defined by a process of exclusion. In particular, there should be no evidence
of infection or inflammation. Investigations by end-organ specialists should thus be aimed at obtaining
a differential diagnosis; repeated, unnecessary investigations are detrimental in the management of
chronic pain syndromes.
2. A subdivision phenotype should only be used if there is adequate evidence to support its use. For
instance, in non-specific, poorly localised pelvic pain without obvious pathology, only the term chronic
pelvic pain syndrome (CPPS) should be used. If the pain can be localised to an organ, then a more
specific term, such as rectal pain syndrome, may be used. If the pain is localised to multiple organs,
then the syndrome is a regional pain syndrome and the term CPPS should once again be considered.
As well as defining the patient by a specific end-organ phenotype, there are several other more
general descriptors that need to be considered. These are primarily psychological (e.g., cognitive

UPDATE FEBRUARY 2012 17
or emotional), sexual, behavioural and functional. Psychological and behavioural factors are well
established to relate to QoL issues and prognosis. In North America a research programme, the MAPP
program (Multi-disciplinary Approach to the study of chronic Pelvic Pain research) has been devised
to investigate the importance of these factors and looks at all types of pelvic pain irrespective of the
end-organ where the pain is perceived. It also looks at systemic disorder associations, such as the
co-ocurrence of fibromyalgia, facial pain, or autoimmune disorders.
3. In 2004 this expert panel introduced the concept of managing the polysymptomatic nature of CPP,
since then others have developed their own schemes, such as Nickel’s UPOINT (32), modified by
Magri et al. (33). In the light of these and other publications, the symptom classification table has been
updated (Table 5).
The debate in relation to subdividing the pain syndromes remains ongoing. As more information is collected
suggesting that the CNS is involved, and indeed may be the main cause of many CPP conditions (e.g., bladder,
genitalia, colorectal or myofascial), there is a general tendency to move away from end-organ nomenclature.
Whether this is appropriate, only time and good research will tell. To enable such research, it is essential to
have a framework of classification within which to work. Any hierarchical taxonomy must be flexible to allow
change.
In table 5 the classification has been set up according to the axis system used by IASP. The panel used this
table from their first edition and found it very useful for clinical purpose.

18 UPDATE FEBRUARY 2012
Table 5: EAU classification of chronic urogenital pain syndromes
Axis I
Region
Axis II
System
Axis III
End organ as pain sundrome as
identified from Hx, Ex and Ix
Axis IV
Referral
characteristics
Axis V
Temporal
characteristics
Axis VI
Character
Axis VII
Associated
symptoms
Axis VIII
Psychological
symptoms
Chronic
pelvic
pain
Specific disease
associated pelvic
pain
OR
Pelvic pain
syndrome
Urological Prostate Suprapubic
Inguinal
Urethral
Penile/clitoral
Perineal
Rectal
Back
Buttocks
Thighs
ONSET
Acute
Chronic
ONGOING
Sporadic
Cyclical
Continuous
TIME
Filling Emptying
Immediate post
Late post
TRIGGER
Provoked Spontaneous
Aching
Burning
Stabbing
Electric
UROLOGICAL
Frequency
Nocturia
Hesitance
Dysfunctional flow
Urge
Incontinence
GYNAECOLOGICAL
Menstrual
Menopause
GASTROINTESTINAL
Constipation
Diarrhoea
Bloatedness
Urge
Incontinence
NEUROLOGICAL
Dysaesthesia
Hyperaesthesia
Allodynia
Hyperalegesie
SEXUOLOGICAL
Satisfaction
Female dyspareunia
Sexual avoidance
Erectile dysfunction
Medication
MUSCLE
Function impairment
Fasciculation
CUTANEOUS
Trophic changes
Sensory changes
ANXIETY
About pain
or putative
cause of pain
Catastrophic thinking about pain
DEPRESSION
Attributed to
pain or impact
of pain
Attributed to
other causes
Unattributed
PTSD
SYMPTOMS
Re-experiencing
Avoidance
Bladder
Scrotal
Testicular
Epididymal
Penile
Urethral
Post-vasectomy
Gynaecological Vulvar
Vestibular
Clitoral
Endometriosis associated
CPPS with cyclical exacerbations
Dysmenorrhoea
Gastrointestinal Irritable blowel
Chronic anal
Intermittent chronic anal
Peripheral nervers Pudendal pain syndrome
Sexological Dyspareunia
Pelvic pain with sexual dysfunction
Psychological Any pelvic organ
Musculo-skeletal Pelvic floor muscle
Abdominal muscle
Spinal
Coccyx

UPDATE FEBRUARY 2012 19
2.5.3 Pain syndromes
The original EAU classification (31) was inspired by the IASP classification (19) and much work around what
has become known as “pain as a disease” and its associated psychological, behavioural, sexual and functional
correlates. After 10 years work developing the initial ideas an updated version was accepted by IASP Council
for publication January 2012.
2.5.3.1 Definition of chronic pelvic pain (CPP)
Chronic pelvic pain is chronic or persistent pain perceived* in structures related to the pelvis of either men or
women. It is often associated with negative cognitive, behavioural, sexual and emotional consequences as well
as with symptoms suggestive of lower urinary tract, sexual, bowel, pelvic floor or gynaecological dysfunction.
[*Perceived indicates that the patient and clinician, to the best of their ability from the history, examination and
investigations (where appropriate) has localised the pain as being perceived in the specified anatomical pelvic
area].
In the case of documented nociceptive pain that becomes chronic/persistent through time, pain must have
been continuous or recurrent for at least 6 months. That is, it can be cyclical over a 6-month period, such as
the cyclical pain of dysmenorrhoea. Six months is arbitrary, however, it was chosen because 3 months was
not considered long enough if we include cyclical pain conditions. If non-acute and central sensitisation pain
mechanisms are well documented, then the pain may be regarded as chronic, irrespective of the time period.
Cyclical pain is included in the classification and hence dysmenorrhoea needs to be considered as a chronic
pain syndrome if it is persistent and associated with negative cognitive, behavioural, sexual, or emotional
consequences.
Chronic pelvic pain may be subdivided into conditions with well-defined classical pathology (such as infection
or cancer) and those with no obvious pathology. For the purpose of this classification, the term “specific
disease-associated pelvic pain” is proposed for the former, and “chronic pelvic pain syndrome” for the latter.
The following classification only deals with CPPS.
2.5.3.2 Definition of chronic pelvic pain syndrome
Chronic pelvic pain syndrome (CPPS) is the occurrence of CPP when there is no proven infection or other
obvious local pathology that may account for the pain. It is often associated with negative cognitive,
behavioural, sexual or emotional consequences, as well as with symptoms suggestive of lower urinary tract,
sexual, bowel or gynaecological dysfunction. CPPS is a subdivision of CPP.
2.5.3.2.1 Further subdivision of CPPS
Pain perception in CPPS may be focused within a single organ, more than one pelvic organ and even
associated with systemic symptoms such as chronic fatigue syndrome, fibromyalgia or Sjögren’s syndrome.
When the pain is localised to a single organ, some specialists may wish to consider using an end-organ term
such as BPS (Table 6). The use of such a phrase with the terminology “syndrome” indicates that, although
peripheral mechanisms may exist, CNS neuromodulation may be more important and systemic associations
may occur. When the pain is localised to more than one organ site, the term CPPS should be used. Many,
including some of the authors of this text, never subdivide by anatomy and prefer to refer to patients with
pain perceived within the pelvis and no specific disease process as suffering from CPPS, subdivided by
psychological and functional symptoms.
2.5.3.2.2 Psychological considerations for classification
Many CPPSs are associated with a range of concurrent negative psychological, behavioural and sexual
consequences that must be described and assessed. Examples that need to be considered are depression,
anxiety, fears about pain or its implications, unhelpful coping strategies, and distress in relationships.
Both anxiety and depression can be significant important concomitant symptoms that are relevant to pain,
disability and poor QoL. Catastrophic interpretation of pain has been shown to be a particularly salient
variable, predicting patients’ report of pain, disability, and poor QoL, over and above psychosocial variables
such as depression or behavioural factors such as self-reported sexual dysfunction. It is suggested that
CPPS sometimes creates a sense of helplessness that can be reported as overwhelming, and may be
associated with the refractory nature of the patients’ symptoms. It is important to note that many of these
biopsychosocial consequences are common to other persistent pain problems but may show varying degrees
of salience for any one individual suffering from CPPS. In all patients with CPPS, these consequences must
be clearly described as part of the phenotype (where the term phenotype is used to indicate the observable
Axis I
Region
Axis II
System
Axis III
End organ as pain sundrome as
identified from Hx, Ex and Ix
Axis IV
Referral
characteristics
Axis V
Temporal
characteristics
Axis VI
Character
Axis VII
Associated
symptoms
Axis VIII
Psychological
symptoms
Chronic
pelvic
pain
Specific disease
associated pelvic
pain
OR
Pelvic pain
syndrome
Urological Prostate Suprapubic
Inguinal
Urethral
Penile/clitoral
Perineal
Rectal
Back
Buttocks
Thighs
ONSET
Acute
Chronic
ONGOING
Sporadic
Cyclical
Continuous
TIME
Filling Emptying
Immediate post
Late post
TRIGGER
Provoked Spontaneous
Aching
Burning
Stabbing
Electric
UROLOGICAL
Frequency
Nocturia
Hesitance
Dysfunctional flow
Urge
Incontinence
GYNAECOLOGICAL
Menstrual
Menopause
GASTROINTESTINAL
Constipation
Diarrhoea
Bloatedness
Urge
Incontinence
NEUROLOGICAL
Dysaesthesia
Hyperaesthesia
Allodynia
Hyperalegesie
SEXUOLOGICAL
Satisfaction
Female dyspareunia
Sexual avoidance
Erectile dysfunction
Medication
MUSCLE
Function impairment
Fasciculation
CUTANEOUS
Trophic changes
Sensory changes
ANXIETY
About pain
or putative
cause of pain
Catastrophic thinking about pain
DEPRESSION
Attributed to
pain or impact
of pain
Attributed to
other causes
Unattributed
PTSD
SYMPTOMS
Re-experiencing
Avoidance
Bladder
Scrotal
Testicular
Epididymal
Penile
Urethral
Post-vasectomy
Gynaecological Vulvar
Vestibular
Clitoral
Endometriosis associated
CPPS with cyclical exacerbations
Dysmenorrhoea
Gastrointestinal Irritable blowel
Chronic anal
Intermittent chronic anal
Peripheral nervers Pudendal pain syndrome
Sexological Dyspareunia
Pelvic pain with sexual dysfunction
Psychological Any pelvic organ
Musculo-skeletal Pelvic floor muscle
Abdominal muscle
Spinal
Coccyx

20 UPDATE FEBRUARY 2012
characteristics of the syndrome).
2.5.3.2.3 Functional considerations for classification
Functional disorders, for the purpose of this document, are pathologies that have arisen secondary to changes
in the control mechanisms of an organ or system. That is they are disorders characterised by disturbance of
function. As an example, slow colonic transit is a functional disorder of the bowel - the normal function of the
bowel is not occurring as a result of changes in the mechanisms that produce defecation, and hence the bowel
control is abnormal. The term is not used in the sense of a psychiatric functional disorder. Many CPPSs are
associated with functional abnormalities at a local and even systemic level. These also need to be defined as a
part of the phenotype.
Functional pain disorders may not express significant pathology in the organs that appear responsible
for the primary symptoms, but they are associated with substantial neurobiological, physiological and
sometimes anatomical changes in the CNS.
2.5.3.2.4 Multisystem subdivision
It is recognised that the end-organ where the pain is perceived may not be the centre of pain generation. This
classification is based upon the most effective accepted method of classifying and identifying different pain
syndromes, that is, by site of presentation. It is argued that keeping the end-organ name in the classification
is inappropriate because, in most cases, there are multisystemic causes and effects, with the result that
symptoms are perceived in several areas. This is an area in which discussions are ongoing, and despite there
being strong arguments for both keeping and dispensing with end-organ classification, the authors have not
taken the umbrella approach of referring to all pain perceived in the pelvis as CPPS.
2.5.3.2.5 Dyspareunia
Dyspareunia is defined as pain perceived within the pelvis associated with penetrative sex. It tells us nothing
about the mechanism and may be applied to women and men. It is usually applied to penile penetration, but is
often associated with pain during insertion of any object. It may apply to anal as well as vaginal intercourse. It
is classically subdivided into superficial and deep.
2.5.3.2.6 Perineal pain syndrome
Perineal pain syndrome is a neuropathic-type pain that is perceived in the distribution area of the pudendal
nerve, and may be associated with symptoms and signs of rectal, urinary tract or sexual dysfunction. There is
no proven obvious pathology. It is often associated with negative cognitive, behavioural, sexual and emotional
consequences, as well as with symptoms suggestive of lower urinary tract, sexual, bowel or gynaecological
dysfunction.
Perineal pain syndrome should be distinguished from pudendal neuralgia, which is a specific disease
associated with pelvic pain that is caused by nerve damage.
UPDATE FEBRUARY 2012 21
Table 6: Urological pain syndromes
Urological Pain Syndromes - Chapter 3
Prostate pain
syndrome
PPS is the occurrence of persistent or recurrent episodic pain (which is convincingly
reproduced by prostate palpation). There is no proven infection or other obvious local
pathology. PPS is often associated with negative cognitive, behavioural, sexual or
emotional consequences, as well as with symptoms suggestive of lower urinary tract
and sexual dysfunction.
The term “chronic prostatitis” continues to be equated with that of PPS. In the
author’s and others’ opinion, this is an inappropriate term, although it is recognised
that it has a long history of use. The National Institutes of Health (NIH) consensus (34)
includes infection (types I and II), which the authors feel should not be considered
under PPS, but as specific disease-associated pelvic pain. The term prostadynia has
also been used in the past but is no longer recommended by the expert panel. Please
note that some of the authors of the IASP document disagree with this term and
suggest that CPPS of the male is used instead of PPS, which has been agreed by the
majority.
Bladder pain
syndrome
BPS is the occurrence of persistent or recurrent pain perceived in the urinary bladder
region, accompanied by at least one other symptom, such as pain worsening with
bladder filling and day-time and/or night-time urinary frequency. There is no proven
infection or other obvious local pathology. BPS is often associated with negative
cognitive, behavioural, sexual or emotional consequences, as well as with symptoms
suggestive of lower urinary tract and sexual dysfunction.
BPS is believed to represent a heterogeneous spectrum of disorders. There may
be specific types of inflammation as a feature in subsets of patients. Localisation
of the pain can be difficult by examination, and consequently, another localising
symptom is required. Cystoscopy with hydrodistension and biopsy may be indicated
to define phenotypes. Recently, ESSIC has suggested a standardised scheme of
subclassifications (11) to acknowledge differences and make it easier to compare
various studies.
Other terms that have been used include “interstitial cystitis”, “painful bladder
syndrome”, and “PBS/IC” or “BPS/IC”; these terms are no longer recommended.
Scrotal pain
syndrome
Scrotal pain syndrome is the occurrence of persistent or recurrent episodic pain
localised within the organs of the scrotum, and may be associated with symptoms
suggestive of urinary tract or sexual dysfunction. There is no proven infection or other
obvious local pathology. Scrotal pain syndrome is often associated with negative
cognitive, behavioural, sexual or emotional consequences, as well as with symptoms
suggestive of lower urinary tract and sexual dysfunction.
Scrotal pain syndrome is a generic term and is used when the site of the pain is not
clearly testicular or epididymal. The pain is not in the skin of the scrotum as such, but
perceived within its contents, in a similar way to idiopathic chest pain.
Testicular pain
syndrome
Testicular pain syndrome is the occurrence of persistent or recurrent episodic pain
perceived in the testes, and may be associated with symptoms suggestive of urinary
tract or sexual dysfunction. There is no proven infection or other obvious local
pathology. Testicular pain syndrome is often associated with negative cognitive,
behavioural, sexual or emotional consequences, as well as with symptoms suggestive
of lower urinary tract and sexual dysfunction.
Previous terms have included orchitis, orchialgia and orchiodynia. These terms are no
longer recommended.
Epididymal pain
syndrome
Epididymal pain syndrome is the occurrence of persistent or recurrent episodic pain
perceived in the epididymis, and may be associated with symptoms suggestive of
urinary tract or sexual dysfunction. There is no proven infection or other obvious local
pathology. Epididymal pain syndrome is often associated with negative cognitive,
behavioural, sexual or emotional consequences, as well as with symptoms suggestive
of lower urinary tract and sexual dysfunction.
22 UPDATE FEBRUARY 2012
Penile pain
syndrome
Penile pain syndrome is the occurrence of pain within the penis that is not primarily
in the urethra, in the absence of proven infection or other obvious local pathology.
Penile pain syndrome is often associated with negative cognitive, behavioural, sexual
or emotional consequences, as well as with symptoms suggestive of lower urinary
tract and sexual dysfunction.
Urethral pain
syndrome
Urethral pain syndrome is the occurrence of chronic or recurrent episodic pain
perceived in the urethra, in the absence of proven infection or other obvious local
pathology. Urethral pain syndrome is often associated with negative cognitive,
behavioural, sexual or emotional consequences, as well as with symptoms suggestive
of lower urinary tract, sexual, bowel or gynaecological dysfunction.
Urethral pain syndrome may occur in men and women.
Postvasectomy
scrotal pain
syndrome
Postvasectomy scrotal pain syndrome is a scrotal pain syndrome that follows
vasectomy. Postvasectomy scrotal pain syndrome is often associated with negative
cognitive, behavioural, sexual or emotional consequences, as well as with symptoms
suggestive of lower urinary tract and sexual dysfunction.
Postvasectomy pain may be as frequent as 1% following vasectomy, possibly more
frequent. The mechanisms are poorly understood and it is for that reason considered
a special form of scrotal pain syndrome.
Gynaecological Pain Syndromes: external genitalia - Chapter 4
Vulvar pain
syndrome
Vulvar pain syndrome is the occurrence of persistent or recurrent episodic vulvar pain.
There is no proven infection or other local obvious pathology. It is often associated
with negative cognitive, behavioural, sexual or emotional consequences, as well as
with symptoms suggestive of lower urinary tract, sexual, bowel or gynaecological
dysfunction.
Although pain perceived in the vulva was subsumed under sexual disorders in the
DSM-IV-R manual for classifying psychiatric disorders, there is no scientific basis
for this classification, and pain perceived in the vulva is best understood as a pain
problem that usually has psychological consequences. There is no evidence for its
classification as a psychiatric disorder.
The International Society for the Study of Vulvovaginal Disease (ISSVD) has used
the term vulvodynia, where we use the term vulvar pain syndrome. According to the
ISSVD, vulvodynia is vulvar pain that is not accounted for by any physical findings.
The ISSVD has defined vulvodynia as “vulvar discomfort, most often described
as burning pain, occurring in the absence of relevant visible findings or a specific,
clinically identifiable, neurologic disorder”. If physical findings are present, the patient
is said to have vulvar pain due to a specified cause. The ISSVD has subdivided
vulvodynia based on pain location and temporal characteristics of the pain (e.g.,
provoked or unprovoked). The following definitions are based on that approach.
Generalised vulvar
pain syndrome
Generalised vulvar pain syndrome refers to a vulvar pain syndrome in which the pain/
burning cannot be consistently and precisely localised by point-pressure mapping
via probing with a cotton-tipped applicator or similar instrument. Rather, the pain
is diffuse and affects all parts of the vulva. The vulvar vestibule (the part that lies
between the labia minora into which the urethral meatus and vaginal introitus open)
may be involved but the discomfort is not limited to the vestibule. This pain syndrome
is often associated with negative cognitive, behavioural, sexual or emotional
consequences. Previous terms have included “dysesthetic vulvodynia” and “essential
vulvodynia”, but are no longer recommended.
Localised vulvar
pain syndrome
Localised vulvar pain syndrome refers to pain that can be consistently and precisely
localised by point-pressure mapping to one or more portions of the vulva. Clinically,
the pain usually occurs as a result of provocation (touch, pressure or friction).
Localised vulvar pain syndrome can be subdivided into vestibular pain syndrome and
clitoral pain syndrome.
Vestibular pain
syndrome
Vestibular pain syndrome refers to pain that can be localised by point-pressure
mapping to the vestibule or is well perceived in the area of the vestibule.
Clitoral pain
syndrome
Clitoral pain syndrome refers to pain that can be localised by point-pressure mapping
to the clitoris or is well perceived in the area of the clitoris.
Gynaecological system: internal pelvic pain syndromes - Chapter 4.

UPDATE FEBRUARY 2012 23
Endometriosis-
associated pain
syndrome
Endometriosis-associated pain syndrome is chronic or recurrent pelvic pain in
patients with laparoscopically confirmed endometriosis, and the term is used
when the symptoms persist despite adequate endometriosis treatment. It is often
associated with negative cognitive, behavioural, sexual or emotional consequences,
as well as with symptoms suggestive of lower urinary tract, sexual, bowel or
gynaecological dysfunction.
Many patients have pain above and beyond the endometriotic lesions; this term is
used to cover that group of patients. Endometriosis may be an incidental finding,
is not always painful, and the degree of disease seen laparoscopically does not
correlate with severity of symptoms. As with other patients, they often have more
than one end-organ involved. It has been suggested that this phenotype should be
removed from the classification because the endometriosis may be irrelevant.
CPPS with cyclical
exacerbations
CPPS with cyclical exacerbations covers the non-gynaecological organ pain that
frequently shows cyclical exacerbations (e.g., IBS or BPS) as well as pain similar to
that associated with endometriosis/adenomyosis but where no pathology is identified.
This condition is different from dysmenorrhoea, in which pain is only present with
menstruation.
Dysmenorrhoea Dysmenorrhoea is pain with menstruation that is not associated with well-defined
pathology. Dysmenorrhoea needs to be considered as a chronic pain syndrome if it
is persistent and associated with negative cognitive, behavioural, sexual or emotional
consequences.
Musculoskeletal System - Chapter 9
Pelvic floor muscle
pain syndrome
Pelvic floor muscle pain syndrome is the occurrence of persistent or recurrent
episodic pelvic floor pain. There is no proven well-defined local pathology. It is often
associated with negative cognitive, behavioural, sexual or emotional consequences,
as well as with symptoms suggestive of lower urinary tract, sexual, bowel or
gynaecological dysfunction.
This syndrome may be associated with overactivity of or trigger points within the
pelvic floor muscles. Trigger points may also be found in several muscles, such as the
abdominal, thigh and paraspinal muscles and even those not directly related to the
pelvis.
Coccyx pain
syndrome
Coccyx pain syndrome is the occurrence of chronic or recurrent episodic pain
perceived in the region of the coccyx, in the absence of proven infection or other
obvious local pathology. Coccyx pain syndrome is often associated with negative
cognitive, behavioural, sexual or emotional consequences, as well as with symptoms
suggestive of lower urinary tract, sexual, bowel or gynaecological dysfunction. The
term “coccydynia” was used but is no longer recommended.
Gastrointestinal Pelvic Pain Syndromes - Chapter 5
Irritable bowel
syndrome
IBS is the occurrence of chronic or recurrent episodic pain perceived in the bowel, in
the absence of proven infection or other obvious local pathology. Bowel dysfunction
is frequent. IBS is often associated with worry and preoccupation about bowel
function, and negative cognitive, behavioural, sexual or emotional consequences,
as well as with symptoms suggestive of lower urinary tract or gynaecological
dysfunction.
The above classification is based upon the Rome III Criteria (35): 3 months of
continuous or recurring symptoms of abdominal pain or irritation that may be relieved
with a bowel movement, may be coupled with a change in frequency, or may be
related to a change in stool consistency.
Two or more of the following are present at least 25% of the time: change in stool
frequency (> 3 bowel movements per day or < 3 per week); noticeable difference in
stool form (hard, loose, watery or poorly formed stools); passage of mucus in stools;
bloating or feeling of abdominal distension; or altered stool passage (e.g., sensation
of incomplete evacuation, straining, or urgency). Extra-intestinal symptoms include:
nausea, fatigue, full sensation after even a small meal, and vomiting.

24 UPDATE FEBRUARY 2012
Chronic anal pain
syndrome
Chronic anal pain syndrome is the occurrence of chronic or recurrent episodic pain
perceived in the anus, in the absence of proven infection or other obvious local
pathology. Chronic anal pain syndrome is often associated with negative cognitive,
behavioural, sexual or emotional consequences, as well as with symptoms suggestive
of lower urinary tract, sexual, bowel or gynaecological dysfunction.
Intermittent chronic
anal pain syndrome
Intermittent chronic anal pain syndrome refers to severe, brief, episodic pain that
seems to arise in the rectum or anal canal and occurs at irregular intervals. This
is unrelated to the need to or the process of defecation. It may be considered a
subgroup of the chronic anal pain syndromes. It was previously known as “proctalgia
fugax”; this term is no longer recommended.
2.6 Conclusions and recommendations: CPP and mechanisms
Conclusions LE
CPPS mechanisms are well defined and involve mechanisms of neuroplasticity and neuropathic pain. 2
The mechanisms of neuroplasticity and neuropathic pain result in increased perception of afferent
stimuli which may produce abnormal sensations as well as pain.
1
End-organ function can also be altered by the mechanisms of neuroplasticity and neuropathic pain,
so that symptoms of function can also occur.
1
CPP is associated with a high impact on QoL. 1
The diagnosis of a CPPS as a pain syndrome is essential as it encourages a holistic approach to
management with multispecialty and multidisciplinary care.
2
Recommendations GR
All of those involved in the management of CPP should have an understanding and training in CPPS
pain mechanisms.
A
The early assessment of patients should involve not only investigations aimed at specific disease-
associated pelvic pain but also assessment of functional, emotional, behavioural, sexual and other
quality of life issues, such as effect on work and socialisation.*
A
CPPS patients should be managed in a multispecialty and multidisciplinary environment with
consideration of all their symptoms.
A
Future classification should involve consideration of all three recommendations above. A
CPP = chronic pelvic pain; CPPS = chronic pelvic pain syndrome.
* Instruments for assessment see Chapter 8.
2.7 An algorithm for CPP diagnosis and treatment
The algorithm for diagnosing and treating CPP (Figure 2) has been developed to guide a physician through
the process from diagnosis to management. A physician should follow the lines by answering the appropriate
questions with yes or no. By doing this the clinician will end up at a box that refers to the chapter in this
guideline that contains all the information needed.
Because CPP is pain perceived in structures related to the pelvis, it is necessary to approach a
patient diagnosed with CPP as a chronic pain patient. Confining the diagnosis to a specific organ may overlook
multisystem functional abnormalities requiring individual treatment and general aspects of pain in planning
investigation and treatment. This idea is easily recognised in the algorithm where the division in specific
disease associated pain is made on one hand and pelvic pain syndrome on the other.
The algorithm also illustrates that the authors advocate early involvement of a multidisciplinary pain
team. In practice, this should mean that well-known diseases, e.g. ‘true’ cystitis and endometriosis, will be
diagnosed and treated early. If treating such conditions does not reduce symptoms, or such well-defined
conditions are not found, then further investigation may be necessary, depending on where the pain is
localised.
Every chapter of this guideline shows specific algorithms that assist the clinician in decision making.
It should be noted, however, that over-investigation may be as harmful as not performing appropriate
investigations. The EAU algorithms introduce the concept of the ‘minimum investigations’ required to exclude a
well-defined condition.

UPDATE FEBRUARY 2012 25
Figure 2: an algorithm for diagnosing and managing CPP
Figure 3: an algorithm for pain management
Chronic Pelvic Pain
History
Physical
examination
see chapter 3 see chapter 4 see chapter 5 see chapter 7
Organ specific symptoms present
urology gynaecology gastro-enterology sexology
Treat according to specific
disease guidelines
Symptom of a well known
disease
Go to: Pain management
Specific disease associated pelvic pain
Pelvic pain syndrome
see chapter 9
pelvic floor
yes
no
yes
neurology
see chapter 6
no
Holistic approach
Psychology
Pain management
Physiotherapy Pain medicine
see chapter 8 see chapter 9
see chapter 10
Multidisciplinary team

26 UPDATE FEBRUARY 2012
Figure 4: phenotyping and assessment algorithm for CPP
2.8 References
1. Linley JE, Rose K, Ooi L, et al. Understanding inflammatory pain: ion channels contributing to acute
and chronic nociception. Pflugers Arch. 2010 Apr;459(5):657-69
http://www.ncbi.nlm.nih.gov/pubmed/20162302
2. McMahon SB, Dmitrieva N, Koltzenburg M, et al. Visceral pain. Br J Anaesth 75(2):132-144.
http://www.ncbi.nlm.nih.gov/pubmed/7577247
3. Bergeron S, Khalifé S, Glazer HI, et al. Surgical and behavioral treatments for vestibulodynia: two-and-
one-half year follow-up and predictors of outcome. Obstet Gynecol. 2008 Jan;111(1):159-66.
http://www.ncbi.nlm.nih.gov/pubmed/18165405
4. Tripp DA, Nickel JC, Wang Y, et al. Catastrophizing and pain-contingent rest predict patient
adjustment in men with chronic prostatitis/chronic pelvic pain syndrome. J Pain. 2006 Oct;7(10):
697-708.
http://www.ncbi.nlm.nih.gov/pubmed/17018330
5. Tripp DA, Nickel JC, Fitzgerald MP, et al. Sexual functioning, catastrophizing, depression, and pain, as
predictors of quality of life in women with interstitial cystitis/painful bladder syndrome. Urology. 2009
May;73(5):987-92.
http://www.ncbi.nlm.nih.gov/pubmed/19394494
6. Nickel JC, Tripp DA, Pontari M, et al. Psychosocial phenotyping in women with interstitial cystitis/
painful bladder syndrome: a case control study. J Urol. 2010 Jan;183(1):167-72.
http://www.ncbi.nlm.nih.gov/pubmed/19913812
7. Abrams PA, Baranowski AP, Berger RE, et al. A new classification is needed for pelvic pain
syndromes--are existing terminologies of spurious diagnostic authority bad for patients? J Urol. 2006
Jun;175(6):1989-90.
http://www.ncbi.nlm.nih.gov/pubmed/16697782
8. Baranowski AP, Abrams P, Berger RE, et al. Urogenital pain--time to accept a new approach to
phenotyping and, as a consequence, management. Eur Urol. 2008 Jan;53(1):33-6.
http://www.ncbi.nlm.nih.gov/pubmed/17961909
9. Baranowski AP, Abrams P, et al. (2008). Urogenital Pain in Clinical Practice. New York, Informa
Healthcare.
10. Hanno P, Lin A, Nordling J, et al. Bladder Pain Syndrome Committee of the International Consultation
on Incontinence. Neurourol Urodyn 29(1):191-198.
http://www.ncbi.nlm.nih.gov/pubmed/20025029
11. van de Merwe JP, Nordling J, Bouchelouche P, et al. Diagnostic criteria, classification, and
nomenclature for painful bladder syndrome/interstitial cystitis: an ESSIC proposal. Eur Urol. 2008
Jan;53(1):60-7.
http://www.ncbi.nlm.nih.gov/pubmed/17900797
Urology
Psychology
Organ specific
Infection
Tender muscle
Phenotyping
Urinary flow, micturition diary, cystoscopy, ultrasound, uroflowmetry
Neurological
Assessment
History of negative experiences, important loss, coping mechanism, depression
Ask for gynaecological, gastro-intestinal, ano-rectal, sexological complaints
Gynaecological examination, rectal examination
Semen culture and urine culture, vaginal swab, stool culture
Ask for neurological complaints (sensory loss, dysaesthesia).
Neurological testing during physical examination: sensory problems, sacral reflexes and muscular function
Palpation of the pelvic floor muscles, the abdominal muscles and the gluteal muscles

UPDATE FEBRUARY 2012 27
12. Wesselmann U, Baranowski AP, Börjesson M, et al. EMERGING THERAPIES AND NOVEL
APPROACHES TO VISCERAL PAIN. Drug Discov Today Ther Strateg. 2009 Fall;6(3):89-95
http://www.ncbi.nlm.nih.gov/pubmed/21243067
13. Giamberardino MA, Costantini R, Affaitati G, et al. Viscero-visceral hyperalgesia: characterization in
different clinical models. Pain. Pain. 2010 Nov;151(2):307-22.
http://www.ncbi.nlm.nih.gov/pubmed/20638177
14. Pezet S, McMahon SB. Neurotrophins: mediators and modulators of pain. Annu Rev Neurosci.
2006;29:507-38.
http://www.ncbi.nlm.nih.gov/pubmed/16776595
15. Cervero F, Laird JM. Understanding the signaling and transmission of visceral nociceptive events. J
Neurobiol. 2004 Oct;61(1):45-54.
http://www.ncbi.nlm.nih.gov/pubmed/15362152
16. Petersen M, Segon von Banchet G, Heppelman B, et al. Nerve growth factor regulates the expression
of bradykinin binding sites on adult sensory neurons via the neurotrophin receptor p75.Neuroscience.
1998 Mar;83(1):161-8.
http://www.ncbi.nlm.nih.gov/pubmed/9466406
17. McMahon SB, Jones NG. Plasticity of pain signaling: role of neurotrophic factors exemplified by acid-
induced pain. J Neurobiol. 2004 Oct;61(1):72-87.
http://www.ncbi.nlm.nih.gov/pubmed/15362154
18. Nazif O, Teichman JM, Gebhart GF, et al. Neural upregulation in interstitial cystitis. Urology. 2007
Apr;69(4 Suppl):24-33.
http://www.ncbi.nlm.nih.gov/pubmed/17462476
19. Merskey H, Bogduk N. Classification of Chronic Pain. Seattle, IASP press.
20. Melzack R, Coderre TJ, Katz J, et al. Central neuroplasticity and pathological pain. Ann N Y Acad Sci.
2001 Mar;933:157-74.
http://www.ncbi.nlm.nih.gov/pubmed/12000018
21. Fulbright RK, Troche CJ, Skudlarski P, et al. Functional MR imaging of regional brain activation
associated with the affective experience of pain. AJR Am J Roentgenol. 2001 Nov;177(5):1205-10.
http://www.ncbi.nlm.nih.gov/pubmed/11641204
22. Rygh LJ, Tjølsen A, Hole K, et al. Cellular memory in spinal nociceptive circuitry. Scand J Psychol.
2002 Apr;43(2):153-9.
http://www.ncbi.nlm.nih.gov/pubmed/12004953
23. Savidge CJ, Slade P. Psychological aspects of chronic pelvic pain. J Psychosom Res. 1997
May;42(5):433-44.
http://www.ncbi.nlm.nih.gov/pubmed/9194016
24. Raphael KG, Widom CS, Lange G. Childhood victimization and pain in adulthood: a prospective
investigation. Pain. 2001 May;92(1-2):283-93.
http://www.ncbi.nlm.nih.gov/pubmed/11323150
25. Raphael KG. Childhood abuse and pain in adulthood: more than a modest relationship? Clin J Pain.
2005 Sep-Oct;21(5):371-3.
http://www.ncbi.nlm.nih.gov/pubmed/16093741
26. Anda RF, Felitti VJ, Bremner JD, et al. The enduring effects of abuse and related adverse experiences
in childhood. A convergence of evidence from neurobiology and epidemiology. Eur Arch Psychiatry
Clin Neurosci. 2006 Apr;256(3):174-86.
http://www.ncbi.nlm.nih.gov/pubmed/16311898
27. Vecchiet L, Vecchiet J, Giamberardino MA. Referred Muscle Pain: Clinical and Pathophysiologic
Aspects. Curr Rev Pain. 1999;3(6):489-498.
http://www.ncbi.nlm.nih.gov/pubmed/10998708
28. Slocumb JC. Neurological factors in chronic pelvic pain: trigger points and the abdominal pelvic pain
syndrome. Am J Obstet Gynecol. 1984 Jul 1;149(5):536-43.
http://www.ncbi.nlm.nih.gov/pubmed/6234807
29. Taylor DC, Meyers WC, Moylan JA, et al. Abdominal musculature abnormalities as a cause of groin
pain in athletes. Inguinal hernias and pubalgia. Am J Sports Med. 1991 May-Jun;19(3):239-42.
http://www.ncbi.nlm.nih.gov/pubmed/1831010
30. Akermark C, Johansson C. Tenotomy of the adductor longus tendon in the treatment of chronic groin
pain in athletes. Am J Sports Med. 1992 Nov-Dec;20(6):640-3.
http://www.ncbi.nlm.nih.gov/pubmed/1456357
31. Fall M, Baranowski AP, Fowler CJ, et al. EAU guidelines on chronic pelvic pain. Eur Urol. 2004
Dec;46(6):681-9.
http://www.ncbi.nlm.nih.gov/pubmed/15548433

28 UPDATE FEBRUARY 2012
32. Shoskes DA, Nickel JC, Dolinga R, et al. Clinical phenotyping of patients with chronic prostatitis/
chronic pelvic pain syndrome and correlation with symptom severity.Urology. 2009 Mar;73(3):538-42;
discussion 542-3.
http://www.ncbi.nlm.nih.gov/pubmed/19118880
33. Magri V, Wagenlehner F, Perletti G, et al. Use of the UPOINT chronic prostatitis/chronic pelvic pain
syndrome classification in European patient cohorts: sexual function domain improves correlations.J
Urol. 2010 Dec;184(6):2339-45.
http://www.ncbi.nlm.nih.gov/pubmed/20952019
34. Krieger JN, Nyberg L Jr., Nickel JC. NIH consensus definition and classification of prostatitis. JAMA.
1999 Jul 21;282(3):236-7.
http://www.ncbi.nlm.nih.gov/pubmed/10422990
35. Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006
Apr;130(5):1480-91.
http://www.ncbi.nlm.nih.gov/pubmed/16678561
3. UROLOGICAL ASPECTS OF CHRONIC PELVIC
PAIN
3.1 Prostate pain syndrome
3.1.1 Introduction
Chronic pain in the region of the prostate has been linked to the term “prostatitis” in the past, although
there is a proven bacterial infection in only 10% of the cases (1). The remaining 90% should be classified as
prostate pain syndrome (PPS), based on the fact that there is no proven infection or other obvious pathology.
If CPP cannot be clearly ascribed to the prostate or another organ of the pelvis, the condition is defined more
generally as CPPS, as outlined in Chapter 2.
3.1.2 Definition
Prostate pain syndrome is the occurrence of persistent or recurrent episodic pain in the region of the prostate
over at least 3 out of the past 6 months, which is convincingly reproduced by prostate palpation. There is no
proven infection or other obvious local pathology. PPS is often associated with negative cognitive, behavioural,
sexual, or emotional consequences (2), as well as with symptoms suggestive of lower urinary tract and sexual
dysfunction (3,4). According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
classification, this correlates to CP/CPPS (Cat. III). Laboratory diagnosis goes along with sterile specimen
cultures and either significant, or insignificant, white blood cell counts in prostate-specific specimens (i.e.
semen, expressed prostatic secretions and urine collected after prostate massage) (5). At present, there are no
clinically relevant diagnostic or therapeutic consequences arising from differentiating inflammatory from non-
inflammatory PPS (according to NIH definition), therefore, they are considered here as one entity.
3.1.3 Pathogenesis
Pain is the main symptom in PPS. As a common feature of chronic pain syndromes, no single aetiological
explanation has been found. One explanation (6) is that the condition probably occurs in susceptible men
exposed to one or more initiating factors, which may be single, repetitive or continuous. Several of these
potential initiating factors have been proposed, including infectious, genetic, anatomical, neuromuscular,
endocrine, immune (including autoimmune), or psychological mechanisms. These factors may then lead to a
peripheral self-perpetuating immunological inflammatory state and/or neurogenic injury, creating acute and
then chronic pain. Based on the peripheral and the CNS, sensitisation involving neuroplasticity may lead to a
centralised neuropathic pain state (see Chapter 2) (6). This could also explain why tissue damage is not usually
found in PPS. There is growing evidence for a neuropathic origin and association with CNS changes of pain
in PPS. As outlined earlier, PPS patients have been shown to report higher visual analogue scale scores than
controls to short bursts of noxious stimuli to the perineum but not to the anterior thigh (7). This implies an
altered sensation in the perineum compared with healthy controls similar to other chronic pain syndromes.
3.1.4 Epidemiology
There is only limited information on the true prevalence of PPS in the population. As a result of significant
overlap of symptoms with other conditions (e.g. benign prostate syndrome and BPS), purely symptom-based
case definitions may not reflect the true prevalence of PPS (8,9). Prostatitis was diagnosed in 8% of all visits

UPDATE FEBRUARY 2012 29
to urologists and 1% of all primary care physicians annually in the USA (10). In a systematic review of the
literature, the population-based prevalence of prostatitis symptoms was found to be 8.2% (range: 2.2-9.7%)
(11). In two recent studies not included in this review, prevalence was found to be 2.7% (4) and 2% (12). A
prospective Italian survey of visits to a urologist for a physician-assigned diagnosis of prostatitis revealed a
prevalence of 12.8%. Among these, ~40% had clinical features of PPS (13). In a self-reported, population-
based, cross sectional study of Finnish men aged 20-59 years, the overall lifetime prevalence of prostatitis was
as high as 14.2% (14). The risk of prostatitis increased with age (men aged 50-59 years had a 3.1-fold greater
risk than those aged 20-39 years). Usual clinical treatment in North American populations has been studied in
two studies of sufficient quality. In the follow-up of a cohort of men with PPS-like symptoms based on the NIH
Prostatitis Symptom Index (NIH-CPSI) pain and voiding domains, 63% still suffered from persistent symptoms,
in contrast to 3% of controls with newly developing symptoms (15). Patients with more severe symptoms were
more likely to report symptoms 1 year later. In addition, symptoms substantially improved for up to 6 months
follow-up, but then remained unchanged (16).
3.1.5 Diagnosis
Prostate pain syndrome is a symptomatic diagnosis, which is diagnosed from a history of pain perceived in the
region of the prostate (convincingly reproduced by prostate palpation), and absence of other lower urinary tract
pathology, for a minimum of 3 out of the past 6 months. This implies that specific disease-associated pelvic
pain caused by bacterial infection, urogenital cancer, urinary tract disease, urethral stricture, and neurogenic
disease of the bladder must be ruled out. A thorough history is an important first step in the evaluation of
PPS. It should include type of pain and localisation. Pain is often reported in other pelvic areas outside the
prostate such as perineum, rectum, penis, testicles and abdomen (17). In addition, associated lower urinary
tract symptoms (LUTS), sexual function, psychological, social and economic factors should be addressed.
Determination of the severity of disease, its progression and treatment response can be assessed only by
means of a validated symptom-scoring instrument. QoL should also be measured because it can be as poor as
in acute myocardial infarction, unstable angina pectoris or Crohn’s disease (19,20). In a study by Tripp et al. (2)
more pain, pain-contingent rest, and urinary symptoms were associated with greater disability (also measured
by self-report), and pain was predicted by depression and by catastrophising (helplessness subscale).
Demographic and social support variables were not associated with either pain or adjustment.
Reliable, valid indexes of symptoms and QoL are the NIH-CPSI (17) and the International Prostate Symptom
Score (I-PSS) (18). These subjective outcome measures are recommended for the basic evaluation and
therapeutic monitoring of patients in urological practice and have been translated and validated for many
European languages.
There is no single “gold standard” diagnostic test for PPS, therefore, procedures are on the one hand directed
towards identification and exclusion of specific diseases associated with pelvic pain, and on the other hand
may be used for phenotypic description. Physical examination including digital rectal examination should be
carried out. Muscle tenderness and trigger points in the pelvic floor may be palpated. Measurement of resting
urine by ultrasound should exclude incomplete voiding. Prostate-specific antigen testing does not help to
diagnose PPS but can exclude prostate cancer in patients at risk.
Laboratory diagnosis has been classically based on the four-glass test for bacterial localisation (21).
Besides sterile pre-massage urine (voided bladder urine-2), PPS shows < 10,000 cfu of uropathogenic bacteria
in expressed prostatic secretions and insignificant numbers of leukocytes or bacterial growth in ejaculates.
However, this test is too complex for use by practising urologists. Diagnostic efficiency may be enhanced cost-
effectively by a simple screening procedure, that is, the two-glass test or pre-post-massage test (PPMT) (22). In
an extensive analysis of both tests, PPMT was able to indicate the correct diagnosis in > 96% of patients (23).
Overall, these tests help only a little in the diagnosis of PPS, because 8% of patients with suggested PPS have
been found to have positive prostatic localisation cultures, similar to the percentage of asymptomatic (24).
In PPS, urodynamic studies should be considered in patients with significant LUTS. They may
demonstrate decreased urinary flow rates, incomplete relaxation of the bladder neck and prostatic urethra, as
well as abnormally high urethral closure pressure at rest. The external urethral sphincter may be dysfunctional
(non-relaxing) during voiding (25). As for non-PPS cases, cystoscopy may be considered for further evaluation
of micturition symptoms to exclude bladder outlet or urethral pathology, or if haematuria or infection has been
found to exclude intravesical pathology.
A general algorithm for assessment and treatment of PPS is shown in Figure 5.

30 UPDATE FEBRUARY 2012
3.1.6 Conclusions and recommendations: assessment/diagnosis PPS
Conclusions LE
PPS is associated with negative cognitive, behavioural, sexual, or emotional consequences, as well
as with symptoms suggestive of lower urinary tract and sexual dysfunction.
2b
PPS has no known single aetiology. 3
Pain in PPS involves mechanisms of neuroplasticity and neuropathic pain. 2a
PPS has a high impact on QoL. 2b
Depression and catastrophic thinking are associated with more pain and poorer adjustment. 3
The prevalence of PPS-like symptoms is high in population-based studies (> 2%). 2b
There is significant overlap of symptoms with other conditions. 2b
Reliable instruments assessing symptom severity as well as phenotypic differences exist. 2b
Recommendations GR
Specific diseases with similar symptoms must be excluded. It is therefore recommended to adapt
diagnostic procedures to the patient and to aim at identifying them.
A
After primary exclusion of specific diseases, patients with symptoms according to the above
definition should be diagnosed with prostate pain syndrome.
A
A validated symptom and quality of life scoring instrument, such as the NIH-CPSI, should be
considered for initial assessment as well as for follow-up.
B
It is recommended to assess prostate pain syndrome associated negative cognitive, behavioural,
sexual, or emotional consequences, as well as symptoms of lower urinary tract and sexual
dysfunctions.
B
3.1.7 Treatment
There is a large discrepancy in the treatment effects reported in case series and controlled trials that results
from a large placebo effect or publication bias. As a result of the multifactorial origin of PPS, one reason for
treatment failure in some large randomised placebo-controlled trials may be the heterogeneity of the patient
population. Thus, one strategy for improving treatment effects may be stratification of patient phenotypes.
A prospective series of phenotypically directed treatment for PPS has shown significant improvement of
symptoms and QoL (26). Monotherapeutic strategies for the treatment of PPS may fail (27), therefore, most
patients require multimodal treatment aimed at the main symptoms, and taking comorbidity into account. In the
past 10 years, results from RCTs have led to advances in standard and novel treatment options.
3.1.7.1 Alpha-blockers
Positive results from RCTs of alpha-blockers, i.e. terazosin (28,29), alfuzosin (30) doxazosin (31,32) and
tamsulosin (33) have led to widespread use of alpha-antagonists in the treatment of PPS in recent years. The
effects of alpha-antagonists may include improved outflow performance by blocking the alpha-receptors of
the bladder neck and prostate and by direct action on alpha1A/1D receptors in the CNS (33). In contrast,
an earlier meta-analysis of nine trials (n = 734) did not show a beneficial effect on pain (34). Moreover, in
accordance with an earlier negative report on tamsulosin (35), one adequately powered large placebo-
controlled randomised trial of 12 weeks treatment with alfuzosin failed to show any significant difference in the
outcome measures, with the exception of the score for ejaculation of the Male Sexual Health Questionnaire
scores (showing significant improvement in the alfuzosin group compared to the placebo group, P= 0.04) (36).
Regarding safety, this large trial reported similar adverse event rates in the treatment and placebo groups.
The most recent in-depth systematic review and network meta-analysis of alpha-blockers (37) has shown
significant improvement in symptoms, with standardised mean differences in total symptom, pain, voiding, and
QoL scores of -1.7 [95% confidence interval (CI): -1.8 to -0.3], -1.1 (95% CI: -1.8 to -0.3), 1.4 (95% CI: -2.3 to
-0.5), and -1.0 (95% CI: -1.8 to 0.2), respectively. In addition, they had a higher rate of favourable response
compared to placebo (pooled relative risk of 1.6 (95% CI: 1.1-2.3). However, this finding was associated with
publication bias for smaller studies. Overall, alpha-blockers seem to have moderate but significant beneficial
effects. This probably is not the case for long-standing PPS patients (36). Future studies should show if
longer duration of therapy or some sort of phenotypically directed (e.g. patients with PPS and relevant voiding
dysfunction) treatment strategies will improve treatment outcomes.

UPDATE FEBRUARY 2012 31
3.1.7.2 Antibiotic therapy
Empirical antibiotic therapy is widely used because some patients have improved with antimicrobial therapy.
Patients responding to antibiotics should be maintained on medication for 4-6 weeks or even longer.
Unfortunately, culture, leukocyte and antibody status of prostate-specific specimens does not predict antibiotic
response in patients with PPS (38), and prostate biopsy culture findings do not differ from those of healthy
controls (39). The only randomised placebo-controlled trials of sufficient quality have been done for oral
antibiotic treatment with ciprofloxacin (6 weeks) (35), levofloxacin (6 weeks) (40), and tetracycline hydrochloride
(12 weeks) (41). These have been analysed in a recently published meta-analysis (37). Although direct meta-
analysis has not shown significant differences in outcome measures, network meta-analysis has suggested
significant effects in decreasing total symptom scores (-9.8; 95% CI: -15.1 to -4.6), pain scores (-4.4; 95% CI:
-7.0 to -1.9), voiding scores (-2.8; 95% CI: -4.1 to -1.6), and QoL scores (-1.9; 95% CI: -3.6 to -0.2) compared
with placebo. Overall, antibiotic treatment of PPS is based only on weak evidence. Combination therapy of
antibiotics with alpha-blockers has shown even better outcomes in network meta-analysis. However, sample
sizes of the studies were relatively small and treatment effects were only modest and most of the time below
clinical significance. It may be speculated that patients profiting from treatment have had some unrecognised
uropathogens. If antibiotics are used, other therapeutic options should be offered after one unsuccessful
course of a quinolone or tetracycline antibiotic over 6 weeks.
3.1.7.3 Anti-inflammatory drugs
For non-steroidal anti-inflammatory drugs, only two RCTs have been published. The first was for rofecoxib,
which is no longer on the market; statistical significance over placebo was achieved in some of the outcome
measures (42). In the second trial with celecoxib, pain subscore, QoL subscore, and total NIH-CPSI score
were in favour of the treatment arm versus placebo, but effects were limited to the duration of therapy (43).
A leukotriene antagonist, zafirlukast, has been evaluated in a small randomised placebo-controlled study
of patients treated with concomitant doxycycline (44). This study was negative but had a lack of power. For
corticosteroids, no significant benefits were shown in a low-power, placebo-controlled, randomised pilot
study of a short course of oral prednisolone (45). In a recent meta-analysis, two studies of NSAIDs (40,43) and
one with prednisolone (45) were pooled. Anti-inflammatory drugs were 80% more likely to have a favourable
response than placebo (total n = 190, RR: 1.8; 95% CI: 1.2-2.6). Overall, a moderate treatment effect has been
shown for anti-inflammatory drugs, but larger studies should be done for final confirmation, and long-term side
effects have to be taken into account.
3.1.7.4 Opioids
Opioids produce modest pain relief in some patients with refractory PPS, although there are limited data on
the long-term efficacy of opioids in non-cancer pain. Opioid treatment carries the risks of side effects, reduced
QoL, addiction, opioid tolerance and opioid-induced hyperalgesia (46). Urologists should use opioids for PPS
only in collaboration with pain clinics and with other treatments.
3.1.7.5 5-alpha-reductase inhibitors
Although a few small pilot studies with 5-alpha-reductase inhibitors supported the view that finasteride may
improve voiding and pain, the first placebo-controlled randomised trial published in a peer-reviewed journal did
not support this, but the study did lack power (47). In another RCT, finasteride provided better amelioration of
symptoms compared to saw palmetto over a 1-year period, but lacked a placebo-control arm (48). A 6-month
placebo-controlled study showed a non-significant tendency towards better outcome in favour of finasteride,
possibly because of a lack of statistical power (49). Based on these data, 5-alpha-reductase inhibitors cannot
be recommended for use in PPS.
3.1.7.6 Allopurinol
An RCT of allopurinol was conducted based on the hypothesis that urine reflux intoprostatic ducts causes
prostatic inflammation via high concentrations of purine and pyrimidine base-containing metabolites in
prostatic secretions (50). However, positive results have not been considered sufficient for recommendation
by reviewers of the Cochrane Database (51). In addition, a recent randomised placebo-controlled trial of
allopurinol as an adjunct to ofloxacin has not shown any benefit (52).
3.1.7.7 Phytotherapy
Positive effects of phytotherapy have been documented. Although a validated symptom score was not used,
an RCT of a pollen extract (Prostat/Poltit) showed significant symptom improvement (53). An adequately
powered randomised placebo-controlled study of Cernilton, another pollen extract, showed clinically significant
symptom improvement over a 12-week period in inflammatory PPS patients (NIH Cat. IIIA) (54). The effect
was mainly based on a significant effect on pain. Quercetin, a polyphenolic bioflavonoid with documented

32 UPDATE FEBRUARY 2012
antioxidant and anti-inflammatory properties, improved NIH-CPSI scores significantly in a small RCT (55).
In contrast, treatment with saw palmetto, most commonly used for benign prostatic hyperplasia, did not
improve symptoms over a 1-year period (47). In a systematic review and meta-analysis, patients treated
with phytotherapy were found to have significantly lower pain scores than those treated with placebo (37). In
addition, overall response rate in network analysis was in favour of phytotherapy (RR: 1.6; 95% CI: 1.1-1.6).
3.1.7.8 Pentosan polysulphate
High-dose oral pentosan polysulphate (3 300 mg/day), as for BPS, is able to improve clinical global assessment
and QoL significantly over placebo in men with PPS, suggesting a possible common aetiology (56).
3.1.7.9 Muscle relaxants
Muscle relaxants (diazepam, baclofen) are claimed to be helpful in sphincter dysfunction or pelvic floor/perineal
muscle spasm, but there have been only a few prospective clinical trials to support these claims. In a recent
RCT, a triple combination of a muscle relaxant (tiocolchicoside), an anti-inflammatory drug (ibuprofen) and an
alpha-blocker (doxazosin) was effective in treatment-naïve patients, but not superior to an alpha-blocker alone
(32).
3.1.7.10 Pregabalin
Pregabalin is an antiepileptic drug that has been approved for use in chronic postherpetic neuralgia,
fibromyalgia, and diabetic neuropathy. In an adequately powered randomised placebo-controlled study, a
6-week course of pregabalin (n = 218) compared to placebo (n = 106) did not result in a significant reduction of
NIH-CPSI total score by at least 6 points (57).
3.1.7.11 Botulinum toxin A
Botulinum toxin A (BTX-A) may have pain-alleviating effects through non-neuromuscular action on afferent
nociceptive pathways. Local treatment with periurethral injection of BTX-A (200 U) has been tested in a small
pilot study with improvement in pain and changes in urethral pressure profile (58). A small randomised placebo-
controlled study of perineal skeletal muscle injection (100 U) has been published recently (59). Some effect
was found in the global response assessment and the NIH-CPSI pain subdomain score. However, patient
number was too low (13 in the BTX-A group and 16 in the placebo group), and follow-up was too short to draw
definitive conclusions.
3.1.7.12 Physical treatments
• Electromagnetic therapy. In a small, sham-controlled, double-blind study, 4 weeks electromagnetic
therapy showed a significant, sustained effect over a 1-year period (60).
• Microwave thermotherapy. Significant symptomatic improvement has been reported from heat
therapy, for example, transrectal and transurethral thermotherapy (61,62), but there was no sham-
control.
• Extracorporeal shock wave therapy. A recent sham-controlled double-blind study of four times weekly
perineal extracorporeal shock wave therapy (n = 30) showed significant improvement in pain, QoL,
and voiding compared to the control group (n = 30) over 12 weeks (63). Confirmatory studies are
awaited because of an absent placebo-effect, which is very unusual in PPS trials.
• Electroacupuncture. In a small three-arm randomised trial, electroacupuncture was superior to sham
treatment and advice and exercise alone (64). In a recent prospective case series of 6 weeks of weekly
electroacupuncture of 97 patients with PPS, 92% showed significant improvement in total NIH-CPSI
score. Based on these studies, no definitive conclusion can be drawn.
• Posterior tibial nerve stimulation. One sham-controlled medium-sized study (n = 89) demonstrated
significant improvement in total NIH-CPSI score and visual analogue scale for pain (65).
• Myofascial physical therapy. A randomised feasibility trial of myofascial physical therapy including PPS
(n = 21) and patients with BPS showed a clinical benefit compared to global therapeutic massage (66).
In the PPS group alone, there was no difference in the effect between the two treatment arms.
3.1.7.13 Surgical management
Surgical management, including transurethral incision of the bladder neck, radical transurethral resection of
the prostate, or in particular, radical prostatectomy, has a very limited role and requires an additional, specific
indication. In addition, the treatment effect of transurethral needle ablation of the prostate (TUNA) was only
comparable to sham treatment in two small randomised trials (67,68).
3.1.7.14 Psychological treatment
It is of note that QoL decreases as symptoms increase. Given prediction of QoL by psychological problems

UPDATE FEBRUARY 2012 33
(depression and catastrophising in particular), this means that psychological status should also be targeted
in treatment, and the development of a psychologically focused treatment for patients refractory to
drug treatment has been noted by the authors of the summary findings from the NIH Chronic Prostatitis
Collaborative Research Network studies (69). There are no RCTs of psychological treatment for men with CPP,
but Tripp et al. (70) have completed a feasibility trial, which represents the only known account of psychological
treatment. Their 8-h intervention improved pain, catastrophising, and QoL, but not depression or some urinary
symptoms. Details concerning appropriate treatment content and delivery are contained in Chapter 8.
3.1.8 Conclusions and recommendations: treatment of PPS
Conclusions LE
Monotherapeutic treatment regimens in PPS may fail. 3
Phenotypically directed treatment may improve treatment success. 3
Alpha-blockers have moderate treatment effect regarding total pain-, voiding-, and QoL scores in
PPS.
1a
Antimicrobial therapy has a moderate effect on total pain-, voiding-, and QoL scores in PPS. 1a
NSAIDs have moderate overall treatment effects on PPS. 1a
There are insufficient data on the effectiveness of steroids in PPS. 2b
There are insufficient data on the effectiveness of opioids in PPS. 4
There are insufficient data on the effectiveness of 5-alpha-reductase inhibitors in PPS. 2b
There are insufficient data on the effectiveness of allopurinol in PPS. 2b
Phytotherapy has some beneficial effect on pain and overall favourable treatment response in PPS. 1a
Pentosan polysulphate improves global assessment and QoL score in PPS. 1b
There are insufficient data on the effectiveness of muscle relaxants in PPS. 2b
Pregabalin is not effective for the treatment of PPS. 1b
BTX-A injection into the pelvic floor may have a modest effect in PPS. 2b
There are only limited data on the effectiveness of electromagnetic therapy in PPS. 2b
There are only limited data on the effectiveness of microwave thermotherapy in PPS. 3
Perineal extracorporeal shock wave therapy probably is effective for the treatment of PPS. 1b
There are limited data on the effectiveness of electroacupuncture for the treatment of PPS. 2b
Posterior tibial nerve stimulation is probably effective for the treatment of PPS. 1b
There are insufficient data on the effectiveness of myofascial physical therapy for the treatment of
PPS.
2b
There are limited data on lack of effectiveness of TUNA of the prostate for PPS. 2b
There are insufficient data supporting the use of other surgical treatments, such as transurethral
incision of the bladder neck, transurethral resection of the prostate, or radical prostatectomy in
patients with PPS.
3
Cognitive behavioural therapy designed for PPS may improve pain, and QoL. 3

34 UPDATE FEBRUARY 2012
Recommendations GR
Consider multimodal and phenotypically directed treatment options for PPS. B
Alpha-blockers are recommended for patients with a duration of PPS < 1 year. A
Single use of antimicrobial therapy (quinolones or tetracyclines) is recommended in treatment-naïve
patients over a minimum of 6 weeks with a duration of PPS < 1 year.
A
NSAIDs are recommended for use in PPS, but long-term side effects have to be considered. B
Allopurinol is not recommended for use in PPS. B
Phytotherapy might be used in patients with PPS. B
Consider high-dose pentosan polysulphate to improve symptoms and quality of life in PPS. A
Pregabalin is not recommended for use in PPS. A
Perineal extracorporeal shock wave therapy might be considered for the treatment of PPS. B
Electroacupuncture might be considered for the treatment of PPS. B
Posterior tibial nerve stimulation might be considered for the treatment of PPS. B
TUNA of the prostate is not recommended for the treatment of PPS. B
For PPS with significant psychological distress, psychological treatment focussed on PPS should be
attempted.
B
PPS = prostate pain syndrome; TUNA = transurethral needle ablation.
Figure 5: assessment and treatment algorithm for PPS
3.1.9 References
1. de la Rosette JJ, Hubregtse MR, Meuleman EJ, et al. Diagnosis and treatment of 409 patients with
prostatitis syndromes. Urology 1993 Apr;41(4):301-7.
http://www.ncbi.nlm.nih.gov/pubmed/8470312
2. Tripp DA, Nickel JC, Wang Y, et al. Catastrophizing and pain-contingent rest predict patient
adjustment in men with chronic prostatitis/chronic pelvic pain syndrome.J Pain. 2006 Oct;7(10):697-
708.
http://www.ncbi.nlm.nih.gov/pubmed/17018330
3. Walz J, Perotte P, Hutterer G, et al. Impact of chronic prostatitis-like symptoms on the quality of life in
a large group of men. BJU Int. 2007 Dec;100(6):1307-11.
http://www.ncbi.nlm.nih.gov/pubmed/17941922
4. Marszalek M, Wehrberger C, Hochreiter W, et al. Symptoms suggestive of chronic pelvic pain
syndrome in an urban population: prevalence and associations with lower urinary tract symptoms and
erectile function. J Urol. 2007 May;177(5):1815-9.
http://www.ncbi.nlm.nih.gov/pubmed/17437827
Urine culture
Uroflowmetry
Transrectal US
prostate
NIH-CPSI scoring
list
Pelvic floor muscle
testing
Assessment
Grade A recommended
Phenotyping
Treatment
Grade B recommended
Not recommended
Alpha-blockers when duration is < 1 year
Single use antibiotics (6 weeks) when duration is < 1 year
NSAID’s. Be aware of long-term side effects
Phytotherapy
High dose Pentosan polysulfate to improve QoL and symptoms
Allopurinol [B]
Pregabalin [A]
Perineal extracorporeal shockwave therapy
Electroacupuncture
Percutaneous tibial nerve stimulation (PTNS)
TransUrethral Needle Ablation (TUNA) [B]
Psychological treatment focused on the pain

UPDATE FEBRUARY 2012 35
5. Nickel JC. Prostatitis: myths and realities. Urology. 1998 Mar;51(3):362-6.
http://www.ncbi.nlm.nih.gov/pubmed/9510337
6. Nickel JC, Baranowski AP, Pontari M, et al. Management of men diagnosed with chronic prostatitis/
chronic pelvic pain syndrome who have failed traditional management. Rev Urol. 2007;9(2) :63-72
http://www.ncbi.nlm.nih.gov/pubmed/17592539
7. Yang CC, Lee JC, Kromm BG, et al. Pain sensitization in male chronic pelvic pain syndrome: why are
symptoms so difficult to treat? J Urol. 2003 Sep;170(3):823-6.
http://www.ncbi.nlm.nih.gov/pubmed/12913708
8. Barry MJ, Link CL, McNaughton-Collins MF, et al. Overlap of different urological symptom complexes
in a racially and ethnically diverse, community-based population of men and women.BJU Int. 2008
Jan;101(1):45-51.
http://www.ncbi.nlm.nih.gov/pubmed/17868419
9. Roberts RO, Jacobson DJ, Girman CJ, et al. Low agreement between previous physician diagnosed
prostatitis and national institutes of health chronic prostatitis symptom index pain measures.J Urol.
2004 Jan;171(1):279-83.
http://www.ncbi.nlm.nih.gov/pubmed/14665894
10. Collins MM, Stafford RS, O’Leary MP, et al. How common is prostatitis? A national survey of physician
visits.J Urol. 1998 Apr;159(4):1224-8.
http://www.ncbi.nlm.nih.gov/pubmed/9507840
11. Krieger JN, Lee SW, Jeon J, et al. Epidemiology of prostatitis. Int J Antimicrob Agents. 2008 Feb;31
Suppl 1:S85-90.
http://www.ncbi.nlm.nih.gov/pubmed/18164907
12. Ferris JA, Pitts MK, Richters J, et al. National prevalence of urogenital pain and prostatitis-like
symptoms in Australian men using the National Institutes of Health Chronic Prostatitis Symptoms
Index.BJU Int. 2010 Feb;105(3):373-9.
http://www.ncbi.nlm.nih.gov/pubmed/19549116
13. Rizzo M, Marchetti F, Travaglini A, et al. Prevalence, diagnosis and treatment of prostatitis in Italy: A
prospective urology outpatient practice study. BJU Int. 2003 Dec;92(9):955-9.
http://www.ncbi.nlm.nih.gov/pubmed/14632854
14. Mehik A, Hellström P, Lukkarinen O, et al. Epidemiology of prostatitis in Finnish men: a population-
based cross-sectional study.BJU Int. 2000 Sep;86(4):443-8.
http://www.ncbi.nlm.nih.gov/pubmed/10971269
15. Nickel JC, Siemens DR, Nickel KR, et al. The patient with chronic epididymitis: Characterization of an
enigmatic syndrome. J Urol. 2002 Apr;167(4):1701-4.
http://www.ncbi.nlm.nih.gov/pubmed/11912391
16. Turner JUA, Ciol MA, Von Korff M, et al. Prognosis of patients with new prostatitis/pelvic pain
syndrome episodes.J Urol. 2004 Aug;172(2):538-41.
http://www.ncbi.nlm.nih.gov/pubmed/15247724
17. Litwin MS, McNaughton-Collins M, Fowler FJ Jr, et al. The National Institutes of Health chronic
prostatitis symptom index: development and validation of a new outcome measure. Chronic Prostatitis
Collaborative Research Network. J Urol 1999 Aug;162(2):369-75.
http://www.ncbi.nlm.nih.gov/pubmed/10411041
18. Mebust WK, Bosch R, Donovan J, et al. Symptom evaluation, quality of life and sexuality. In: Cockett
ATK, Khoury S, Aso Y, et al. Proceedings of the 2ndConsultation on Benign Prostatic Hyperplasia
(BPH), Paris. Channel Islands: Scientific Communication International Ltd, 1993, pp. 131-138.
19. Wenninger K, Heiman JR, Rothman I, et al. Sickness impact of chronic nonbacterial prostatitis and its
correlates. J Urol 1996 Mar;155(3):965-8.
http://www.ncbi.nlm.nih.gov/pubmed/8583619
20. McNaughton Collins M, Pontari MA, O’Leary MP, et al; Chronic Prostatitis Collaborative Research
Network. Quality of life is impaired in men with chronic prostatitis: the Chronic Prostatitis Collaborative
Research Network. J Gen Intern Med 2001 Oct;16(10):656-62.
http://www.ncbi.nlm.nih.gov/pubmed/11679032
21. Meares EM, Stamey TA. Bacteriologic localization patterns in bacterial prostatitis and urethritis. Invest
Urol 1968 Mar;5(5):492-518.
http://www.ncbi.nlm.nih.gov/pubmed/4870505
22. Nickel JC. The Pre and Post Massage Test (PPMT): a simple screen for prostatitis. Tech Urol 1997
Spring;3(1):38-43.
http://www.ncbi.nlm.nih.gov/pubmed/9170224

36 UPDATE FEBRUARY 2012
23. Nickel JC, Shoskes D, Wang Y, et al. How does the pre-massage and postmassage 2-glass test
compare to the Meares-Stamey 4-glass test in men with chronic prostatitis/chronic pelvic pain
syndrome? J Urol 2006 Jul;176(1):119-24.
http://www.ncbi.nlm.nih.gov/pubmed/16753385
24. Nickel JC, Pontari M, Moon T, et al; Rofecoxib Prostatitis Investigator Team. A randomized, placebo
controlled, multicenter study to evaluate the safety and efficacy of rofecoxib in the treatment of
chronic nonbacterial prostatitis. J Urol 2003 Apr;169(4):1401-5.
http://www.ncbi.nlm.nih.gov/pubmed/12629372
25. Zermann DH, Ishigooka M, Doggweiler R, et al. Neurourological insights into the etiology of
genitourinary pain in men. J Urol. 1999 Mar;161(3):903-8.
http://www.ncbi.nlm.nih.gov/pubmed/10022711
26. Shoskes DA, Nickel JC, Kattan MW. Phenotypically Directed Multimodal Therapy for Chronic
Prostatitis/Chronic Pelvic Pain Syndrome: A Prospective Study Using UPOINT. Urology. 2010
Jun;75(6):1249-53.
http://www.ncbi.nlm.nih.gov/pubmed/20363491
27. Nickel JC, Narayan P, McKay J, et al. Treatment of chronic prostatitis/chronic pelvic pain syndrome
with tamsulosin: a randomized double blind trial. J Urol 2004 Apr;171(4):1594-7.
http://www.ncbi.nlm.nih.gov/pubmed/15017228
28. Cheah PY, Liong ML, Yuen KH, et al. Terazosin therapy for chronic prostatitis/chronic pelvic pain
syndrome: a randomized, placebo controlled trial. J Urol 2003 Feb;169(2):592-6.
http://www.ncbi.nlm.nih.gov/pubmed/12544314
29. Gül O, Eroglu M, Ozok U. Use of terazosine in patients with chronic pelvic pain syndrome and
evaluation by prostatitis symptom score index. Int Urol Nephrol. 2001;32(3):433-6.
http://www.ncbi.nlm.nih.gov/pubmed/11583367
30. Mehik A, Alas P, Nickel JC, et al. Alfuzosin treatment for chronic prostatitis/chronic pelvic pain
syndrome: a prospective, randomized, double-blind, placebo-controlled, pilot study. Urology 2003
Sep;62(3):425-9.
http://www.ncbi.nlm.nih.gov/pubmed/12946740
31. Evliyaoglu Y, Burgut R. Lower urinary tract symptoms, pain and quality of life assessment in chronic
non-bacterial prostatitis patients treated with alpha-blocking agent doxazosin; versus placebo. Int Urol
Nephrol 2002;34(3):351-6.
http://www.ncbi.nlm.nih.gov/pubmed/12899226
32. Tugcu V, Tasci AI, Fazlioglu, Gurbuz G, Ozbek E, Sahin S, Kurtulus F, Cek M. A placebo-controlled
comparison of the efficiency of triple- and monotherapy in category III B chronic pelvic pain syndrome
(PPS). Eur Urol 2007 Apr;51(4):1113-7; discussion 1118.
http://www.ncbi.nlm.nih.gov/pubmed/17084960
33. Nickel JC, Downey J, Pontari MA, et al. A randomized placebo-controlled multicentre study to
evaluate the safety and efficacy of finasteride for male chronic pelvic pain syndrome (category IIIA
chronic nonbacterial prostatitis). BJU Int 2004 May;93(7):991-5.
http://www.ncbi.nlm.nih.gov/pubmed/15142149
34. Yang G, Wei Q, Li H, et al. The effect of alpha-adrenergic antagonists in chronic prostatitis/
chronic pelvic pain syndrome: a meta-analysis of randomized controlled trials. J Androl 2006 Nov-
Dec;27(6):847-52.
http://www.ncbi.nlm.nih.gov/pubmed/16870951
35. Alexander RB, Propert KJ, Schaeffer AJ, et al. Ciprofloxacin or tamsulosin in men with chronic
prostatitis/chronic pelvic pain syndrome: a randomized, double-blind trial. Ann Intern Med. 2004 Oct
19;141(8):581-9.
http://www.ncbi.nlm.nih.gov/pubmed/15492337
36. Nickel JC, Krieger JN, McNaughton-Collins M, et al; Chronic Prostatitis Collaborative Research
Network. Alfuzosin and symptoms of chronic prostatitis-chronic pelvic pain syndrome. N Engl J Med
2008 Dec 18;359(25):2663-73.
http://www.ncbi.nlm.gov/pubmed/19092152
37. Anothaisintawee, AttiaJ, Nickel JC, et al. Management of chronic prostatitis/chronic pelvic pain
syndrome: A systematic review and network meta-analysis. JAMA. 2011 Jan 5;305(1):78-86.
http://www.ncbi.nlm.nih.gov/pubmed/21205969
38. Nickel JC, Downey J, Johnston B, et al; Canadian Prostatitis Research Group. Predictors of patient
response to antibiotic therapy for the chronic prostatitis/chronic pelvic pain syndrome: a prospective
multicenter clinical trial. J Urol 2001 May;165(5):1539-44.
http://www.ncbi.nlm.nih.gov/pubmed/11342913

UPDATE FEBRUARY 2012 37
39. Lee JC, Muller CH, Rothman I, et al. Prostate biopsy culture findings of men with chronic pelvic pain
syndrome do not differ from those of healthy controls. J Urol 2003 Feb;169(2):584-7.
http://www.ncbi.nlm.nih.gov/pubmed/12544312
40. Nickel JC, Pontari M, Moon T, et al; Rofecoxib Prostatitis Investigator Team. A randomized, placebo
controlled, multicenter study to evaluate the safety and efficacy of rofecoxib in the treatment of
chronic nonbacterial prostatitis. J Urol 2003 Apr;169(4):1401-5.
http://www.ncbi.nlm.nih.gov/pubmed/12629372
41. Zhou Z, Hong L, Shen X, et al. Detection of Nanobacteria Infection in Type III Prostatitis. Urology.
2008 Jun;71(6):1091-5.
http://www.ncbi.nlm.nih.gov/pubmed/18538692
42. Nickel JC, Downey J, Clark J, et al. Levofloxacin for chronic prostatitis/chronic pelvic pain syndrome
in men: A randomized placebo-controlled multicenter trial. Urology. 2003 Oct;62(4):614-7.
http://www.ncbi.nlm.nih.gov/pubmed/14550427
43. Zhao WP, Zhang ZG, Li XD, et al. Celecoxib reduces symptoms in men with difficult chronic pelvic
pain syndrome (Category IIIA). Braz J Med Biol Res. 2009 Oct;42(10):963-7.
http://www.ncbi.nlm.nih.gov/pubmed/19787151
44. Goldmeier D, Madden P, McKenna M, et al. Treatment of category III A prostatitis with zafirlukast: A
randomized controlled feasibility study. Int J STD AIDS. 2005 Mar;16(3):196-200.
http://www.ncbi.nlm.nih.gov/pubmed/15829018
45. Bates SM, Hill VA, Anderson JB, et al. A prospective, randomized, double-blind trial to evaluate the
role of a short reducing course of oral corticosteroid therapy in the treatment of chronic prostatitis/
chronic pelvic pain syndrome. BJU Int 2007 Feb;99(2):355-9.
http://www.ncbi.nlm.nih.gov/pubmed/17313424
46. Nickel JC. Opioids for chronic prostatitis and interstitial cystitis: lessons learned from the 11th World
Congress on Pain. Urology 2006 Oct;68(4):697-701.
http://www.ncbi.nlm.nih.gov/pubmed/17070334
47. Leskinen M, Lukkarinen O, Marttila T. Effects of finasteride in patients with inflammatory chronic pelvic
pain syndrome: a double-blind, placebo-controlled, pilot study. Urology 1999 Mar;53(3):502-5.
http://www.ncbi.nlm.nih.gov/pubmed/10096374
48. Kaplan SA, Volpe MA, Te AE. A prospective, 1-year trial using saw palmetto versus finasteride in the
treatment of category III prostatitis/chronic pelvic pain syndrome. J Urol 2004 Jan;171:284-8.
http://www.ncbi.nlm.nih.gov/pubmed/14665895
49. Nickel JC, Downey J, Ardern D, et al. Failure of a monotherapy strategy for difficult chronic prostatitis/
chronic pelvic pain syndrome. J Urol. 2004 Aug;172(2):551-4.
http://www.ncbi.nlm.nih.gov/pubmed/15247727
50. Persson BE, Ronquist G, Ekblom M. Ameliorative effect of allopurinol on nonbacterial prostatitis: a
parallel double-blind controlled study. J Urol 1996 Mar;155(3):961-4.
http://www.ncbi.nlm.nih.gov/pubmed/8583618
51. McNaughton CO, Wilt T. Allopurinol for chronic prostatitis. Cochrane Database Syst Rev
2002;(4):CD001041.
http://www.ncbi.nlm.nih.gov/pubmed/12519549
52. Ziaee AM, Akhavizadegan H, Karbakhsh M. Effect of allopurinol in chronic nonbacterial prostatitis: a
double blind randomized clinical trial. Int Braz J Urol 2006 Mar-Apr;32(2):181-6.
http://www.ncbi.nlm.nih.gov/pubmed/16650295
53. Elist J. Effects of pollen extract preparation Prostat/Poltit on lower urinary tract symptoms in patients
with chronic nonbacterial prostatitis/chronic pelvic pain syndrome: a randomized, double-blind,
placebo-controlled study. Urology 2006 Jan;67(1):60-3.
http://www.ncbi.nlm.nih.gov/pubmed/16413333
54. Wagenlehner FME, Schneider H, Ludwig M, et al. A Pollen Extract (Cernilton) in Patients with
Inflammatory Chronic Prostatitis-Chronic Pelvic Pain Syndrome: A Multicentre, Randomised,
Prospective, Double-Blind, Placebo-Controlled Phase 3 Study. Eur Urol. 2009 Sep;56(3):544-51.
http://www.ncbi.nlm.nih.gov/pubmed/19524353
55. Shoskes DA, Zeitlin SI, Shahed A, et al. Quercetin in men with category III chronic prostatitis: A
preliminary prospective, double-blind, placebo-controlled trial. Urology 1999 Dec;54(6):960-3.
http://www.ncbi.nlm.nih.gov/pubmed/10604689
56. Nickel JC, Forrest JB, Tomera K, et al. Pentosan polysulfate sodium therapy for men with
chronic pelvic pain syndrome: a multicenter, randomized, placebo controlled study. J Urol 2005
Apr;173(4):1252-5.
http://www.ncbi.nlm.nih.gov/pubmed/15758763

38 UPDATE FEBRUARY 2012
57. Pontari MA, Krieger JN, Litwin MS, et al. Pregabalin for the treatment of men with chronic
prostatitis/chronic pelvic pain syndrome: A randomized controlled trial. Arch Intern Med. 2010 Sep
27;170(17):1586-93.
http://www.ncbi.nlm.nih.gov/pubmed/20876412
58. Zermann D, Ishigooka M, Schubert J. Perisphincteric injection of botulinum toxin type A. A treatment
option for patients with chronic prostatic pain? Eur Urol. 2000 Oct;38(4):393-9.
http://www.ncbi.nlm.nih.gov/pubmed/11025376
59. Gottsch HP, Yang CC, Berger RE. A pilot study of botulinum toxin A for male chronic pelvic pain
syndrome. Scand J Urol Nephrol 2010 Nov 9. Epub ahead of print. PubMed PMID:21062115. Scand J
Urol Nephrol. 2011 Feb;45(1):72-6.
http://www.ncbi.nlm.nih.gov/pubmed/21062115
60. Rowe E, Smith C, Laverick L, et al. A prospective, randomized, placebo controlled, double-blind study
of pelvic electromagnetic therapy for the treatment of chronic pelvic pain syndrome with 1 year of
followup. J Urol 2005 Jun;173(6):2044-7.
http://www.ncbi.nlm.nih.gov/pubmed/15879822
61. Montorsi F, Guazzoni G, Bergamaschi F, et al. Is there role for transrectal microwave hyperthermia of
the prostate in the treatment of abacterial prostatitis and prostatodynia? Prostate 1993;22(2):139-46.
http://www.ncbi.nlm.nih.gov/pubmed/8456052
62. Kastner C, Hochreiter W, Huidobro C, et al. Cooled transurethral microwave thermotherapy for
intractable chronic prostatitis-results of a pilot study after 1 year. Urology 2004 Dec;64(6):1149-54.
http://www.ncbi.nlm.nih.gov/pubmed/15596188
63. Zimmermann R, Cumpanas A. Miclea F, et al. Extracorporeal Shock Wave Therapy for the Treatment
of Chronic Pelvic Pain Syndrome in Males: A Randomised, Double-Blind, Placebo-Controlled Study.
Eur Urol. 2009 Sep;56(3):418-24.
http://www.ncbi.nlm.nih.gov/pubmed/19372000
64. Lee SH, Lee BC. Electroacupuncture Relieves Pain in Men With Chronic Prostatitis/Chronic Pelvic
Pain Syndrome: Three-arm Randomized Trial. Urology. 2009 May;73(5):1036-41.
http://www.ncbi.nlm.nih.gov/pubmed/19394499
65. Kabay S, Kabay SC, Yucel M, et al. Efficiency of posterior tibial nerve stimulation in category IIIB
chronic prostatitis/chronic pelvic pain: A sham-controlled comparative study. Urol Int. 2009;83(1):33-8.
http://www.ncbi.nlm.nih.gov/pubmed/19641356
66. FitzGerald MP, Anderson RU, Potts J, et al. Randomized Multicenter Feasibility Trial of Myofascial
Physical Therapy for the Treatment of Urological Chronic Pelvic Pain Syndromes. J Urol. 2009
Aug;182(2):570-80.
http://www.ncbi.nlm.nih.gov/pubmed/19535099
67. Leskinen MJ, Kilponen A, Lukkarinen O, et al. Transurethral needle ablation for the treatment of
chronic pelvic pain syndrome (category III prostatitis): a randomized, sham-controlled study urology
2002 Aug;60(2):300-4.
http://www.ncbi.nlm.nih.gov/pubmed/12137830
68. Aaltomaa S, Ala-Opas M. The effect of transurethral needle ablation on symptoms of chronic pelvic
pain syndrome--a pilot study. Scand J Urol Nephrol. 2001 Apr;35(2):127-31.
http://www.ncbi.nlm.nih.gov/pubmed/11411655
69. Nickel JC, Alexander RB, Anderson R, et al. Category III chronic prostatitis/chronic pelvic pain
syndrome: insights from the National Institutes of Health Chronic Prostatitis Collaborative Research
Network studies.Curr Urol Rep. 2008 Jul;9(4):320-7.
http://www.ncbi.nlm.nih.gov/pubmed/18765132
70. Tripp DA, Nickel JC, Katz L. A feasibility trial of a cognitive-behavioural symptom management
program for chronic pelvic pain for men with refractory chronic prostatitis/chronic pelvic pain
syndrome.Can Urol Assoc J. 2011 Oct;5(5):328-32.
http://www.ncbi.nlm.nih.gov/pubmed/22031613
3.2 Bladder pain syndrome
3.2.1 Introduction
Interstitial cystitis (IC) describes a chronic, distressing bladder condition (1). The so-called ulcer, which is a
typical cystoscopic finding in 10-50% of IC patients, was first described by Guy Hunner at the beginning of
the last century (2,3). Subsequent research (4-6) has shown that IC encompassed a heterogeneous spectrum
of disorders, with different endoscopic and histopathological presentations, with inflammation an important
feature in only a subset of patients. To embrace all patients suffering from bladder pain, the terms painful
bladder syndrome (PBS) or BPS have been suggested as more accurate when referring to pain in the bladder
region, while assuming IC with Hunner’s lesion as a specific type of chronic inflammation of the bladder (7,8).

UPDATE FEBRUARY 2012 39
The term BPS was put forward by the International Society for the Study of BPS (ESSIC) and will be used in
these guidelines. In accordance Classic IC (Hunner’s lesion and inflammation) will be refered to as BPS type 3
C (See Chapter 2, section 2.4 ‘Definitions of CPP terminology’).
3.2.2 Definition
Although generally accepted, the NIDDK criteria provide only a minimum framework to establish the
diagnosis and have been felt to be too restrictive for clinical use (9-12). Recently, the ESSIC has suggested
a standardised scheme of diagnostic criteria (13) to make it easier to compare different studies. BPS was
preferred as the general term to match the current taxonomy of chronic pain syndromes.
3.2.3 Diagnosis
Bladder pain syndrome should be diagnosed on the basis of pain, pressure or discomfort associated
with the urinary bladder, accompanied by at least one other symptom, such as daytime and/or night-time
increased urinary frequency, the exclusion of confusable diseases as the cause of symptoms, and if indicated,
cystoscopy with hydrodistension and biopsy (Table 7) (8).
Table 7: ESSIC classification of types of BPS according to the results of cystoscopy with
hydrodistension and biopsies (8)
Cystoscopy with hydrodistension
Not done Normal Glomerulations
a
Hunner’s lesion
b
Biopsy
Not done XX 1X 2X 3X
Normal XA 1A 2A 3A
Inconclusive XB 1B 2B 3B
Positive
c
XC 1C 2C 3C
a
Cystoscopy: glomerulations grade 2-3
b
Lesion per Fall’s definition with/without glomerulations
c
Histology showing inflammatory infiltrates and/or detrusor mastocytosis and/or granulation tissue and/or
intrafascicular fibrosis.
Beyond subtyping, recent work has indicated the need to phenotype BPS patients. The - Urinary,
Psychosocial, Organ Specific, Inflammation, Neurological/Systemic, Tenderness - UPOINT phenotyping
system classifies patients according to clinically relevant domains, facilitating the use and appraisal of
multimodal therapies (14).
3.2.4 Pathogenesis
Current thought implicates an initial unidentified insult to the bladder, triggering inflammatory, endocrine and
neural phenomena (15-17). This may happen in patients with an underlying systemic defect. In fact, BPS is
similar and frequently precedes, coexists or follows other so-called functional somatic syndromes (FSSs),
occurring predominantly in women, with pain as the main symptom, no abnormal laboratory or anatomical
findings, and exacerbated by stress, namely fibromyalgia (FM), IBS and chronic fatigue syndrome (CFS) (17-
19). At the bladder level, multiple aetiological or pathophysiological mechanisms have been and are still sought
after.
No infection has as yet been implicated (20-25). BPS patients and controls have equal UTI frequency (18,26).
Nevertheless, UTI and urgency are significantly more frequent during childhood and adolescence, in patients
who later develop BPS in adulthood (27). Pancystitis, with associated perineural inflammatory infiltrates, is an
essential part of BPS type 3 C (23), but is scant in non-ulcer BPS (6). There is a 10-fold increase in the mast cell
count in bladder tissue from patients with BPS type 3 C compared with controls. Mast-cell-secreted mediators
(28,29) can indeed induce symptoms and findings of BPS type 3 C (30). In non-ulcer BPS, however, the mast
cell count is normal or only slightly increased (6,29,31,32).
Cystoscopic and biopsy findings in both ulcer and non-ulcer BPS are consistent with defects in the urothelial
glycosaminoglycan (GAG) layer, which might expose the submucosal nerve filaments to noxious urine
components (33-37). Furthermore, urinary uronate, and sulphated GAG levels are increased in patients
with severe BPS (38). Uroplakin III-delta 4, caveolin-1, acid-sensing channels 2a and 3, muscarinic (M2-5)

40 UPDATE FEBRUARY 2012
and purinergic receptors (P2X2 and P2X1), bradykinin B1 receptor, and cannabinoid receptor CB1 are also
upregulated and bladder urothelial sensitivity to carbachol enhanced in urothelial cells of BPS patients (39-
41). In contrast, tight junction proteins zona occludens-1, junctional adherins molecule -1, and occludin
genes are downregulated. Luminal nitric oxide (NO) urinary levels and inducible NO synthetase activity (iNOS)
are increased in BPS patients (43). Urinary NO is significantly increased in ulcer patients and decreases
with treatment, but not in non-ulcer BPS patients (44). iNOS-dependent NO production may have a role in
urothelial dysfunction (44). Altogether, these data further point to increased urothelial permeability. Moreover,
constituents of urine may exert a cytotoxic effect (45), especially in situations such as altered urothelial
barrier or existence of unsialylated Tamm-Horsefall protein observed in BPS (46,47). Along with altered gene
regulation, post translational epigenetic conditioning through micro RNA interference with messenger RNA
transcription, may perpetuate the answer to agression mode, induced on urethelial cells by an initial insult
(39,48).
Microvascular alterations are present in BPS. Despite unaltered number of microvessels, the ratio of mature to
total vessels is significantly lower (49) and decreased bladder perfusion upon filling is observed in BPS patients
(50). Adding to that, proangiogenic vascular endothelial growth factor and hypoxia inducible factor (HIF)-1
expression is increased in the urothelium of BPS patients (49,51).
Involvement of neurogenic inflammation as the trigger to a cascade of events in BPS has been confirmed by
multiple observations documenting its occurrence, followed by neuroplasticity and neuronal sensitisation, both
in the peripheral and CNS of BPS patients. Thus, bladder sensory nerve fibres can induce bladder wall events
through neurogenic inflammation sparked by an initial insult, as well as pain regionalisation and centralisation.
In fact, several data have shown enhanced bladder peripheral nerve density and increased peripheral
neuromediator release, along with neurotrophin and nerve fibre receptor increases, especially in sensory and
sympathetic nerves. Furthermore, besides cytokines from umbrella cells, activation of mast cells in close
proximity to nerve terminals can be influenced by oestradiol as well as corticotrophin-releasing hormone (52-
58). Regionalisation of pain is observed frequently in BPS patients (59). Moreover, autonomic responses and
CNS processing of afferent stimuli are altered in patients with BPS (55,59,60).
Some of the clinical and histopathological characteristics are similar to autoimmune phenomena. However,
only some BPS patients demonstrate autoantibodies, immune deposits or complement activation (61-68). Of
note, differing T-cell infiltrates and B-cell nodules are seen in BPS type 3 C (69).
3.2.5 Epidemiology
Reports of the prevalence of BPS have varied greatly, along with the diagnostic criteria and populations
studied. Recent reports generally show higher figures than earlier ones, ranging from 0.06% to 30% (71-80)
There is a female predominance of about 10:1 (4,71,81,82) but contrary to prior belief, possibly no difference
in race or ethnicity (80-83). The relative proportions of classic and non-ulcer disease are unclear. Incidence in
various studies has ranged from 5 to 50% (5,12,86,87).
Evidence that BPS may have a genetic component has been presented in several studies, but
may contribute to less than one third of total variation in susceptibility for BPS, with the remainder being
environmental (19,88-91).
BPS has significant economic costs. Direct annual costs in the USA have been estimated to be $750
million (92).
3.2.6 References
1. Skene AJC. Diseases of the bladder and urethra in women. New York: William Wood 1887;167.
http://www.archive.org/stream/diseasesofbladd00sken
2. Hunner GL. A rare type of bladder ulcer in women: report of cases. Boston Med Surg J 1915;172:
660-4.
3. Hunner G. Elusive ulcer of the bladder: further notes on a rare type of bladder ulcer with report of 25
cases. Am J Obstet 1918;78:374-95.
4. Hand JR. Interstitial cystitis: report of 223 cases (204 women and 19 men). J Urol. 1949 Feb;61(2):
291-310.
http://www.ncbi.nlm.nih.gov/pubmed/18111850
5. Messing EM, Stamey TA. Interstitial cystitis: early diagnosis, pathology, and treatment. Urology 1978
Oct;12(4):381-92.
http://www.ncbi.nlm.nih.gov/pubmed/213864

UPDATE FEBRUARY 2012 41
6. Fall M, Johansson SL, Aldenborg F. Chronic interstitial cystitis: a heterogeneous syndrome. J Urol
1987 Jan;137(1):35-8.
http://www.ncbi.nlm.nih.gov/pubmed/3795363
7. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function:
report from the Standardisation Subcommitte of the International Continence Society. Am J Obstet
Gynecol 2002 Jul;187(1):116-26.
http://www.ncbi.nlm.nih.gov/pubmed/12114899
8. van de Merwe JP, Nordling J, Bouchelouche P, et al. Diagnostic criteria, classification, and
nomenclature for painful bladder syndrome/interstitial cystitis: an ESSIC poposal. Eur Urol 2008
Jan;53(1):60-7.
http://www.ncbi.nlm.nih.gov/pubmed/17900797
9. Gillenwater JY, Wein AJ. Summary of the National Institute of Arthritis, Diabetes, Digestive and Kidney
Diseases Workshop on Interstitial Cystitis, National Institutes of Health, Bethesda, Maryland, August
28-29,1987. J Urol 1988 Jul;140(1):203-6.
http://www.ncbi.nlm.nih.gov/pubmed/3379688
10. Hanno PM, Landis JR, Matthews-Cook Y, et al. The diagnosis of interstitial cystitis revisited: lessons
learned from the National Institutes of Health Interstitial Cystitis Database study. J Urol 1999
Feb;161(2):553-7.
http://www.ncbi.nlm.nih.gov/pubmed/9915447
11. Erickson DR, Belchis DA, Dabbs DJ. Inflammatory cell types and clinical features of interstitial cystitis.
J Urol 1997 Sep;158(3 Pt 1):790-3.
http://www.ncbi.nlm.nih.gov/pubmed/9258082
12. Peeker R, Fall M. Toward a precise definition of interstitial cystitis: further evidence of differences in
classic and nonulcer disease. J Urol 2002 Jun;167(6):2470-2.
http://www.ncbi.nlm.nih.gov/pubmed/11992059
13. Nordling J, Anjum FH, Bade JJ, et al. Primary evaluation of patients suspected of having interstitial
cystitis (IC). Eur Urol 2004 May;45(5):662-9.
http://www.ncbi.nlm.nih.gov/pubmed/15082211
14. Nickel JC, Shoskes D, Irvine-Bird K. Clinical phenotyping of women with interstitial cystitis/painful
bladder syndrome: a key to classification and potentially improved management. J Urol. 2009
Jul;182(1):155-60.
http://www.ncbi.nlm.nih.gov/pubmed/19447429
15. Elbadawi A. Interstitial cystitis: a critique of current concepts with a new proposal for pathologic
diagnosis and pathogenesis. Urology. 1997 May;49(5A Suppl):14-40.
http://www.ncbi.nlm.nih.gov/pubmed/9145999
16. Okragly AJ, Niles AL, Saban R, et al. Elevated tryptase, nerve growth factor,neurotrophin-3 and
glial cell line-derived neurotrophic factor levels in theurine of interstitial cystitis and bladder cancer
patients. J Urol. 1999 Feb;161(2):438-41.
http://www.ncbi.nlm.nih.gov/pubmed/9915421
17. Warren JW, Wesselmann U, Morozov V, et al. Numbers and types of non bladder syndromes as risk
factors for interstitial cystitis/painful bladder syndrome. Urology. 2011 Feb;77(2):313-9.
http://www.ncbi.nlm.nih.gov/pubmed/21295246
18. Nickel JC, Shoskes DA, Irvine-Bird K. Prevalence and impact of bacteriuria and/or urinary tract
infection in interstitial cystitis/painful bladder syndrome. Urology. 2010 Oct;76(4):799-803.
http://www.ncbi.nlm.nih.gov/pubmed/20573386
19. Talati A, Ponniah K, Strug LJ, et al. Panic disorder, social anxiety disorder, and a possible medical
syndrome previously linked to chromosome 13.Biol Psychiatry. 2008 Mar 15;63(6):594-601.
http://www.ncbi.nlm.nih.gov/pubmed/17920564
20. Domingue GJ, Ghoniem GM, Bost KL, et al. Dormant microbes in interstitial cystitis. Erratum in: J Urol
1996;155:298. J Urol 1995 Apr;153(4):1321-6.
http://www.ncbi.nlm.nih.gov/pubmed/7869536
21. Lynes WL, Sellers RG, Dairiki Shortliffe LM. The evidence for occult bacterial infections as a cause for
interstitial cystitis. J Urol 1989;141:268A (abstr 393).
22. Hukkanen V, Haarala M, Nurmi M, et al. Viruses and interstitial cystitis: adenovirus genomes cannot be
demonstrated in urinary bladder biopsies. Urol Res 1996;24(4):235-8.
http://www.ncbi.nlm.nih.gov/pubmed/8873382
23. Fall M, Johansson SL, Vahlne A. A clinicopathological and virological study of interstitial cystitis. J Urol
1985 May;133(5):771-3.
http://www.ncbi.nlm.nih.gov/pubmed/2985831

42 UPDATE FEBRUARY 2012
24. Duncan JL, Schaeffer AJ. Do infectious agents cause interstitial cystitis? Urology 1997 May;49(5A
Suppl):48-51.
http://www.ncbi.nlm.nih.gov/pubmed/9146001
25. Al-Hadithi HN, Williams H, Hart CA, et al. Absence of bacterial and viral DNA in bladder biopsies from
patients with interstitial cystitis/chronic pelvic pain syndrome. J Urol 2005 Jul;174(1):151-4.
http://www.ncbi.nlm.nih.gov/pubmed/15947607
26. Warren JW, Brown V, Jacobs S, et al. Urinary Tract Infection and Inflammation at Onset of Interstitial
Cystitis/Painful bladder Syndrome. Urology. 2008 Jun;71(6):1085-90.
http://www.ncbi.nlm.nih.gov/pubmed/18538691
27. Peters KM, Killinger KA, Ibrahim IA. Childhood symptoms and events in women with interstitial
cystitis/painful bladder syndrome. Urology. 2009 Feb;73(2):258-62.
http://www.ncbi.nlm.nih.gov/pubmed/19036420
28. Agarwal M, Dixon RA. A study to detect Helicobacter pylori in fresh and archival specimens from
patients with interstitial cystitis, using amplification methods. BJU Int 2003 Jun;91(9):814-6.
http://www.ncbi.nlm.nih.gov/pubmed/12780839
29. Peeker R, Enerback L, Fall M, et al. Recruitment, distribution and phenotypes of mast cells in
interstitial cystitis. J Urol 2000 Mar;163(3):1009-15.
http://www.ncbi.nlm.nih.gov/pubmed/10688040
30. Richter B, Roslind A, Hesse U, et al. YKL-40 and mast cells are associated with detrusor fibrosis in
patients diagnosed with bladder pain syndrome/interstitial cystitis according to the 2008 criteria of the
European Society for the Study of Interstitial Cystitis.Histopathology. 2010 Sep;57(3):371-83.
http://www.ncbi.nlm.nih.gov/pubmed/20840668
31. Dundore PA, Schwartz AM, Semerjian H. Mast cell counts are not useful in the diagnosis of
nonulcerative interstitial cystitis. J Urol 1996 Mar;155(3):885-7.
http://www.ncbi.nlm.nih.gov/pubmed/8583599
32. Wyndaele JJ, Van Dyck J, Toussaint N. Cystoscopy and bladder biopsies in patients with bladder pain
syndrome carried out following ESSIC guidelines. Scand J Urol Nephrol. 2009;43(6):471-5.
http://www.ncbi.nlm.nih.gov/pubmed/19707951
33. Johansson SL, Fall M. Clinical features and spectrum of light microscopic changes in interstitial
cystitis. J Urol 1990 Jun;143(6):1118-24.
http://www.ncbi.nlm.nih.gov/pubmed/2342171
34. Anderström CR, Fall M, Johansson SL. Scanning electron microscopic findings in interstitial cystitis.
Br J Urol 1989 Mar;63(3):270-5.
http://www.ncbi.nlm.nih.gov/pubmed/2702424
35. Fellows GJ, Marshall DH. The permeability of human bladder epithelium to water and sodium. Invest
Urol 1972 Jan;9(4):339-44.
http://www.ncbi.nlm.nih.gov/pubmed/5058772
36. Parsons CL, Mulholland SG. Successful therapy of interstitial cystitis with pentosanpolysulfate. J Urol
1987 Sep;138(3):513-6.
http://www.ncbi.nlm.nih.gov/pubmed/2442417
37. Parsons CL, Lilly JD, Stein P. Epithelial dysfunction in nonbacterial cystitis (interstitial cystitis). J Urol
1991 Apr;145(4):732-5.
http://www.ncbi.nlm.nih.gov/pubmed/2005689
38. Lokeshwar VB, Selzer MG, Cerwinka WH, et al. Urinary uronate and sulfated glycosaminoglycan
levels: markers for interstitial cystitis severity. J Urol 2005 Jul;174(1):344-9.
http://www.ncbi.nlm.nih.gov/pubmed/15947687
39. Sánchez-Freire V, Blanchard MG, Burkhard FC, et al. Acid-Sensing Channels in Human Bladder:
Expression, Function and Alterations During Bladder Pain Syndrome. J Urol. 2011 Oct;186(4):1509-16.
http://www.ncbi.nlm.nih.gov/pubmed/21855903
40. Gupta GN, Lu S, Gold MS, et al. Bladder Urothelial Cells From Patients With Interstitial Cystitis Have
an Increased Sensitivity to Carbachol. Neurourol Urodyn. 2009;28(8):1022-7.
http://www.ncbi.nlm.nih.gov/pubmed/19283864
41. Lin XC, Zhang QH, Zhou P, et al. Caveolin-1 may participate in the pathogenesis of bladder pain
syndrome/interstitial cystitis. Urol Int. 2011;86(3):334-9.
http://www.ncbi.nlm.nih.gov/pubmed/21335944
42. Ehrén I, Hosseini A, Lundberg JO, et al. Nitric oxide: a useful gas in the detection of lower urinary tract
inflammation. J Urol 1999 Aug;162(2):327-9.
http://www.ncbi.nlm.nih.gov/pubmed/10411031

UPDATE FEBRUARY 2012 43
43. Logadottir YR, Ehren I, Fall M, et al. Intravesical nitric oxide production iscriminates between classic
and nonulcer interstitial cystitis. J Urol 2004 Mar;171(3):1148-50; discussion 50-1.
http://www.ncbi.nlm.nih.gov/pubmed/14767289
44. Birder LA, Wolf-Johnston A, Buffington CA, et al. Altered inducible nitricoxide hase expression and
nitric oxide production in the bladder of cats with feline interstitial cystitis. J Urol 2005 Feb;173(2):
625-9.
http://www.ncbi.nlm.nih.gov/pubmed/15643277
45. Parsons CL, Bautista SL, Stein PC, et al. Cyto-injury factors in urine: a possible mechanism for the
development of interstitial cystitis. J Urol 2000 Oct;164(4):1381-4.
http://www.ncbi.nlm.nih.gov/pubmed/10992419
46. Hang L, Wullt B, Shen Z, et al. Cytokine repertoire of epithelial cells lining the human urinary tract.
J Urol 1998 Jun;159(6):2185-92.
http://www.ncbi.nlm.nih.gov/pubmed/9598567
47. Parsons CL, Stein P, Zupkas P, et al. Defective Tamm-Horsfall protein in patients with interstitial
cystitis. J Urol 2007 Dec;178(6):2665-70.
http://www.ncbi.nlm.nih.gov/pubmed/17945284
48. Sanchez Freire V, Burkhard FC, Kessler TM, et al. MicroRNAs may mediate the down-regulation of
neurokinin-1 receptor in chronic bladder pain syndrome. Am J Pathol. 2010 Jan;176(1):288-303.
http://www.ncbi.nlm.nih.gov/pubmed/20008142
49. Kiuchi H, Tsujimura A, Takao T, et al. Increased vascular endothelial growth factor expression
in patients with bladder pain syndrome/interstitial cystitis: its association with pain severity and
glomerulations. BJU Int. 2009 Sep;104(6):826-31.
http://www.ncbi.nlm.nih.gov/pubmed/19298410
50. Pontari MA, Hanno PM, Ruggieri MR. Comparison of bladder blood flow in patients with and without
interstitial cystitis. J Urol 1999 Aug;162(2):330-4.
http://www.ncbi.nlm.nih.gov/pubmed/10411032
51. Lee JD, Lee MH. Increased Expression of Hypoxia-inducible Factor-1 and Vascular Endothelial
Growth Factor Associated With Glomerulation Formation in Patients With Interstitial Cystitis. Urology.
2011 Oct;78(4):971.e11-5.
http://www.ncbi.nlm.nih.gov/pubmed/21813166
52. Abdel-Mageed AB, Ghoniem GM. Potential role of rel/nuclear factor-kappaB in the pathogenesis of
interstitial cystitis. J Urol 1998 Dec;160(6 Pt 1):2000-3.
http://www.ncbi.nlm.nih.gov/pubmed/9817309
53. Abdel-Mageed A, Ghoniem G, Human I, et al. Induction of proinflammatory cytokine gene expression
by NF-kappaB in human bladder epithelial (T-24) cells: possible mechanism for interstitial cystitis.
J Urol 1999;161(Suppl):28.
54. Hohenfellner M, Nunes L, Schmidt RA, et al. Interstitial cystitis: increased sympathetic innervation and
related neuropeptide synthesis. J Urol 1992 Mar;147(3):587-91.
http://www.ncbi.nlm.nih.gov/pubmed/1538434
55. Twiss CO, Kilpatrick L, Triaca V, et al. Evidence for central hyperexitability in patients with interstitial
cystitis. J Urol 2007 Jun;177(4):49.
56. Theoharides TC, Pang X, Letourneau R, et al. Interstitial cystitis: a neuroimmunoendocrine disorder.
Ann N Y Acad Sci 1998 May;840:619-34.
http://www.ncbi.nlm.nih.gov/pubmed/9629289
57. Okragly AJ, Niles AL, Saban R, et al. Elevated tryptase, nerve growth factor, neurotrophin-3 and
glial cell line-derived neurotrophic factor levels in the urine of interstitial cystitis and bladder cancer
patients. J Urol 1999 Feb;161(2):438-41; discussion 441-2.
http://www.ncbi.nlm.nih.gov/pubmed/9915421
58. Boucher W, Kempuraj D, Michaelian M, et al. Corticotropin-releasing hormone-receptor 2 is required
for acute stress-induced bladder vascular permeability and release of vascular endothelial growth
factor. BJU Int. 2010 Nov;106(9):1394-9.
http://www.ncbi.nlm.nih.gov/pubmed/20201838
59. Warren JW, Langenberg P, Greenberg P, et al. Sites of pain from interstitial cystitis/painful bladder
syndrome. J Urol. 2008 Oct;180(4):1373-7.
http://www.ncbi.nlm.nih.gov/pubmed/18707715
60. Yilmaz U, Liu YW, Berger RE, et al. Autonomic nervous system changes in men with chronic pelvic
pain syndrome. J Urol 2007 Jun;177(6):2170-4; discussion 2174.
http://www.ncbi.nlm.nih.gov/pubmed/17509311

44 UPDATE FEBRUARY 2012
61. Elbadawi AE, Light JK. Distinctive ultrastructural pathology of nonulcerative interstitial cystitis: new
observations and their potential significance in pathogenesis. Urol Int 1996;56(3):137-62.
http://www.ncbi.nlm.nih.gov/pubmed/8860736
62. Oravisto KJ, Alfthan OS, Jokinen EJ. Interstitial cystitis. Clinical and immunological findings. Scand J
Urol Nephrol 1970;4(1):37-42.
http://www.ncbi.nlm.nih.gov/pubmed/5314306
63. Jokinen EJ, Alfthan OS, Oravisto KJ. Antitissue antibodies in interstitial cystitis. Clin Exp Immunol
1972 Jul;11(3):333-9.
http://www.ncbi.nlm.nih.gov/pubmed/4114472
64. Ochs RL, Stein TW Jr, Peebles CL, et al. Autoantibodies in interstitial cystitis. J Urol 1994
Mar;151(3):587-92.
http://www.ncbi.nlm.nih.gov/pubmed/8308964
65. Tan EM. Antinuclear antibodies: diagnostic markers for autoimmune diseases and probes for cell
biology. Adv Immunol 1989;44:93-151.
http://www.ncbi.nlm.nih.gov/pubmed/2646863
66. von Muhlen CA, Tan EM. Autoantibodies in the diagnosis of systemic rheumatic diseases. Semin
Arthritis Rheum 1995 Apr;24(5):323-58.
http://www.ncbi.nlm.nih.gov/pubmed/7604300
67. Ochs RL. Autoantibodies and interstitial cystitis. Clin Lab Med 1997 Sep;17(3):571-9.
http://www.ncbi.nlm.nih.gov/pubmed/9316774
68. Mattila J. Vascular immunopathology in interstitial cystitis. Clin Immunol Immunopathol 1982
Jun;23(3):648-55.
http://www.ncbi.nlm.nih.gov/pubmed/6981479
69. Mattila J, Linder E. Immunoglobulin deposits in bladder epithelium and vessels in interstitial
cystitis: possible relationship to circulating anti-intermediate filament autoantibodies. Clin Immunol
Immunopathol 1984 Jul;32(1):81-9.
http://www.ncbi.nlm.nih.gov/pubmed/6733983
70. Harrington DS, Fall M, Johansson SL. Interstitial cystitis: bladder mucosa lymphocyte
immunophenotyping and peripheral blood flow cytometry analysis. J Urol 1990 Oct;144(4):868-71.
http://www.ncbi.nlm.nih.gov/pubmed/2204728
71. Oravisto KJ. Epidemiology of interstitial cystitis. Ann Chir Gynaecol Fenn 1975;64(2):75-7.
http://www.ncbi.nlm.nih.gov/pubmed/1137336
72. Held PJ, Hanno PM, Wein AJ. In: Hanno PM, Staskin DR, Krane RJ, Wein AJ, eds. Interstitial Cystitis.
Epidemiology of interstitial cystitis. London: Springer Verlag, 1990, pp. 29-48.
73. Bade JJ, Rijcken B, Mensink HJ. Interstitial cystitis in The Netherlands: prevalence, diagnostic criteria
and therapeutic preferences. J Urol 1995 Dec;154(6):2035-7; discussion 2037-8.
http://www.ncbi.nlm.nih.gov/pubmed/7500452
74. Jones CA, Harris MA, Nyberg L. Prevalence of interstitial cystitisin the United States, Proc Am Urol
Ass J Urol 1994;151(Suppl):423A.
75. Curhan GC, Speizer FE, Hunter DJ, et al. Epidemiology of interstitial cystitis: a population based
study. J Urol 1999 Feb;161(2):549-52.
http://www.ncbi.nlm.nih.gov/pubmed/9915446
76. Leppilahti M, Sairanen J, Tammela TL, et al. Finnish Interstitial Cystitis-Pelvic Pain Syndrome Study
Group. Prevalence of clinically confirmed interstitial cystitis in women: a population based study in
Finland. J Urol 2005 Aug;174(2):581-3.
http://www.ncbi.nlm.nih.gov/pubmed/16006902
77. Temml C, WehrbergerC, Riedl C, et al. Prevalence and correlates for interstitial cystitis symptoms in
women participating in a health screening project. Eur Urol. 2007 Mar;51(3):803-8; discussion 809.
http://www.ncbi.nlm.nih.gov/pubmed/16979286
78. Burkman RT.Chronic pelvic pain of bladder origin: epidemiology, pathogenesis and quality of life.
J Reprod Med 2004 Mar;49(3 Suppl):225-9.
http://www.ncbi.nlm.nih.gov/pubmed/15088860
79. Roberts RO, Bergstralh EJ, Bass SE, et al. Incidence of physician-diagnosed interstitial cystitis in
Olmsted County: a community-based study. BJU Int 2003 Feb;91(3):181-5.
http://www.ncbi.nlm.nih.gov/pubmed/12581000
80. Parsons CL, Tatsis V. Prevalence of interstitial cystitis in young women. Urology. 2004 Nov;64(5):
866-70.
http://www.ncbi.nlm.nih.gov/pubmed/15533465
81. Greenberg E, Barnes R, Stewart S, et al. Transurethral resection of Hunner’s ulcer. J Urol 1974
Jun;111(6):764-6.
http://www.ncbi.nlm.nih.gov/pubmed/4830879

UPDATE FEBRUARY 2012 45
82. Koziol JA. Epidemiology of interstitial cystitis. Urol Clin North Am 1994 Feb;21(1):7-20.
http://www.ncbi.nlm.nih.gov/pubmed/8284848
83. Berry SH, Elliott MN, Suttorp M, et al. Prevalence of symptoms of bladder pain syndrome/interstitial
cystitis among adult females in the United States. J Urol. 2011 Aug;186(2):540-4.
http://www.ncbi.nlm.nih.gov/pubmed/21683389
84. Barry MJ, Link CL, McNaughton-Collins MF, et al. Boston Area Community Health (BACH)
Investigators. Overlap of different urological symptom complexes in a racially and ethnically diverse,
community-based population of men and women. BJU Int. 2008 Jan;101(1):45-51.
http://www.ncbi.nlm.nih.gov/pubmed/17868419
85. Song Y, Zhang W, Xu B, et al. Prevalence and correlates of painful bladder syndrome symptoms in
Fuzhou Chinese women. Neurourol Urodyn. 2009;28(1):22-5.
http://www.ncbi.nlm.nih.gov/pubmed/18671294
86. Parsons CL. Interstitial cystitis: clinical manifestations and diagnostic criteria in over 200 cases.
Neurourol Urodynam 1990;9:241.
http://onlinelibrary.wiley.com/doi/10.1002/nau.1930090302/abstract
87. Koziol JA, Adams HP, Frutos A. Discrimination between the ulcerous and the nonulcerous forms of
interstitial cystitis by noninvasive findings. J Urol 1996 Jan;155(1):87-90.
http://www.ncbi.nlm.nih.gov/pubmed/7490906
88. Parsons CL, Zupkas P, Parsons JK. Intravesical potassium sensitivity in patients with interstitial
cystitis and urethral syndrome. Urology 2001 Mar;57(3):428-32; discussion 432-3.
http://www.ncbi.nlm.nih.gov/pubmed/11248610
89. Warren J, Jackson T, Meyers D, et al. Fishbein/interstitial cystitis association (ICA) survey of interstitial
cystitis among family members of ICA members: preliminary analysis. Urology 2001 Jun;57(6 Suppl 1):
126-7.
http://www.ncbi.nlm.nih.gov/pubmed/11378121
90. Warren JW, Keay SK, Meyers D, et al. Concordance of interstitial cystitis in monozygotic and dizygotic
twin pairs. Urology 2001 Jun;57(6 Suppl 1):22-5.
http://www.ncbi.nlm.nih.gov/pubmed/11378045
91. Altman D, Lundholm C, Milsom I, et al. The genetic and environmental contribution to the occurrence
of bladder pain syndrome: an empirical approach in a nationwide population sample. Eur Urol. 2011
Feb;59(2):280-5.
http://www.ncbi.nlm.nih.gov/pubmed/21056533
92. Clemens JQ, Meenan RT, Rosetti MC et al. Costs of interstitial cystitis in a managed care population.
Urology. 2008 May;71(5):776-80
http://www.ncbi.nlm.nih.gov/pubmed/18329077
3.2.7 Association with other diseases
An association has been reported between BPS and non-bladder syndromes (NBSs) - IBS, FM, CFS,
vulvodynia, depression, panic disorders, migraine, sicca syndrome, temporomandibular joint disorder, allergy,
asthma, systemic lupus erythematosus, inflammatory bowel disease (1-7). Risk of BPS correlates with number
of NBSs in each patient (8). Recent work showing non-ulcer BPS to have significantly more FM, migraine,
temporomandibular joint disorder and depression than ulcer patients emphasises the need for subtyping (9).
3.2.8 Diagnosis
The diagnosis of BPS is one of exclusion, using symptoms, examination, urine analysis, cystoscopy with
hydrodistension, and biopsy (Figure 6).
The nature of the pain is the key symptom of the disease:
• Pain,pressureordiscomfortperceivedtoberelatedtothebladder,increasingwithincreasingbladder
content.
• Itislocatedsuprapubically,sometimesradiatingtothegroins,vagina,rectumorsacrum.
• Painisrelievedbyvoidingbutsoonreturns(10-14).
• Painisaggravatedbyfoodordrink(13).
The differences between the two BPS subtypes, BPS type 3 C and non-ulcer, include clinical presentation,
age distribution (15), molecular features (16-22), which may be discriminated non-invasively (23), and response
to treatment (24-27). BPS type 3 C is a highly damaging inflammation that often leads to a small-capacity
fibrotic bladder or upper urinary tract outflow obstruction. This type of progression is not observed in non-
ulcer disease (14,28). Endoscopically, BPS type 3 C displays reddened mucosal areas often associated
with small vessels radiating towards a central scar, sometimes covered by a small clot or fibrin deposit - the
Hunner lesion (14). The scar ruptures with increasing bladder distension, producing a characteristic waterfall-

46 UPDATE FEBRUARY 2012
type of bleeding. There is a strong association between BPS type 3 C and reduced bladder capacity under
anaesthesia (14,29,30).
Cystoscopy
Non-ulcer disease displays a normal bladder mucosa at initial cystoscopy. The development of glomerulations
after hydrodistension is considered to be a positive diagnostic sign. A recent report has shown that there is no
difference in the cystoscopic appearance between patients with non-ulcer disease and women without bladder
symptoms about to undergo tubal ligation (31). The observation of glomerulations may however not always be
constant over time (32).
Some authors maintain that cystoscopy with hydrodistension provides little useful information in
addition to the history and physical examination findings (33,34). In contrast, others have found a strong
correlation between pain and cystoscopic findings in patients with untreated BPS, and this difference from the
results of other studies may have been due to treatment effects (35). Glomerulations may be involved in the
disease mechanism, because such findings are highly associated with overexpression of angiogenic growth
factors in the bladder and neovascularisation (36). A recent pilot study has demonstrated feasibility of bladder
distension and biopsy under local anaesthesia (37). ESSIC believes objective findings are important and that
a standardised scheme of diagnostic criteria would help improve the uniformity and comparability of different
studies (38).
Biopsies are helpful in establishing or supporting the clinical diagnosis of both classic and non-ulcer types of
the disease (17, 38-41). Important differential diagnoses to exclude by histological examination are carcinoma
in situ and tuberculous cystitis.
Potassium chloride bladder permeability test has been used in the diagnosis of BPS (41), but recent reports
have suggested that it lacks discriminating power (42,43). A modified test using less concentrated solution has
been suggested. This test, although painless in contrast to the original procedure, decreases the maximum
cystometric volume in 90% of patients with BPS, but not in controls (44). Furthermore, it has been suggested
that the potassium sensitivity test can help to predict the response to GAG treatment (45).
Symptom scores may help to describe symptoms in an individual patient and as outcome measures. The
O’Leary-Sant Symptom Index, also known as the Interstitial Cystitis Symptom Index (ICSI) has recently been
validated successfully in a large study (46).
Biological markers. It is an attractive idea to support or, even better, to confirm the clinical diagnosis using a
biological marker. Finding a universally helpful one is hampered by heterogeneity within the diagnostic group
of BPS. Antiproliferative factor, heparin-binding epidermal growth factor-like growth factor, uroplakin III delta-4
mRNA, and YKL-40 have all presented as potential candidates (47-49). NO is interesting because of its ability
to discriminate classic from non-ulcer disease with minimal invasiveness. However, all putative markers to date
have yet to be validated (50).
3.2.9 BPS in children and males
According to NIDDK criteria, children aged < 18 years is an exclusion criterion. However, occasional cases
of BPS of both subtypes have been identified in patients under this age (51). There is increasing evidence
that children aged 2-11 may also be affected, although prevalence figures are low (52). Thus, BPS cannot be
excluded on the basis of age.
It has been argued that PPS and BPS are inter-related (53,54). However, differences in urinary markers suggest
that BPS and PPS are different disorders with distinct pathophysiology (55).

UPDATE FEBRUARY 2012 47
3.2.10 Conclusions and recommendations: assessment and diagnosis BPS
Conclusions LE
BPS has no known single aetiology. 3
Pain in BPS does not correlate with bladder cystoscopic or histologic findings. 2a
BPS Type 3 C is not surely distinguishable by non-invasive means. 2a
Ulcer non-ulcer disease ratios of BPS are highly variable between studies. 2a
The prevalence of BPS-like symptoms is high in population-based studies. 2a
BPS associated non bladder diseases are extremely prevalent, differ in BPS subtypes and correlate
with BPS risk.
2a
BPS has a high impact on quality of life. 2a
There is significant overlap of symptoms with other conditions. 2a
Reliable instruments assessing symptom severity as well as phenotypical differences exist. 2a
Recommendations GR
Specific diseases with similar symptoms have to be excluded. It is therefore recommended to adapt
diagnostic procedures to each patient and aim at identifying them.
A
After primary exclusion of specific diseases, patients with symptoms according to the above
definition should be diagnosed with BPS by subtype and phenotype.
A
A validated symptom and quality of life scoring instrument should be considered for initial
assessment as well as for follow-up.
B
BPS associated non bladder diseases should be assessed systematically. A
BPS associated negative cognitive, behavioural, sexual, or emotional consequences should be
assessed.
A
BPS = Bladder pain syndrome.
3.2.11 References
1. Warren J, Jackson T, Meyers D, et al. Fishbein/interstitial cystitis association (ICA) survey of interstitial
cystitis among family members of ICA members: preliminary analysis. Urology. 2001 Jun;57(6 Suppl
1):126-7.
http://www.ncbi.nlm.nih.gov/pubmed/11378121
2. Warren JW, Howard FM, Cross RK, et al. Antecedent nonbladder syndromes in case-control study of
interstitial cystitis/painful bladder syndrome. Urology. 2009 Jan;73(1):52-7.
http://www.ncbi.nlm.nih.gov/pubmed/18995888
3. Alagiri M, Chottiner S, Ratner V, et al. Interstitial cystitis: unexplained associations with other chronic
disease and pain syndromes. Urology 1997 May;49(5A Suppl):52-7.
http://www.ncbi.nlm.nih.gov/pubmed/9146002
4. Clauw DJ, Schmidt M, Radulovic D, et al. The relationship between fibromyalgia and interstitial
cystitis. J Psychiatr Res 1997 Jan-Feb;31(1):125-31.
http://www.ncbi.nlm.nih.gov/pubmed/9201654
5. Erickson DR, Morgan KC, Ordille S, et al. Nonbladder related symptoms in patients with interstitial
cystitis. J Urol 2001;166(2):557-61 Aug; discussion 561-2.
http://www.ncbi.nlm.nih.gov/pubmed/11458068
6. Weissman MM, Gross R, Fyer A, et al. Interstitial Cystitis and Panic Disorder - A Potential Genetic
Syndrome. Arch Gen Psych 2004;61:273-9.
http://archpsyc.ama-assn.org/cgi/content/abstract/61/3/273
7. Buffington CA. Comorbidity of interstitial cystitis with other unexplained clinical conditions. J Urol
2004 Oct;172(4 Pt 1):1242-8.
http://www.ncbi.nlm.nih.gov/pubmed/15371816
8. Warren JW, Wesselmann U, Morozov V, et al. Numbers and types of nonbladder syndromes as risk
factors for interstitial cystitis/painful bladder syndrome. Urology. 2011 Feb;77(2):313-9.
http://www.ncbi.nlm.nih.gov/pubmed/21295246

48 UPDATE FEBRUARY 2012
9. Peters KM, Killinger KA, Mounayer MH, et al. Are ulcerative and nonulcerative interstitial cystitis/
painful bladder syndrome 2 distinct diseases? A study of coexisting conditions. Urology. 2011
Aug;78(2):301-8.
http://www.ncbi.nlm.nih.gov/pubmed/21703668
10. Bullock AD, Becich MJ, Klutke CG, et al. Experimental autoimmune cystitis: a potential murine model
for ulcerative interstitial cystitis. J Urol 1992 Dec;148(6):1951-6.
http://www.ncbi.nlm.nih.gov/pubmed/1433651
11. Dodd LG, Tello J. Cytologic examination of urine from patients with interstitial cystitis. Acta Cytol 1998
Jul-Aug;42(4):923-7.
http://www.ncbi.nlm.nih.gov/pubmed/9684578
12. Erickson DR, Davies MF. Interstitial cystitis. Int Urogynecol J Pelvic Floor Dysfunct 1998;9(3):174-83.
http://www.ncbi.nlm.nih.gov/pubmed/9745978
13. Warren JW, Brown J, Tracy JK, et al. Evidence-based criteria for pain of interstitial cystitis/painful
bladder syndrome in women. Urology. 2008 Mar;71(3):444-8.
http://www.ncbi.nlm.nih.gov/pubmed/18342184
14. Fall M, Johansson SL, Aldenborg F. Chronic interstitial cystitis: a heterogeneous syndrome. J Urol
1987 Jan;137(1):35-8.
http://www.ncbi.nlm.nih.gov/pubmed/3795363
15. Peeker R, Fall M. Toward a precise definition of interstitial cystitis: further evidence of differences in
classic and nonulcer disease. J Urol 2002 Jun;167(6):2470-2.
http://www.ncbi.nlm.nih.gov/pubmed/11992059
16. Dundore PA, Schwartz AM, Semerjian H. Mast cell counts are not useful in the diagnosis of
nonulcerative interstitial cystitis. J Urol 1996 Mar;155(3):885-7.
http://www.ncbi.nlm.nih.gov/pubmed/8583599
17. Johansson SL, Fall M. Clinical features and spectrum of light microscopic changes in interstitial
cystitis. J Urol 1990 Jun;143(6):1118-24.
http://www.ncbi.nlm.nih.gov/pubmed/2342171
18. Harrington DS, Fall M, Johansson SL. Interstitial cystitis: bladder mucosa lymphocyte
immunophenotyping and peripheral blood flow cytometry analysis. J Urol 1990 Oct;144(4):868-71.
http://www.ncbi.nlm.nih.gov/pubmed/2204728
19. Peeker R, Aldenborg F, Haglid K, et al. Decreased levels of S-100 protein in non-cer interstitial cystitis.
Scand J Urol Nephrol 1998 Dec;32(6):395-8.
http://www.ncbi.nlm.nih.gov/pubmed/9925003
20. Twiss CO, Kilpatrick L, Triaca V, et al. Evidence for central hyperexitability in patients with interstitial
cystitis. J Urol 2007 Jun;177(4):49.
21. Koziol JA, Clark DC, Gittes RF, et al. The natural history of interstitial cystitis: a survey of 374 patients.
J Urol 1993 Mar;149(3):465-9.
http://www.ncbi.nlm.nih.gov/pubmed/8437248
22. Enerbäck L, Fall M, Aldenborg F. Histamine and mucosal mast cells in interstitial cystitis. Agents
Actions 1989 Apr;27(1-2):113-6.
http://www.ncbi.nlm.nih.gov/pubmed/2750582
23. oziol JA, Adams HP, Frutos A. Discrimination between the ulcerous and the nonulcerous forms of
interstitial cystitis by noninvasive findings. J Urol 1996 Jan;155(1):87-90.
http://www.ncbi.nlm.nih.gov/pubmed/7490906
24. Hanno PM. Amitriptyline in the treatment of interstitial cystitis. Urol Clin North Am 1994 Feb;21(1):
89-91.
http://www.ncbi.nlm.nih.gov/pubmed/8284851
25. Fall M, Lindström S. Transcutaneous electrical nerve stimulation in classic and nonulcer interstitial
cystitis. Urol Clin North Am 1994 Feb;21(1):131-9.
http://www.ncbi.nlm.nih.gov/pubmed/8284836
26. Peeker R, Haghsheno MA, Holmang S, et al. Intravesical bacillus Calmette-Guerin and dimethyl
sulfoxide for treatment of classic and nonulcer interstitial cystitis: a prospective, randomized
doubleblind study. J Urol 2000 Dec;164(6):1912-1915; discussion 1915-6.
http://www.ncbi.nlm.nih.gov/pubmed/11061879
27. Fritjofsson A, Fall M, Juhlin R, et al. Treatment of ulcer and nonulcer interstitial cystitis with sodium
pentosanpolysulfate: a multicenter trial. J Urol 1987 Sep;138(3):508-12.
http://www.ncbi.nlm.nih.gov/pubmed/2442416
28. Lechevallier E. Interstitial cystitis. Prog Urol 1995 Feb;5(1):21-30.
http://www.ncbi.nlm.nih.gov/pubmed/7719356

UPDATE FEBRUARY 2012 49
29. Peeker R, Fall M. Toward a precise definition of interstitial cystitis: further evidence of differences in
classic and nonulcer disease. J Urol 2002 Jun;167(6):2470-2.
http://www.ncbi.nlm.nih.gov/pubmed/11992059
30. Messing E, Pauk D, Schaeffer A, et al. Associations among cystoscopic findings and symptoms and
physical examination findings in women enrolled in the Interstitial Cystitis Data Base (ICDB) Study.
Urology 1997 May;49(5A Suppl):81-5.
http://www.ncbi.nlm.nih.gov/pubmed/9146006
31. Waxman JA, Sulak PJ, Kuehl TJ. Cystoscopic findings consistent with interstitial cystitis in normal
women undergoing tubal ligation. J Urol 1998 Nov;160(5):1663-7.
http://www.ncbi.nlm.nih.gov/pubmed/9783927
32. Shear S, Mayer R. Development of glomerulations in younger women with interstitial cystitis.
Urology.2006 Aug;68(2):253-6.
http://www.ncbi.nlm.nih.gov/pubmed/16904429
33. Ottem DP, Teichman JM. What is the value of cystoscopy with hydrodistension for interstitial cystitis?
Urology 2005 Sep;66(3):494-9.
http://www.ncbi.nlm.nih.gov/pubmed/16140064
34. Cole EE, Scarpero HM, Dmochowski RR. Are patient symptoms predictive of the diagnostic and/or
therapeutic value of hydrodistention? Neurourol Urodyn 2005;24(7):638-42.
http://www.ncbi.nlm.nih.gov/pubmed/16208660
35. Lamale LM, Lutgendorf SK, Hoffman AN, et al. Symptoms and cystoscopic findings in patients with
untreated interstitial cystitis. Urology 2006 Feb;67(2):242-5.
http://www.ncbi.nlm.nih.gov/pubmed/16442603
36. Tamaki M, Saito R, Ogawa O, et al. Possible mechanisms inducing glomerulations in interstitialcystitis:
relationship between endoscopic findings and expression of angiogenic growth factors. J Urol 2004
Sep;172(3):945-8.
http://www.ncbi.nlm.nih.gov/pubmed/15311005
37. Nordling J, Anjum FH, Bade JJ, et al. Primary evaluation of patients suspected of having interstitial
cystitis (IC). Eur Urol 2004 May;45(5):662-9.
http://www.ncbi.nlm.nih.gov/pubmed/11992059
38. Aihara K, Hirayama A, Tanaka N, et al. Hydrodistension under local anesthesia for patients with
suspected painful bladder syndrome/interstitial cystitis: safety, diagnostic potential and therapeutic
efficacy. Int J Urol. 2009 Dec;16(12):947-52.
http://www.ncbi.nlm.nih.gov/pubmed/19817916
39. Johansson SL, Fall M. Pathology of interstitial cystitis. Urol Clin North Am 1994 Feb;21(1):55-62.
http://www.ncbi.nlm.nih.gov/pubmed/8284845
40. Geurts N, Van Dyck J, Wyndaele JJ. Bladder pain syndrome: do the different morphological and
cystoscopic features correlate? Scand J Urol Nephrol. 2011 Feb;45(1):20-3.
http://www.ncbi.nlm.nih.gov/pubmed/20846081
41. Parsons CL, Greenberger M, Gabal L, et al. The role of urinary potassium in the pathogenesis and
diagnosis of interstitial cystitis. J Urol 1998 Jun;159(6):1862-6;discussion 1866-7.
http://www.ncbi.nlm.nih.gov/pubmed/9598476
42. Chambers GK, Fenster HN, Cripps S, et al. An assessment of the use of intravesical potassium in the
diagnosis of interstitial cystitis. J Urol 1999 Sep;162(3 Pt 1):699-701.
http://www.ncbi.nlm.nih.gov/pubmed/10458346
43. Grégoire M, Liandier F, Naud A, et al. Does the potassium stimulation test predict cystometric,
cystoscopic outcome in interstitial cystitis? J Urol 2002 Aug;168(2):556-7.
http://www.ncbi.nlm.nih.gov/pubmed/12131308
44. Daha LK, Riedl CR, Hohlbrugger G, et al. Comparative assessment of maximal bladder capacity,
0.9%NaCl versus 0.2 M Kcl, for the diagnosis of interstitial cystitis: a prospective controlled study.
J Urol 2003 Sep;170(3):807-9.
http://www.ncbi.nlm.nih.gov/pubmed/12913704
45. Gupta SK, Pidcock L, Parr NJ. The potassium sensitivity test: a predictor of treatment response in
interstitial cystitis. BJU Int 2005 Nov;96(7):1063-6.
http://www.ncbi.nlm.nih.gov/pubmed/16225529
46. Lubeck DP, Whitmore K, Sant GR, et al. Psychometric validation of the O’leary-Sant interstitial cystitis
symptom index in a clinical trial of pentosan polysulfate sodium. Urology 2001 Jun; 57(6 Suppl 1):
62-6.
http://www.ncbi.nlm.nih.gov/pubmed/11378052

50 UPDATE FEBRUARY 2012
47. Zeng Y, Wu XX, Homma Y, et al. Uroplakin III-delta4 messenger RNA as a promising marker to identify
nonulcerative interstitial cystitis. J Urol. 2007 Oct;178(4 Pt 1):1322-7; discussion 1327.
http://www.ncbi.nlm.nih.gov/pubmed/17698128
48. Richter B, Roslind A, Hesse U, et al. YKL-40 and mast cells are associated with detrusor fibrosis in
patients diagnosed with bladder pain syndrome/interstitial cystitis according to the 2008 criteria of the
European Society for the Study of Interstitial Cystitis. Histopathology. 2010 Sep;57(3):371-83.
http://www.ncbi.nlm.nih.gov/pubmed/20840668
49. Keay S, Kleinberg M, Zhang CO, et al. Bladder epithelial cells from patients with interstitial cystitis
produce an inhibitor of heparin-binding epidermal growth factor-like growth factor production. J Urol
2000 Dec;164(6):2112-8.
http://www.ncbi.nlm.nih.gov/pubmed/11061938
50. Logadottir YR, Ehren I, Fall M, et al. Intravesical nitric oxide production iscriminates between classic
and nonulcer interstitial cystitis. J Urol 2004 Mar;171(3):1148-50; discussion 50-1.
http://www.ncbi.nlm.nih.gov/pubmed/14767289
51. Close CE, Carr MC, Burns MW, et al. Interstitial cystitis in children. J Urol 1996 Aug;156(2 Pt 2):860-2.
http://www.ncbi.nlm.nih.gov/pubmed/8683802
52. Mattox TF. Interstitial cystitis in adolescents and children: a review. J Pediatr Adolesc Gynecol
2004Feb;17(1):7-11.
http://www.ncbi.nlm.nih.gov/pubmed/15010032
53. Miller JL, Rothman I, Bavendam TG, et al. Prostatodynia and interstitial cystitis: one and the same?
Urology 1995 Apr;45(4):587-90.
http://www.ncbi.nlm.nih.gov/pubmed/7716839
54. Pontari MA. Chronic prostatitis/chronic pelvic pain syndrome and interstitial cystitis: are they related?
Curr Urol Rep 2006 Jul;7(4):329-34.
http://www.ncbi.nlm.nih.gov/pubmed/16930505
55. Keay S, Zhang CO, Chai T, et al. Antiproliferative factor, heparin-binding epidermal growth factor-like
growth factor, and epidermal growth factor in men with interstitial cystitis versus chronic pelvic pain
syndrome. Urology 2004 Jan;63(1):22-6.
http://www.ncbi.nlm.nih.gov/pubmed/14751340
3.2.12 Medical treatment
Analgesics. Pain is often a dominant symptom, therefore, many patients try commonly used analgesics at
some stage of the disease. However, pain relief is disappointing because the visceral pain experienced in BPS
responds poorly to analgesic drugs. No systematic studies have been conducted on conventional analgesics.
Short-term opioids may be indicated for breakthrough or exacerbated pain and periodic flare-ups. Long-term
opioids may be considered after all other available therapeutic options have been exhausted. Urologists should
obtain informed consent, arrange for regular follow-up, and be prepared to recognise opioid-induced side
effects (1). BPS is a chronic disease, therefore, long-term opioids should be used only exceptionally and under
close surveillance.
Corticosteroids. Reports on outcome with corticosteroid therapy have been both promising (2) and
discouraging (3). Soucy et al. (4) have suggested a trial of prednisone (25 mg daily for 1-2 months, afterwards
reduced to the minimum required for symptom relief) in patients with severe ulcerative BPS, which is otherwise
unresponsive to conventional treatment. The side effects of steroids can be very serious, making it difficult to
justify their use.
Antiallergics. Mast cells may play a role in BPS. Histamine is one of the substances released by mast cells.
Histamine receptor antagonists have been used to block the H1 (5) as well as the H2 (6) receptor subtypes,
with variable results.
Hydroxyzine is a histamine H1-receptor antagonist, which blocks neuronal activation of mast cells by inhibiting
serotonin secretion from thalamic mast cells and neurons (7). Hydroxyzine hydrochloride (Atarax) is usually
given, starting with 25 mg at bedtime, increasing to 50 mg/day, or if tolerated, 75 mg. The most common
side effects are sedation and generalised weakness, which usually resolve after a period of treatment. In the
first series using hydroxyzine, > 90% of patients showed improvement across the whole range of symptoms.
Interestingly, improvement was noted in associated symptoms including migraine, IBS and allergies (5).
Although these initial results were supported by a further uncontrolled study (5,8), a prospective RCT
of hydroxyzine or sodium pentosan polysulphate compared to placebo failed to show a statistically significant
effect (9). However, the study was underpowered, which may be why it failed to demonstrate a statistically
significant outcome for either drug compared to placebo. Combination therapy showed the highest response

UPDATE FEBRUARY 2012 51
rate of 40%, with a placebo response rate of 13%.
Amitriptyline. The tricyclic antidepressant amitriptyline has alleviated symptoms in BPS, probably via
mechanisms such as blockade of acetylcholine receptors, inhibition of reuptake of released serotonin and
noradrenalin, and blockade of histamine H1 receptors. It is also an anxiolytic agent (10). Several reports have
indicated amelioration after oral amitriptyline (11-13). In a prospective RCT, 48 patients (14) were treated for 4
months with amitriptyline.
Drug dosages were escalated in 25-mg increments at 1-week intervals up to a maximum dosage of
100 mg. Amitriptyline significantly improved the mean symptom score, pain and urgency intensity, whereas
frequency and functional bladder capacity improved but not significantly. In a subsequent, prospective,
open-label study (15), a response rate of 64% with an overall mean dose of 55 mg was seen with long-
term amitriptyline for 20 months. Patient overall satisfaction was good to excellent in 46%, with significant
improvement in symptoms.
A therapeutic response was observed in all 28 patients fulfilling NIDDK criteria and those with a clinical
diagnosis of BPS. Anticholinergic side effects (mouth dryness and weight gain) were common and considered
to be a drawback of amitriptyline. A multicentre, randomised, double-blind, placebo-controlled clinical trial
comparing amitriptyline and placebo plus behavioural modification in 273 patients concluded that amitriptyline
may be beneficial at ≥ 50 mg/daily (16). In clinical practice drowsiness is also a limiting factor with amitriptyline
and a lower starting dose of 10mg is often suggested. Nortriptyline is sometimes considered in place of
amitriptyline when drowsiness is the limiting factor.
Pentosan polysulphate sodium (Elmiron) has been evaluated in double-blind, placebo-controlled studies.
Pentosan polysulphate sodium is thought to substitute for a defect in the GAG layer. Subjective improvement
of pain, urgency, frequency, but not nocturia, has been reported in patients taking the drug compared to
placebo (17,18). In an open multicentre study, pentosan polysulphate sodium had a more favourable effect
in BPS type 3 C than in non-ulcer disease (19). The normal dose is 150-200 mg twice daily between meals.
However, absorption is incomplete. An RCT has compared 300 mg pentosan polysulphate sodium with
evaluated dosages of 600 and 900 mg in 380 BPS patients. Mean ICSI scores improved significantly for all
dosages (20). However, treatment response was not dose-dependent but related more to treatment duration.
At 32 weeks, about half of all patients were responders. Most adverse events were mild and resolved without
intervention. In contrast, a prospective RCT comparing pentosan polysulphate sodium and hydroxyzine
against placebo failed to demonstrate a statistically significant outcome for either drug, although the former
approached statistical significance (P = 0.064) (9). Combination therapy showed the highest response rate of
40% compared to 13% with placebo. For patients with an initial minor response to pentosan polysulphate
sodium, additional subcutaneous administration of heparin appeared to be helpful (21).
Antibiotics have a limited role in the treatment of BPS. A prospective pilot RCT of sequential oral antibiotics
in 50 patients found that overall improvement occurred in 12/25 patients in the antibiotic group and 6/25 in
the placebo group, whereas 10 and 5 patients reported an improvement in pain and urgency, respectively.
Antibiotics alone or in combination may be associated with decreased symptoms in some patients, but do not
represent a major advance in therapy for BPS (22).
Immunosuppressants. Azathioprine, 50-100 mg daily, was given to 38 patients, resulting in disappearance
of pain in 22 and urinary frequency in 20 (23). Cyclosporin A (CyA) (24) and methotrexate (25) were initially
evaluated in open studies, with a good effect on pain, but a limited effect on urgency and frequency.
More recent studies of CyA have reported promising results (26,27). In 23 patients, daily voiding,
maximal bladder capacity, and voided volume improved significantly after 1 year of treatment. The effect was
maintained throughout 5 years follow-up, with 20/23 patients reporting no bladder pain. However, symptoms
recurred within a few months of discontinuing CyA.
In a subsequent randomised study (27), 64 patients fulfilling the NIH criteria were randomised
to 1.5 mg/kg CyA twice daily or low-dose (3x 100 mg) pentosan polysulphate sodium for 6 months. CyA
was superior to pentosan polysulphate sodium in all clinical outcome parameters, with the frequency of
micturition significantly reduced in CyA-treated patients, and clinical global response rates of 75% (CyA) and
19% (pentosan polysulphate sodium) (P < 0.001). However, there were more adverse events in the CyA arm
(including induced hair growth, gingival pain and hyperplasia, paraesthesia in the extremities, abdominal pain,
flushing, muscle pain and shaking), and only 29 patients completed the 6 months follow-up in both groups.
During CyA therapy, careful follow-up is mandatory, including regular blood pressure measurement and serum
creatinine.
Gabapentin is an antiepileptic drug, which is used as adjunctive treatment in painful disorders. Gabapentin

52 UPDATE FEBRUARY 2012
may reduce the use of concomitant therapeutics, such as opioids. Two patients with BPS showed improved
functional capacity and received adequate pain control when gabapentin was added to their regimen (28). In
an uncontrolled dose-escalation protocol with 21 chronic genitourinary pain patients (29), 10 improved with
gabapentin at 6 months. The study included eight BPS patients, of whom, five responded to gabapentin.
Pregabalin is an alpha (2)-delta ligand that binds to and modulates voltage-gated calcium channels, exerting its
intended effect to reduce neuropathic pain (30). Pregabalin is the second of only two medications that are US
FDA-approved for the treatment of neuropathic pain associated with diabetic peripheral neuropathy; it is used
for the treatment of postherpetic neuralgia. Studies on BPS are still lacking.
Suplatast tosilate (IPD-1151T) is an oral immunoregulator that suppresses helper-T-cell-mediated allergic
processes. Fourteen women with BPS treated with suplatast tosilate reported significantly increased bladder
capacity and decreased symptoms after 1 year of treatment. No major side effects occurred and therapeutic
effects correlated with a reduction in blood eosinophils, IgE and urinary T cells (31). Comparative controlled
data are unavailable.
Quercetin is a bioflavonoid that may be effective in male pelvic pain syndrome. It was first tested in a small
open-label study of 29 patients, with hopeful results (32). Theoharides et al. (33) have studied the dietary
supplement CystoProtek formulated from quercetin and the natural GAG components, chondroitin sulphate
and sodium hyaluronate. In an uncontrolled study, symptoms were significantly improved in 37 BPS patients
(NIH criteria), who had failed all forms of therapy and who took six capsules per day for 6 months. Larger
controlled studies are warranted by this result.
3.2.12.1 References
1. Nickel JC. Opioids for chronic prostatitis and interstitial cystitis: lessons learned from the 11th World
Congress on Pain. Urology 2006 Oct;68(4):697-701.
http://www.ncbi.nlm.nih.gov/pubmed/17070334
2. Badenoch AW. Chronic interstitial cystitis. Br J Urol 1971 Dec;43(6):718-21.
http://www.ncbi.nlm.nih.gov/pubmed/5159574
3. Pool TL. Interstitial cystitis: clinical considerations and treatment. Clin Obstet Gynecol 1967
Mar;10(1):185-91.
http://www.ncbi.nlm.nih.gov/pubmed/6021011
4. Soucy F, Grégoire M. Efficacy of prednisone for severe refractory ulcerative interstitial cystitis. J Urol
2005 Mar;173(3):841-3; discussion 843.
http://www.ncbi.nlm.nih.gov/pubmed/15711286
5. Theoharides TC. Hydroxyzine in the treatment of interstitial cystitis. Urol Clin North Am 1994
Feb;21(1):113-9.
http://www.ncbi.nlm.nih.gov/pubmed/8284834
6. Seshadri P, Emerson L, Morales A. Cimetidine in the treatment of interstitial cystitis. Urology 1994
Oct;44(4):614-6.
http://www.ncbi.nlm.nih.gov/pubmed/7941209
7. Theoharides TC. Hydroxyzine for interstitial cystitis. J Allergy Clin Immunol 1993 Feb;91(2):686-7.
http://www.ncbi.nlm.nih.gov/pubmed/8436783
8. Theoharides TC, Sant GR. Hydroxyzine therapy for interstitial cystitis. Urology 1997 May;49(5A
Suppl):108-10.
http://www.ncbi.nlm.nih.gov/pubmed/9146011
9. Sant GR, Propert KJ, Hanno PM, et al; Interstitial Cystitis Clinical Trials Group. A pilot clinical trial
of oral pentosan polysulfate and oral hydroxyzine in patients with interstitial cystitis. J Urol 2003
Sep;170(3):810-5.
http://www.ncbi.nlm.nih.gov/pubmed/12913705
10. Baldessarini RJ. Drugs and the treatment of psychiatric disorders. In: Gilman A, Gooman L, Rall T,
eds. The Pharmacological Basis of Therapeutics. 7th ed. New York: Macmillan, 1985, pp. 387-445.
11. Hand JR. Interstitial cystitis: report of 223 cases (204 women and 19 men). J Urol. 1949 Feb;61(2):291-
310.
http://www.ncbi.nlm.nih.gov/pubmed/18111850
12. Hanno PM, Buehler J, Wein AJ. Use of amitriptyline in the treatment of interstitial cystitis. J Urol 1989
Apr;141(4):846-8.
http://www.ncbi.nlm.nih.gov/pubmed/2926877
13. Kirkemo AK, Miles BJ, Peters JM. Use of amitriptyline in interstitial cystitis. J Urol 1990;143
(Suppl):279A.

UPDATE FEBRUARY 2012 53
14. van Ophoven A, Pokupic S, Heinecke A, et al. A prospective, randomized, placebo controlled,
doubleblind study of amitriptyline for the treatment of interstitial cystitis. J Urol 2004 Aug;172(2):533-6.
http://www.ncbi.nlm.nih.gov/pubmed/15247722
15. van Ophoven A, Hertle L. Long-term results of amitriptyline treatment for interstitial cystitis. J Urol
2005 Nov;174(5):1837-40.
http://www.ncbi.nlm.nih.gov/pubmed/16217303
16. Foster HE Jr, Hanno PM, Nickel JC, et al. Interstitial Cystitis Collaborative Research Network. Effect
of amitriptyline on symptoms in treatment naïve patients with interstitial cystitis/painful bladder
syndrome.J Urol. 2010 May;183(5):1853-8.
http://www.ncbi.nlm.nih.gov/pubmed/20303115
17. Mulholland SG, Hanno P, Parsons CL, et al. Pentosan polysulfate sodium for therapy of interstitial
cystitis. A double-blind placebo-controlled clinical study. Urology 1990 Jun;35(6):552-8.
http://www.ncbi.nlm.nih.gov/pubmed/1693797
18. Hwang P, Auclair B, Beechinor D, et al. Efficacy of pentosan polysulfate in the treatment of interstitial
cystitis: a meta-analysis. Urology 1997 Jul;50(1):39-43.
http://www.ncbi.nlm.nih.gov/pubmed/9218016
19. Fritjofsson A, Fall M, Juhlin R, et al. Treatment of ulcer and nonulcer interstitial cystitis with sodium
pentosanpolysulfate: a multicenter trial. J Urol 1987 Sep;138(3):508-12.
http://www.ncbi.nlm.nih.gov/pubmed/2442416
20. Nickel JC, Barkin J, Forrest J, et al; Elmiron Study Group. Randomized, double-blind, dose-ranging
study of pentosan polysulfate sodium for interstitial cystitis. Urology 2005 Apr;65(4):654-8.
http://www.ncbi.nlm.nih.gov/pubmed/15833501
21. van Ophoven A, Heinecke A, Hertle L. Safety and efficacy of concurrent application of oral pentosan
polysulfate and subcutaneous low-dose heparin for patients with interstitial cystitis. Urology 2005
Oct;66(4):707-11.
http://www.ncbi.nlm.nih.gov/pubmed/16230121
22. Warren JW, Horne LM, Hebel JR, et al. Pilot study of sequential oral antibiotics for the treatment of
interstitial cystitis. J Urol 2000 Jun;163(6):1685-8.
http://www.ncbi.nlm.nih.gov/pubmed/10799160
23. Oravisto KJ, Alfthan OS. Treatment of interstitial cystitis with immunosuppression and chloroquine
derivatives. Eur Urol 1976;2(2):82-4.
http://www.ncbi.nlm.nih.gov/pubmed/971677
24. Forsell T, Ruutu M, Isoniemi H, et al. Cyclosporine in severe interstitial cystitis. J Urol 1996
May;155(5):1591-3.
http://www.ncbi.nlm.nih.gov/pubmed/8627830
25. Moran PA, Dwyer PL, Carey MP, et al. Oral methotrexate in the management of refractory interstitial
cystitis. Aust N Z J Obstet Gynaecol 1999 Nov;39(4):468-71.
http://www.ncbi.nlm.nih.gov/pubmed/10687766
26. Sairanen J, Forsell T, Ruutu M. Long-term outcome of patients with interstitial cystitis treated with low
dose cyclosporine A. J Urol 2004 Jun;171(6 Pt 1):2138-41.
http://www.ncbi.nlm.nih.gov/pubmed/15126772
27. Sairanen J, Tammela TL, Leppilahti M, et al. Cyclosporine A and pentosan polysulfate sodium for the
treatment of interstitial cystitis: a randomized comparative study. J Urol 2005 Dec;174(6):2235-8.
http://www.ncbi.nlm.nih.gov/pubmed/16280777
28. Hansen HC. Interstitial cystitis and the potential role of gabapentin. South Med J 2000 Feb;93(2):
238-42.
http://www.ncbi.nlm.nih.gov/pubmed/10701800
29. Sasaki K, Smith CP, Chuang YC, et al. Oral gabapentin (neurontin) treatment of refractory
genitourinary tract pain. Tech Urol 2001 Mar;7(1):47-9.
http://www.ncbi.nlm.nih.gov/pubmed/11272678
30. Sonnett TE, Setter SM, Campbell RK. Pregabalin for the treatment of painful neuropathy. Expert
RevNeurother 2006 Nov;6(11):1629-35.
http://www.ncbi.nlm.nih.gov/pubmed/17144773
31. Ueda T, Tamaki M, Ogawa O, et al. Improvement of interstitial cystitis symptoms and problems that
developed during treatment with oral IPD-1151T. J Urol 2000 Dec;164(6):1917-20.
http://www.ncbi.nlm.nih.gov/pubmed/11061880
32. Katske F, Shoskes DA, Sender M, et al. Treatment of interstitial cystitis with a quercetin supplement.
Tech Urol 2001 Mar;7(1):44-6.
http://www.ncbi.nlm.nih.gov/pubmed/11272677

54 UPDATE FEBRUARY 2012
33. Theoharides TC, Sant GR. A pilot open label study of Cystoprotek in interstitial cystitis. Int J
Immunopathol Pharmacol 2005 Jan-Mar;18(1):183-8.
http://www.ncbi.nlm.nih.gov/pubmed/15698523
3.2.13 Intravesical treatment
Intravesical application of medications establishes high concentrations at the target, with few systemic side
effects. Disadvantages include the need for intermittent catheterisation, which can be painful in BPS patients,
cost, and risk of infection.
Local anaesthetics. There are sporadic reports of successful treatment of BPS with intravesical lidocaine (1,2).
Alkalisation of lidocaine before intravesical application improves pharmacokinetics (3). In an uncontrolled study,
significant immediate symptom relief was reported in 94% of patients and sustained relief after 2 weeks in
80%, using instillations of combined heparin and alkalinised lidocaine [40,000 U heparin, 2% lidocaine (160
mg), and 3 mL 8.4% sodium bicarbonate] (4). One hundred and two adult patients (99 women) with a clinical
diagnosis of BPS were randomised from 19 centres in the USA and Canada to receive a daily intravesical
instillation of alkalinised lidocaine or placebo (double-blind), for 5 consecutive days. Treated patients had
significant sustained symptom relief for up to 1 month (5).
Pentosan polysulphate sodium is a glycoprotein aimed at replenishing the GAG layer, which is applied
intravesically due to poor bioavailability following oral administration. A double-blind placebo-controlled study
(6) was performed in 20 patients, of whom 10 received intravesical pentosan polysulphate sodium (300 mg in
50 mL 0.9% saline) twice weekly for 3 months, and 10 received placebo.
At 3 months, four patients in the pentosan polysulphate sodium group and two in the placebo group achieved
significant symptomatic relief. Bladder capacity showed a significant increase only in patients treated with
pentosan polysulphate sodium. At 18 months, symptoms were relieved in eight patients, who were still
receiving pentosan polysulphate sodium instillation, and in four patients not receiving the drug. In another
study, a total of 41 women diagnosed with BPS were randomised to receive a combination of intravesical
plus oral pentosan polysulphate sodium (21 in treatment group) or intravesical placebo plus oral pentosan
polysulphate sodium (20 in placebo group) for 6 weeks. All subjects continued to receive oral pentosan
polysulphate sodium for a further 12 weeks. At week 18, the treatment group showed significant improvement
in all health-related QoL domains compared to baseline (P
_
0.01), whereas the placebo group showed
significant improvement in only three domains, (P
_
0.05) compared to baseline (7).
Intravesical heparin has been proposed as a coating agent. In an open, prospective, uncontrolled trial (8), 48
BPS patients received instillations of 10,000 U in 10 mL sterile water three times weekly for 3 months. In over
half of the patients, intravesical heparin controlled the symptoms, with continued improvement after 1 year of
therapy. Kuo et al. (9) have reported another uncontrolled trial of intravesical heparin (25,000 U twice weekly
for 3 months) in women with frequency-urgency syndrome and a positive potassium test. The study included
10 patients with BPS, of whom eight reported symptomatic improvement. Baykal et al. (10) have evaluated
intravesical heparin plus dorsal tibial nerve stimulation in 10 refractory BPS patients. Voiding frequency, pain
scores and maximum cystometric capacity were significantly better after 2 and 12 months compared to
pretreatment values.
Hyaluronic acid (hyaluronan) is a natural proteoglycan aimed at repairing defects in the GAG layer. A response
rate of 56% at week 4 and 71% at week 7 was reported in 25 patients treated with hyaluronic acid (11). After
week 24, effectiveness decreased, but there was no significant toxicity. Nordling et al. (12) and Kallestrup (13)
have reported a 3-year follow-up of a 3-month, prospective, non-randomised study evaluating the effect of
intravesical hyaluronic acid on BPS symptoms. Of the 20 patients, 11 chose to continue treatment beyond the
initial trial, and modest beneficial long-term effects were noted in about two-thirds of patients. Reduction in
urinary frequency was less effective and mostly due to an improvement in night-time voids.
Another study (14) has demonstrated a similar favourable effect of hyaluronic acid on pain reduction. Forty-
eight patients with typical symptoms and a positive potassium (0.4 M) sensitivity test were treated with weekly
instillations of 40 mg hyaluronic acid for 10 weeks. Visual analogue scale scores showed symptom relief due to
hyaluronic acid therapy, irrespective of bladder capacity. The improvement was particularly evident in patients
with a reduction in C
max
< 30% compared to patients with a reduction of < 30% with 0.2 M KCl solution (P =
0.003). Long-term effects were investigated in a study of 70 patients previously treated with hyaluronan. Of the
70 patients initially treated, 48 were available for evaluation. Of these, 50% reported complete remission with
no further therapy. Another 41.7% of patients with symptom recurrence improved after retreatment (15).

UPDATE FEBRUARY 2012 55
Chondroitin sulphate. Intravesical chondroitin sulphate (16) demonstrated beneficial effects in patients with a
positive potassium stimulation test, in two non-randomised, uncontrolled, open-label pilot studies. Steinhoff
(17) treated 18 patients with 40 mL instilled intravesically once weekly for 4 weeks and then once monthly
for 12 months. Thirteen of 18 patients were followed for the entire 13-month study. Twelve of these patients
responded to treatment within 3-12 weeks. A total of 6/13 (46.2%) showed a good response, 2/13 (15.4%)
had a fair response, 4/13 (30.8%) had a partial response, and 1/13 (7.7%) showed no response. In a second
trial (18), 24 refractory patients with BPS were treated with high-dose (2.0%) chondroitin sulphate instillations
twice weekly for 2 weeks, then weekly with 0.2% solution for 4 weeks, and monthly thereafter for 1 year. The
average symptom improvement reported in 20 patients completing the trial was 73.1% (range: 50-95%). The
time to optimum response was 4-6 months. A more concentrated 2.0% solution was needed in eight patients
to maintain results.
Sixty-five patients with BPS were treated in a prospective, randomised, double-blind, inactive vehicle-
controlled, 12-week study (6 weeks treatment, followed by 6 weeks follow-up). At the primary endpoint analysis
(week 7), 22.6% of the vehicle control group were responders compared with 39.4% of the active therapy
group, however, the difference was not significant, probably due to underpowering of the study (19,20).
Dimethyl sulphoxide (DMSO) is a chemical solvent and water-soluble liquid that penetrates cell membranes.
It is claimed to have analgesic, anti-inflammatory, collagenolytic, and muscle relaxant effects. It is also a
scavenger of the intracellular OH radical, which is believed to be an important trigger of the inflammatory
process. It has been tested empirically and found to alleviate symptoms in BPS. DMSO is now a standard
treatment. In a controlled crossover trial (21), 33 patients received instillations of 50% DMSO solution and
placebo (saline). All patients received both regimens, which were administered intravesically every 2 weeks for
two sessions of four treatments each. Subjective improvement was noted in 53% of patients receiving DMSO
versus 18% receiving placebo, and objective improvement in 93% and 35%, respectively.
Other uncontrolled trials with DMSO have reported response rates of 50-70% for a period of 1-2
months (22). Rossberger et al. (23) have evaluated the discomfort and long-term effects of DMSO instillations
in a total of 28 patients. Side effects were no more common or pronounced in patients with classic compared
to non-ulcer disease. After DMSO instillations, a residual treatment effect lasting 16-72 months could be seen.
DMSO is contraindicated during UTIs or shortly after bladder biopsy. It temporarily causes a garlic-like odour.
There is a case report in which DMSO treatment may have caused pigmented eye lens deposits (24), therefore,
ophthalmic review should be considered during treatment.
Bacillus Calmette Guérin (BCG). The tuberculosis BCG vaccine is used for its immunomodulatory properties
in the intravesical treatment of superficial bladder carcinoma. In 1997, a small prospective, double-blind pilot
study showed that intravesical BCG demonstrated a 60% response rate versus 27% in the placebo group in
30 patients who received six weekly instillations of Tice strain BCG or placebo (25). In a subsequent 24-33-
month follow-up study, eight of the nine responders reported BPS symptom amelioration. BCG did not
worsen symptoms in non-responders (26). However, these results are at variance with two controlled trials. In
a prospective, double-blind crossover trial of BCG and DMSO (86), BCG treatment failed to demonstrate any
benefit.
Another randomised, placebo-controlled, double-blind trial of 260 refractory BPS patients (27) reported global
response rates of 12% for placebo and 21% for BCG (P = 0.062). Small improvements were observed for all
secondary outcomes (voiding diary, pain, urgency, symptom indexes, and adverse events), some of which
were greater with BCG, but with only borderline statistical significance.
In a subsequent study (28), 156 non-responders from both groups were offered treatment with open-label
BCG. The low response rate (18%) for BCG in this series and the results of the same group’s (Interstitial
Cystitis Clinical Trials Group; ICCTG) follow-up on the responders, which found no differences, have
substantiated the argument against the routine use of BCG for BPS (29).
Vanilloids disrupt sensory neurons (30). Resiniferatoxin (RTX) is an ultrapotent analogue of the chilli pepper
extract capsaicin, causing less pain on instillation and therefore no anaesthesia. Chen et al. (31) have
investigated RTX tolerability (0.05 or 0.10 μM) in 22 BPS patients versus placebo. The most commonly reported
adverse event was pain during instillation (RTX > 80.0%, placebo 25.0%) but no serious adverse events were
reported. In a small RCT on 18 patients with hypersensitive bladder disorder and pain (32), RTX significantly
reduced mean frequency, nocturia, and pain scores by about 50%. In another study of seven patients with
detrusor hyper-reflexia, RTX improved urinary frequency, incontinence and bladder capacity (33). In a small
open-label study with single-dose RTX in patients with frequency and urgency (34), RTX significantly improved
LUTS, urodynamic parameters, and QoL for up to 6 months. These results are in contrast with an RCT in 163
BPS patients randomly assigned to receive a single intravesical dose of 50 mL of either placebo or RTX (0.01,
0.05 or 0.10 μM) (35). RTX resulted in a dose-dependent increase in instillation pain, but otherwise was well

56 UPDATE FEBRUARY 2012
tolerated. It did not improve overall symptoms, pain, urgency, frequency, nocturia, or average void volume
during 12 weeks follow-up.
More favourable results have been reported from a prospective study on multiple intravesical
instillations of RTX (36) (0.01 μM once weekly for 4 weeks). Among 12 patients (one drop-out for severe pain),
the overall satisfaction rate was 58.3%, with several scales of symptom and QoL significantly improved after
RTX treatment. There was no significant increase in functional bladder capacity or change in urodynamic
parameters. A prospective, randomised, double-blind, crossover study was performed in 26 women, who
received instillations with various pH values. There was no evidence that changes in urinary pH affected the
pain associated with BPS (37).
3.2.13.1 References
1. Giannakopoulos X, Champilomatos P. Chronic interstitial cystitis. Successful treatment with
intravesical lidocaine. Arch Ital Urol Nefrol Androl 1992 Dec;64(4):337-9.
http://www.ncbi.nlm.nih.gov/pubmed/1462157
2. Asklin B, Cassuto J. Intravesical lidocaine in severe interstitial cystitis. Case report. Scand J Urol
Nephrol 1989;23(4):311-2.
http://www.ncbi.nlm.nih.gov/pubmed/2595329
3. Henry R, Patterson L, Avery N, et al. Absorption of alkalized intravesical lidocaine in normal and
inflamed bladders: a simple method for improving bladder anaesthesia. J Urol 2001 Jun;165(6 Pt
1):1900-3.
http://www.ncbi.nlm.nih.gov/pubmed/11371877
4. Parsons CL. Successful downregulation of bladder sensory nerves with combination of heparin and
alkalinized lidocaine in patients with interstitial cystitis. Urology 2005 Jan;65(1):45-8.
http://www.ncbi.nlm.nih.gov/pubmed/15667861
5. Nickel JC, Moldwin R, Lee S, et al. Intravesical alkalinized lidocaine (PSD597) offers sustained relief
from symptoms of interstitial cystitis and painful bladder syndrome. BJU Int. 2009 Apr;103(7):910-8.
http://www.ncbi.nlm.nih.gov/pubmed/19021619
6. Bade JJ, Laseur M, Nieuwenburg A, et al. A placebo-controlled study of intravesical
pentosanpolysulphate for the treatment of interstitial cystitis. Br J Urol 1997 Feb;79(2):168-71.
http://www.ncbi.nlm.nih.gov/pubmed/9052464
7. Davis EL, El Khoudary SR, Talbott EO, et al. Safety and efficacy of the use of intravesical and oral
pentosan polysulfate sodium for interstitial cystitis: a randomized double-blind clinical trial.J Urol.
2008 Jan;179(1):177-85.
http://www.ncbi.nlm.nih.gov/pubmed/18001798
8. Parsons CL, Housley T, Schmidt JD, et al. Treatment of interstitial cystitis with intravesical heparin.
BrJ Urol 1994 May;73(5):504-7.
http://www.ncbi.nlm.nih.gov/pubmed/8012771
9. Kuo HC. Urodynamic results of intravesical heparin therapy for women with frequency urgency
syndrome and interstitial cystitis. J Formos Med Assoc 2001 May;100(5):309-14.
http://www.ncbi.nlm.nih.gov/pubmed/11432309
10. Baykal K, Senkul T, Sen B, et al. Intravesical heparin and peripheral neuromodulation on interstitial
cystitis. Urol Int 2005;74(4):361-4.
http://www.ncbi.nlm.nih.gov/pubmed/15897705
11. Morales A, Emerson L, Nickel JC, et al. Intravesical hyaluronic acid in the treatment of refractory
interstitial cystitis. Urology. 1997 May;49(5A Suppl):111-3.
http://www.ncbi.nlm.nih.gov/pubmed/9146012
12. Nordling J, Jørgensen S, Kallestrup E. Cystistat for the treatment of interstitial cystitis: a 3-year
followup study. Urology 2001 Jun;57(6 Suppl 1):123.
http://www.ncbi.nlm.nih.gov/pubmed/11378112
13. Kallestrup EB, Jørgensen S, Nordling J, et al. Treatment of interstitial cystitis with Cystistat: a
hyaluronic acid product. Scand J Urol Nephrol 2005;39(2):143-7.
http://www.ncbi.nlm.nih.gov/pubmed/16032779
14. Daha LK, Riedl CR, Lazar D, et al. Do cystometric findings predict the results of intravesical hyaluronic
acid in women with interstitial cystitis? Eur Urol 2005 Mar;47(3):393-7; discussion 397.
http://www.ncbi.nlm.nih.gov/pubmed/15716206
15. Engelhardt PF, Morakis N, Daha LK, et al. Long-term results of intravesical hyaluronan therapy in
bladder pain syndrome/interstitial cystitis. Int Urogynecol J Pelvic Floor Dysfunct. 2011 Apr;22(4):
401-5.
http://www.ncbi.nlm.nih.gov/pubmed/20938644

UPDATE FEBRUARY 2012 57
16. Palylyk-Colwell E. Chondroitin sulfate for interstitial cystitis. Issues Emerg Health Technol 2006
May(84);1-4.
http://www.ncbi.nlm.nih.gov/pubmed/16724430
17. Steinhoff G. The efficacy of chondroitin sulfate in treating interstitial cystitis. Can J Urol. 2002
Feb;9(1):1454-8.
http://www.ncbi.nlm.nih.gov/pubmed/11886599
18. Sorensen RB. Chondroitin sulphate in the treatment of interstitial cystitis and chronic inflammatory
disease of the urinary bladder. Eur Urol 2003;Suppl 2:16-8.
19. Nickel JC, Egerdie B, Downey J, et al. A real-life multicentre clinical practice study to evaluate the
efficacy and safety of intravesical chondroitin sulphate for the treatment of interstitial cystitis. BJU Int.
2009 Jan;103(1):56-60.
http://www.ncbi.nlm.nih.gov/pubmed/18778342
20. Nickel JC, Egerdie RB, Steinhoff G, et al. A multicenter, randomized, double-blind, parallel group pilot
evaluation of the efficacy and safety of intravesical sodium chondroitin sulfate versus vehicle control in
patients with interstitial cystitis/painful bladder syndrome. Urology. 2010 Oct;76(4):804-9.
http://www.ncbi.nlm.nih.gov/pubmed/20494413
21. Perez-Marrero R, Emerson LE, Feltis JT. A controlled study of dimethyl sulfoxide in interstitial cystitis.
J Urol 1988 Jul;140(1):36-9.
http://www.ncbi.nlm.nih.gov/pubmed/3288775
22. Sant GR, LaRock DR. Standard intravesical therapies for interstitial cystitis. Urol Clin North Am 1994
Feb;21(1):73-83.
http://www.ncbi.nlm.nih.gov/pubmed/8284849
23. Rössberger J, Fall M, Peeker R. Critical appraisal of dimethyl sulfoxide treatment for interstitial
cystitis:discomfort, side-effects and treatment outcome. Scand J Urol Nephrol 2005;39(1):73-7.
http://www.ncbi.nlm.nih.gov/pubmed/15764276
24. Rowley S, Baer R. Lens deposits associated with RIMSO-50 (dimethylsulphoxide). Eye 2001 Jun;15(Pt
3):332-3.
http://www.ncbi.nlm.nih.gov/pubmed/11450733
25. Peters K, Diokno A, Steinert B, et al. The efficacy Of intravesical Tice strain bacillus Calmette-Guerin
in the treatment of interstitial cystitis: a double-blind, prospective, placebo controlled trial. J Urol 1997
Jun;157(6):2090-4.
http://www.ncbi.nlm.nih.gov/pubmed/9146587
26. Peters KM, Diokno AC, Steinert BW, et al. The efficacy of intravesical bacillus Calmette-Guerin in the
treatment of interstitial cystitis: long-term followup. J Urol 1998 May;159(5):1483-6; discussion1486-7.
http://www.ncbi.nlm.nih.gov/pubmed/9554338
27. Mayer R, Propert KJ, Peters KM, et al. Interstitial Cystitis Clinical Trials Group. A randomized
controlled trial of intravesical bacillus calmette-guerin for treatment refractory interstitial cystitis. J Urol
2005 Apr;173(4):1186-91.
http://www.ncbi.nlm.nih.gov/pubmed/15758738
28. Propert KJ, Mayer R, Nickel JC, et al. Interstitial Cystitis Clinical Trials Group. Did patients with
interstitial cystitis who failed to respond to initial treatment with bacillus Calmette-Guerin or placebo in
a randomized clinical trial benefit from a second course of open label bacillus Calmette-Guerin? J Urol
2007 Sep;178(3 Pt 1):886-90.
http://www.ncbi.nlm.nih.gov/pubmed/17631335
29. Propert KJ, Mayer R, Nickel JC, et al. Interstitial Cystitis Clinical Trials Group. Followup of patients
with interstitial cystitis responsive to treatment with intravesical bacillus Calmette-Guerin or placebo.
J Urol. 2008 Feb;179(2):552-5.
http://www.ncbi.nlm.nih.gov/pubmed/18082224
30. Chancellor MB. RTX exotoxins. Urology 2001 Jun;57(6 Suppl 1):106-7.
http://www.ncbi.nlm.nih.gov/pubmed/11378069
31. Chen TY, Corcos J, Camel M, et al. Prospective, randomized, double-blind study of safety and
tolerability of intravesical resiniferatoxin (RTX) in interstitial cystitis (IC). Int Urogynecol J Pelvic Floor
Dysfunct 2005 Jul-Aug;16(4):293-7.
http://www.ncbi.nlm.nih.gov/pubmed/15818465
32. Lazzeri M, Beneforti P, Spinelli M, et al. Intravesical resiniferatoxin for the treatment of hypersensitive
disorder: a randomized placebo controlled study. J Urol 2000 Sep;164(3 Pt 1):676-9.
http://www.ncbi.nlm.nih.gov/pubmed/10953124
33. Silva C, Avelino A, Souto-Moura C, et al. A light- and electron-microscopic histopathological study of
human bladder mucosa after intravesical resiniferatoxin application. BJU Int 2001 Sep;88(4):355-60.
http://www.ncbi.nlm.nih.gov/pubmed/11564021

58 UPDATE FEBRUARY 2012
34. Apostolidis A, Gonzales GE, Fowler CJ. Effect of intravesical Resiniferatoxin (RTX) on lower urinary
tract symptoms, urodynamic parameters, and quality of life of patients with urodynamic increased
bladder sensation. Eur Urol 2006 Dec;50(6):1299-305.
http://www.ncbi.nlm.nih.gov/pubmed/16697519
35. Payne CK, Mosbaugh PG, Forrest JB, et al. ICOS RTX Study Group (Resiniferatoxin Treatment for
Interstitial Cystitis). Intravesical resiniferatoxin for the treatment of interstitial cystitis: a randomized,
double-blind, placebo controlled trial. J Urol 2005 May;173(5):1590-4.
http://www.ncbi.nlm.nih.gov/pubmed/15821499
36. Peng CH, Kuo HC. Multiple intravesical instillations of low-dose resiniferatoxin in the treatment of
refractory interstitial cystitis. Urol Int 2007;78(1):78-81.
http://www.ncbi.nlm.nih.gov/pubmed/17192738
37. Nguan C, Franciosi LG, Butterfield NN, et al. A prospective, double-blind, randomized cross-over
study evaluating changes in urinary pH for relieving the symptoms of interstitial cystitis. BJU Int 2005
Jan;95(1):91-4.
http://www.ncbi.nlm.nih.gov/pubmed/15638902
3.2.14 Interventional treatments
Bladder distension. A frequently cited report by Bumpus et al. (1) claims that hydrodistension achieved
symptom improvement in 100 patients over several months. However, the study did not define either patient
population or symptoms and the methods used were inadequately described. Reports by Ormond (2) and
Longacre (3) were just as vague during the 1930s. In 1957, an uncontrolled retrospective study was presented
by Franksson (4), who treated 33 patients with repeated, up to 10-fold, distensions. Twelve patients had
improved symptoms for up to 4 weeks, in 14 patients for up to 6 months, and in seven patients for up to 1
year. British studies from the 1970s have reported contradictory results. Dunn et al. (5) have claimed to have
achieved complete absence of symptoms in 16/25 patients during a mean follow-up of 14 months using the
Helmstein method (6), in which an intravesical balloon is distended at the level of systolic blood pressure for
3 h. Bladder rupture occurred in two cases. These results disagree with those of Badenoch (7), who failed to
note any improvement in 44/56 patients after hydrodistension. Twenty years later, McCahy (8) rejected balloon
hydrodistension because of inefficacy and a complication rate of 20%. In the recent literature, bladder necrosis
following hydrodistension has been extremely rare (9).
In 2002, Glemain et al. (10) reported an uncontrolled study on 65 BPS patients treated by 3 h balloon
hydrodistension. Treatment efficacy in the 33 retrospectively and 32 prospectively studied patients was 38%
and 60% at 6 months, and 22% and 43% at 1 year, respectively. Results were superior for bladder capacities
> 150 mL.
Ottem and Teichmann (2006) reported a retrospective study of 84 BPS patients (11), and 56%
reported short-lived improvement from hydrodistension. Rose et al. have investigated bladder distension using
electromotive drug administration (EMDA) (12,13), as an alternative to general anaesthesia. Among 11 patients,
the distension capacity achieved by EMDA was nearly identical to that in the operating room and cystoscopic
findings were similar. Yamada et al. (14) have reported on repeated hydrodistension in 52 BPS patients (NIH
criteria). Under epidural anaesthesia, the bladder was repeatedly distended to maximal capacity and distension
was repeated on the following day for 30 min. Five patients were classified as good responders, 30 as
moderate and 17 as poor. Overall, hydrodistension was effective for ~70% of patients for > 3 months, without
serious complications.
According to a study by Erickson et al. (15), the median symptom score for newly diagnosed
patients decreased after distension, but only a few patients had at least 30% symptom improvement. Bladder
distension altered levels of urine antiproliferative factor and heparin-binding epidermal-growth-factor-like
growth factor towards normal. However, the mechanism of symptom relief after distension remains unknown.
In a retrospective review of 185 patients who underwent hydrodistension (16), results failed to identify
any statistically significant differences in objective findings (anaesthetic capacity, glomerulations) following
distension, or any therapeutic benefits, when patients were categorised according to presenting symptoms.
Although bladder hydrodistension is a common treatment for BPS, scientific justification is scarce. It
represents a diagnostic tool, but has a limited therapeutic role.
EMDA enhances tissue penetration of ionised drugs by iontophoresis. When adapted for the bladder, EMDA
uses a transurethral anode and a suprapubic skin cathode. EMDA is expensive and has been the subject of
uncontrolled studies only.
Six BPS patients were treated with EMDA using lidocaine (1.5%) and 1:100,000 adrenaline in aqueous
solution, while the bladder was dilated to maximum tolerance (17). Significant bladder enlargement was
achieved and voiding symptoms and pain decreased. In four patients, the results were reported as durable.

UPDATE FEBRUARY 2012 59
Rosamilia et al. (18) treated 21 women using EMDA with lidocaine and dexamethasone, followed by bladder
distension. A good response was seen in 85% of patients at 2 weeks, with 63% still responding at 2 months.
Complete resolution of pain was achieved in 25% of patients reviewed at 6 months. Using a similar technique,
Riedl et al. (19) noted complete resolution of bladder symptoms in 8/13 patients lasting 1-17 months. Partial or
short-term improvement was observed in three patients. Two patients experienced aggravated pain for several
days after therapy. A 66% increase in bladder capacity was observed. Upon symptom recurrence, treatments
were repeated with equal efficacy in 11 patients.
Transurethral resection (TUR) coagulation and laser. Endourological ablation of bladder tissue aims to eliminate
urothelial, mostly Hunner, lesions. In a case report, Kerr (20) has described TUR of a 1-cm ulcer in a woman
who experienced symptom resolution for 1 year. Subsequently, Greenberg et al. (21) have reported 77
patients with Hunner ulcers treated over a 40-year period: 42 were managed conservatively, seven underwent
fulguration, and 28 were treated by TUR in a non-randomised fashion. Fulguration improved symptoms in
5/7 patients. All patients experienced symptom recurrence in < 1 year and efficacy was not superior to non-
surgical treatment.
In another series of 30 BPS type C patients (22), complete TUR of visible lesions resulted in an initial
disappearance of pain in all patients and a decrease in frequency in 21. Relapse was noted in one-third of
patients after 2-20 months, while the remaining two-thirds were still pain-free after 2-42 months. The same
group recently has reported the largest series of patients with BPS type C treated by complete TUR of all
visible ulcers (23). A total of 259 TURs were performed on 103 patients. Ninety-two patients experienced
amelioration, with symptom relief lasting > 3 years in 40% of patients, and most of the remaining patients
responded well to subsequent TUR.
Transurethral application of the (Nd-YAG) laser is suggested as an alternative to TUR for endoscopic
treatment in BPS. Shanberg et al. (24) have treated five refractory BPS patients, four of whom demonstrated
cessation of pain and frequency within several days. Follow-up at 3-15 months revealed no relapse, except
for mild recurrent voiding symptoms. This series was extended to 76 patients treated at two institutions (25).
Although 21 of 27 patients with Hunner ulcers noted symptom improvement, 12 experienced relapse within
18 months. In the group without ulcers, only 20 of 49 patients improved, of whom 10 required further therapy
within 1 year.
In a later study, 24 patients with refractory BPS type C underwent ablative Nd-YAG laser ablation of
Hunner’s ulcers (26). All patients showed symptom improvement within a few days, without complications.
At 23 months, mean pain and urgency scores, nocturia and voiding intervals improved significantly.
However, relapse in 11 patients required up to four additional treatments. Controlled studies are still lacking.
Endourological resection is not applicable to non-ulcer BPS.
Botulinum toxin A (BTX-A) may have an antinociceptive effect on bladder afferent pathways, producing both
symptomatic and urodynamic improvements (27). Thirteen BPS patients were injected with 100-200 IU of
BTX-A (abobotulinumtoxin A or onabotulinumtoxin A) into 20-30 sites submucosally in the trigone and floor of
the bladder. Overall, nine (69%) patients noted subjective improvement, and ICSI scores improved by 70%
(P < 0.05). There were significant decreases in daytime frequency, nocturia and pain, and a significant increase
in first desire to void and maximal cystometric capacity. However, these results are in contrast with those in
another study of BTX-A (onabotulinumtoxin A) in 10 patients with BPS (28). One hundred units were injected
suburothelially into 20 sites in five patients, while 100 U were injected into the trigone in the remaining five.
None of the patients became symptom-free; two showed only limited improvement in bladder capacity and
pain score.
To ascertain effect of repeat injections a total of 13 patients were followed up for 2 years, while 58 injections
were administered with a mean of 4.8 ± 0.8 injections per patient. The mean interval between two consecutive
injections was 5.25 ± 0.75 months. At 1 and 4 months follow-up, 10 patients reported a subjective
improvement. Mean VAS scores, mean daytime and night-time urinary frequency decreased significantly. The
three non-responders to the first intravesical treatment session underwent further treatment 3 months later with
satisfactory results. At 1 and 2 years follow-up, the beneficial effects persisted in all patients (29).
In an RCT, the difference between hydrodistension and hydrodistension plus intravesical BTX-A
(onabotulinumtoxin A) was analysed. Of the 67 patients, 44 were divided in two groups: one received 200
U and the other 100 U, and cystoscopic hydrodistension was performed after 2 weeks. The remaining 23
patients received hydrodistension only. There was symptomatic improvement in all groups. However, in the
hydrodistension group, 70% had returned to their previous symptoms after the first month, while in the BTX-A-
treated groups, there was improvement of VAS, functional bladder capacity and cystometric bladder capacity
at 3 months. At 12 and 24 months, the results in the active group were 55 and 30% versus 26 and 17% in the
hydrodistension group (30).

60 UPDATE FEBRUARY 2012
Trigonal-only injection seems effective and long-lasting because 87% of patients (n = 23) reported
improvement after a 3-month follow-up period in a study by Pinto et al. Over 50% referred continuity of
the beneficial effect 9 months after the first treatment. When retreatment was needed, similar results were
obtained. The authors concluded that this treatment is safe, effective and can be repeated (31).
Hyperbaric oxygen (HBO). In a prospective pilot study, six patients underwent 30 sessions of 100% HBO
inhalation and were followed up for > 15 months. Four patients rated the therapeutic result as excellent or
good, while two showed only short-term amelioration (32). In a subsequent double-blind, sham-controlled
study (33), 3/14 patients on HBO and no control patients were identified as responders (P < 0.05). At 12
months, three patients (21.4%) still reported a treatment response. Hyperbaric oxygenation resulted in a
decrease of baseline urgency and pain (P < 0.05). ICSI scores decreased from 26 to 20 points in patients on
HBO, while sham treatment did not result in any improvement. These results suggest that HBO is a safe and
feasible therapeutic approach, with moderate effects on a small subgroup of BPS patients.
Disadvantages include high costs, limited availability of treatment sites and time-consuming treatment.
Neuromodulation. In the first prospective, single-blind, crossover trial of sacral nerve stimulation (SNS) versus
pudendal nerve stimulation (PNS) for patients with BPS (n = 22), PNS gave an overall 59% improvement in
symptoms, whereas SNS gave an overall 44% improvement (P = 0.05). Most patients who tested both a sacral
and pudendal electrode chose PNS as the better site. Follow-up showed marked improvements in voiding
variables and validated BPS symptom questionnaires. Over 90% of patients treated with neuromodulation
stated that they would undergo implantation again (34).
Long-term results were verified in a retrospective study of 78 patients treated from 1994 to 2008.
Permanent sacral neuromodulation implantation was performed in patients who showed at least 50%
improvement in their symptoms with a temporary peripheral nerve evaluation test. Median follow-up was 61.5
(SD± 27.7 months). Good long-term success of sacral neuromodulation was seen in 72% of the patients. The
explantation rate was 28%. The most frequent reason for explantation was poor outcome (54% of the failed
patients). The revision rate was 50% (35).
In another observational, retrospective, case-controlled review (January 2002-March 2004), 34 female
patients underwent permanent device implants. Mean pre-/postoperative pelvic pain and urgency/frequency
scores were 21.61 ± 8.6/9.22 ± 6.6 (P < 0.01), and mean pre-/postoperative visual analogue pain scale (VAPS)
scores were 6.5 ± 2.9/2.4 ± 1.1 (P < 0.01). Mean follow-up was 86 ± 9.8 months. Sacral neuromodulation
showed adequate improvement for the symptoms of refractory BPS. Reoperation rate was 25% (36).
3.2.14.1 References
1. Bumpus HCJ. Interstitial cystitis: its treatment by overdistension of the bladder. Med Clin North Am
1930;13:1495-8.
2. Ormond JK. Interstitial cystitis. J Urol 1935;33:576-82.
3. Longacre JJ. The treatment of contracted bladder with controlled tidal irrigation. J Urol 1936;36:25-33.
4. Franksson C. Interstitial cystitis: a clinical study of fifty-nine cases. Acta Chir Scand 1957
May;113(1):51-62.
http://www.ncbi.nlm.nih.gov/pubmed/13443727
5. Dunn M, Ramsden PD, Roberts JB, et al. Interstitial cystitis, treated by prolonged bladder distension.
Br J Urol 1977;49(7):641-5.
http://www.ncbi.nlm.nih.gov/pubmed/597701
6. Helmstein K. Treatment of bladder carcinoma by a hydrostatic pressure technique. Report on 43
cases. Br J Urol 1972 Aug;44(4):434-50.
http://www.ncbi.nlm.nih.gov/pubmed/5070147
7. Badenoch AW. Chronic interstitial cystitis. Br J Urol 1971 Dec;43(6):718-21.
http://www.ncbi.nlm.nih.gov/pubmed/5159574
8. McCahy PJ, Styles RA. Prolonged bladder distension: experience in the treatment of detrusor
overactivity and interstitial cystitis. Eur Urol 1995;28(4):325-7.
http://www.ncbi.nlm.nih.gov/pubmed/8575501
9. Zabihi N, Allee T, Maher MG, et al. Bladder necrosis following hydrodistention in patients with
interstitial cystitis. J Urol 2007 Jan;177(1):149-52; discussion 152.
http://www.ncbi.nlm.nih.gov/pubmed/17162025
10. Glemain P, Rivière C, Lenormand L, et al. Prolonged hydrodistention of the bladder for symptomatic
treatment of interstitial cystitis: efficacy at 6 months and 1 year. Eur Urol 2002 Jan;41(1):79-84.
http://www.ncbi.nlm.nih.gov/pubmed/11999471

UPDATE FEBRUARY 2012 61
11. Ottem DP, Teichman JM. What is the value of cystoscopy with hydrodistension for interstitial cystitis?
Urology 2005 Sep;66(3):494-9.
http://www.ncbi.nlm.nih.gov/pubmed/16140064
12. Rose AE, Azevedo KJ, Payne CK. Office bladder distention with electromotive drug administration
(EMDA) is equivalent to distention under general anesthesia (GA). BMC Urol 2005 Nov;5:14.
http://www.ncbi.nlm.nih.gov/pubmed/16300684
13. Rose AE, Payne CK, Azevedo K. Pilot study of the feasibility of in-office bladder distention using
electromotive drug adminstration (EMDA). Neurourol Urodyn 2005;24(3):254-60.
http://www.ncbi.nlm.nih.gov/pubmed/15747341
14. Yamada T, Murayama T, Andoh M. Adjuvant hydrodistension under epidural anesthesia for interstitial
cystitis. Int J Urol 2003 Sep;10(9):463-8; discussion 469.
http://www.ncbi.nlm.nih.gov/pubmed/12941123
15. Erickson DR, Kunselman AR, Bentley CM, et al. Changes in urine markers and symptoms after bladder
distention for interstitial cystitis. J Urol 2007 Feb;177(2):556-60.
http://www.ncbi.nlm.nih.gov/pubmed/17222633
16. Cole EE, Scarpero HM, Dmochowski RR. Are patient symptoms predictive of the diagnostic and/or
therapeutic value of hydrodistention? Neurourol Urodyn 2005;24(7):638-42.
http://www.ncbi.nlm.nih.gov/pubmed/16208660
17. Gürpinar T, Wong HY, Griffith DP. Electromotive administration of intravesical lidocaine in patients
with interstitial cystitis. J Endourol 1996 Oct;10(5):443-7.
http://www.ncbi.nlm.nih.gov/pubmed/8905491
18. Rosamilia A, Dwyer PL, Gibson J. Electromotive drug administration of lidocaine and dexamethasone
followed by cystodistension in women with interstitial cystitis. Int Urogynecol J Pelvic Floor Dysfunct
1997;8(3):142-5.
http://www.ncbi.nlm.nih.gov/pubmed/9449586
19. Riedl CR, Knoll M, Plas E, et al. Electromotive drug administration and hydrodistention for the
treatment of interstitial cystitis. J Endourol 1998 Jun;12(3):269-72.
http://www.ncbi.nlm.nih.gov/pubmed/9658301
20. Kerr WS Jr. Interstitial cystitis: treatment by transurethral resection. J Urol 1971 ay;105(5):664-6.
http://www.ncbi.nlm.nih.gov/pubmed/4397018
21. Fall M. Conservative management of chronic interstitial cystitis: transcutaneous electrical nerve
stimulation and transurethral resection. J Urol 1985 May;133(5):774-8.
http://www.ncbi.nlm.nih.gov/pubmed/3872946
22. Peeker R, Aldenborg F, Fall M. Complete transurethral resection of ulcers in classic interstitial cystitis.
Int Urogynecol J Pelvic Floor Dysfunct 2000;11(5):290-5.
http://www.ncbi.nlm.nih.gov/pubmed/11052564
23. Greenberg E, Barnes R, Stewart S, et al. Transurethral resection of Hunner’s ulcer. J Urol 1974
Jun;111(6):764-6.
http://www.ncbi.nlm.nih.gov/pubmed/4830879
24. Shanberg AM, Baghdassarian R, Tansey LA. Treatment of interstitial cystitis with the neodymium-YAG
laser. J Urol 1985 Nov;134(5):885-8.
http://www.ncbi.nlm.nih.gov/pubmed/3840538
25. Malloy TR, Shanberg AM. Laser therapy for interstitial cystitis. Urol Clin North Am 1994 Feb; 21(1):
141-4.
http://www.ncbi.nlm.nih.gov/pubmed/8284837
26. Rofeim O, Hom D, Freid RM, et al. Use of the neodymium: yag laser for interstitial cystitis: a
prospective study. J Urol 2001 Jul;166(1):134-6.
http://www.ncbi.nlm.nih.gov/pubmed/11435840
27. Smith CP, Radziszewski P, Borkowski A, et al. Botulinum toxin a has antinociceptive effects in treating
interstitial cystitis. Urology 2004 Nov;64(5):871-5; discussion 875.
http://www.ncbi.nlm.nih.gov/pubmed/15533466
28. Kuo HC. Preliminary results of suburothelial injection of botulinum a toxin in the treatment of chronic
interstitial cystitis. Urol Int 2005;75(2):170-4.
http://www.ncbi.nlm.nih.gov/pubmed/16123573
29. Giannantoni A, Mearini E, Del Zingaro M, et al.Two-year efficacy and safety of botulinum a toxin
intravesical injections in patients affected by refractory painful bladder syndrome. Curr Drug Deliv.
2010 Jan;7(1):1-4.
http://www.ncbi.nlm.nih.gov/pubmed/19863481

62 UPDATE FEBRUARY 2012
30. Kuo HC, Chancellor MB. Comparison of intravesical botulinum toxin type A injections plus
hydrodistention with hydrodistention alone for the treatment of refractory interstitial cystitis/painful
bladder syndrome.BJU Int. 2009 Sep;104(5):657-61.
http://www.ncbi.nlm.nih.gov/pubmed/19338543
31. Pinto R, Lopes T, Frias B, et al. Trigonal injection of botulinum toxin A in patients with refractory
bladder pain syndrome/interstitial cystitis. Eur Urol. 2010 Sep;58(3):360-5.
http://www.ncbi.nlm.nih.gov/pubmed/20227820
32. van Ophoven A, Rossbach G, Oberpenning F, et al. Hyperbaric oxygen for the treatment of interstitial
cystitis: long-term results of a prospective pilot study. Eur Urol 2004 Jul;46(1):108-13.
http://www.ncbi.nlm.nih.gov/pubmed/15183555
33. van Ophoven A, Rossbach G, Pajonk F, et al. Safety and efficacy of hyperbaric oxygen therapy for
the treatment of interstitial cystitis: a randomized, sham controlled, double-blind trial. J Urol 2006
Oct;176(4 Pt 1):1442-6.
http://www.ncbi.nlm.nih.gov/pubmed/16952654
34. Peters KM, Feber KM, Bennett RC. A prospective, single-blind, randomized crossover trial of sacral vs
pudendal nerve stimulation for interstitial cystitis. BJU Int. 2007 Oct;100(4):835-9.
http://www.ncbi.nlm.nih.gov/pubmed/17822464
35. Gajewski JB, Al-Zahrani AA. The long-term efficacy of sacral neuromodulation in the management
of intractable cases of bladder pain syndrome: 14 years of experience in one centre. BJU Int. 2011
Apr;107(8):1258-64.
http://www.ncbi.nlm.nih.gov/pubmed/20883483
36. Marinkovic SP, Gillen LM, Marinkovic CM. Minimum 6-year outcomes for interstitial cystitis treated
with sacral neuromodulation. Int Urogynecol J Pelvic Floor Dysfunct. 2011 Apr;22(4):407-12.
http://www.ncbi.nlm.nih.gov/pubmed/20848271
3.2.15 Treatments of limited efficacy and absence of recent publications
Cimetidine. The H2-blocker cimetidine has been reported to improve symptoms in BPS (1). Thirty-six patients
were enrolled in a double-blind clinical study with oral cimetidine versus placebo for 3 months. Patients
receiving cimetidine showed a significant improvement in symptom scores, pain and nocturia, although
histologically, the bladder mucosa showed no qualitative changes in either group (2).
Prostaglandins. Misoprostol is a prostaglandin that regulates various immunological cascades. Twenty-five
BPS patients received 600 μg/day misoprostol for 3 months, with responders treated for a further 6 months.
At 3 months, 14 had significantly improved, with 12 showing a sustained response after a further 6 months.
However, the incidence of adverse drug effects was 64% (3).
L-Arginine. Oral treatment with l-arginine, the substrate for NO synthase, has been reported to decrease BPS-
related symptoms (4-6). NO has been shown to be elevated in patients with BPS (7). However, others could not
demonstrate either symptomatic relief or change in NO production after treatment (8,9).
Anticholinergics. Oxybutynin is an anticholinergic drug used in overactive detrusor dysfunction. Intravesically
administered oxybutynin was combined with bladder training in one study, with improvement of functional
bladder capacity, volume at first sensation and cystometric bladder capacity (10). However, the effect on pain
was not reported.
Duloxetine inhibits both serotonin and noradrenaline reuptake. In an observational study, 48 women were
prospectively treated with duloxetine for 2 months following an up-titration protocol to the target dose of 2
40 mg/day duloxetine over 8 weeks (11). Duloxetine did not result in significant improvement of symptoms.
Administration was safe, but tolerability was poor due to nausea. Based on these preliminary data, duloxetine
cannot be recommended as a therapeutic approach for BPS.
Clorpactin is a detergent of hypochloric acid previously used to treat BPS (12-16). Due to high complication
rates (14-17), clorpactin instillations can no longer be recommended.
3.2.15.1 References
1. Dasgupta P, Sharma SD, Womack C, et al. Cimetidine in painful bladder syndrome: a
histopathological study. BJU Int 2001 Aug;88(3):183-6.
http://www.ncbi.nlm.nih.gov/pubmed/11488726

UPDATE FEBRUARY 2012 63
2. Thilagarajah R, Witherow RO, Walker MM. Oral cimetidine gives effective symptom relief in painful
bladder disease: a prospective, randomized, double-blind placebo-controlled trial. BJU Int 2001
Feb;87(3):207-12.
http://www.ncbi.nlm.nih.gov/pubmed/11167643
3. Kelly JD, Young MR, Johnston SR, et al. Clinical response to an oral prostaglandin analogue in
patients with interstitial cystitis. Eur Urol 1998;34(1):53-6.
http://www.ncbi.nlm.nih.gov/pubmed/9676414
4. Korting GE, Smith SD, Wheeler MA, et al. A randomized double-blind trial of oral Larginine for
treatment of interstitial cystitis. J Urol 1999 Feb;161(2):558-65.
http://www.ncbi.nlm.nih.gov/pubmed/9915448
5. Wheeler MA, Smith SD, Saito N, et al. Effect of long-term oral L-arginine on the nitric oxide synthase
pathway in the urine from patients with interstitial cystitis. J Urol 1997 Dec; 158(6):2045-50.
http://www.ncbi.nlm.nih.gov/pubmed/9366309
6. Smith SD, Wheeler MA, Foster HE Jr, et al. Improvement in interstitial cystitis symptom scores during
treatment with oral L-arginine. J Urol 1997 Sep;158(3 Pt 1):703-8.
http://www.ncbi.nlm.nih.gov/pubmed/9258064
7. Lundberg JO, Ehren I, Jansson O, et al. Elevated nitric oxide in the urinary bladder in infectious and
noninfectious cystitis. Urology 1996 Nov;48(5):700-2.
http://www.ncbi.nlm.nih.gov/pubmed/8911512
8. Ehren I, Lundberg JO, Adolfsson J, et al. Effects of L-arginine treatment on symptoms and bladder
nitric oxide levels in patients with interstitial cystitis. Urology 1998 Dec;52(6):1026-9.
http://www.ncbi.nlm.nih.gov/pubmed/9836549
9. Cartledge JJ, Davies AM, Eardley I. A randomized double-blind placebo-controlled crossover trial of
the efficacy of L-arginine in the treatment of interstitial cystitis. BJU Int 2000 Mar;85(4):421-6.
http://www.ncbi.nlm.nih.gov/pubmed/10691818
10. Barbalias GA, Liatsikos EN, Athanasopoulos A, et al. Interstitial cystitis: bladder training with
intravesical oxybutynin. J Urol 2000 Jun;163(6):1818-22.
http://www.ncbi.nlm.nih.gov/pubmed/10799190
11. van Ophoven A, Hertle L. The dual serotonin and noradrenaline reuptake inhibitor duloxetine for the
treatment of interstitial cystitis: results of an observational study. J Urol 2007 Feb;177(2):552-5.
http://www.ncbi.nlm.nih.gov/pubmed/17222632
12. O’Conor VJ. Clorpactin WCS-90 in the treatment of interstitial cystitis. Q Bull Northwest Univ Med Sch
1955;29(4):293-5.
http://www.ncbi.nlm.nih.gov/pubmed/13273619
13. Wishard WN Jr, Nourse MH, Mertz JH. Use of Clorpactin WCS 90 for relief of symptoms due to
interstitial cystitis. J Urol 1957 Mar;77(3):420-3.
http://www.ncbi.nlm.nih.gov/pubmed/13417272
14. Messing EM, Freiha FS. Complication of Clorpactin WCS90 therapy for interstitial cystitis. Urology
1979 Apr;13(4):389-92.
http://www.ncbi.nlm.nih.gov/pubmed/219578
15. Murnaghan GF, Saalfeld J, Farnworth RH. Interstitial cystitis - treatment with Clorpactin WCS 90. Br J
Urol 1970 Dec;42(6):744.
http://www.ncbi.nlm.nih.gov/pubmed/5491939
16. von Heyden B, Schmid HP. [Intravesical therapy of interstitial cystitis.] Urologe A 2000 Nov;39(6):
542-4.
http://www.ncbi.nlm.nih.gov/pubmed/11138274
17. Hanno P. Interstitial cystitis and related diseases. In: Walsh PC, Retik AB, Stamey TA, Vaughan ED,
eds. Campbell’s Urology. Philadelphia: WB Saunders Co., 1998, pp. 648.
3.2.16 Non-pharmacological treatments
Behavioural bladder training techniques are attractive for BPS patients with predominant symptoms of
frequency/urgency but hardly any pain. Parsons et al. (1) included 21 selected BPS patients in a protocol
that focused on progressively increasing micturition intervals. Fifteen patients reported a 50% decrease in
urgency, frequency and nocturia, and there was a moderate increase in bladder capacity. Chaiken et al. (2)
retrospectively analysed 42 patients, who had been instructed in diary keeping, timed voiding, controlled fluid
intake, and pelvic floor muscle training. After 12 weeks, voiding intervals increased by a mean 93 min and daily
micturition was reduced by an average of nine voids. Overall, 88% of the patients reported markedly improved
or improved symptoms.
Diet. Dietary restrictions are among the many physical self-care strategies found among BPS patients (3).

64 UPDATE FEBRUARY 2012
In an analysis of the Interstitial Cystitis Data Base (ICDB) cohort study, special diets were among the five
most commonly used therapies (4). Bade et al. (5) have found that BPS patients consume significantly fewer
calories, less fat and coffee, but more fibre. Scientific data on a rationale for such diets are unavailable. The
concentration of some metabolites and amino acids appears to be changed in BPS (6).
A study of the metabolism of the arylalkylamines (tryptophan, tyrosine, tyramine and phenylalanine)
in 250 patients revealed an inability to synthesise normal amounts of serotonin and MHPG noradrenaline
metabolite. In this study, dietary restriction of acid foods and arylalkylamines lessened the symptoms, but
did not alter specific abnormalities in dopamine metabolism. In another, non-randomised, prospective study
of BPS patients with nutrition-related exacerbations, calcium glycerophosphate was reported to ease food-
related flares (7). The observed efficacy seems little better than would be expected with placebo.
Overall, dietary management is a common self-care strategy in BPS and offers a cost-effective
therapeutic approach. Comprehensive instructions on how to identify individual trigger foods are given in the
IC-Network Patient Handbook (8). However, scientific data are limited and dietary restriction alone does not
produce complete symptomatic relief.
Acupuncture. In non-curable and agonising diseases like BPS, desperate patients often try complementary
medicines, such as acupuncture. However, scientific evidence for such treatments is often poor, with
contradictory results from a few low-evidence reports on acupuncture, with any effects appearing to be limited
and temporary. A significant increase in capacity occurred after acupuncture in 52 women with 85% reporting
an improvement in frequency, urgency and dysuria and symptoms (9). However, at follow-up at 1 and 3 years,
these effects were no longer detectable and the authors concluded that repeated acupuncture was necessary
to maintain beneficial effects (10).
In a non-randomised comparison in women with urethral syndrome, 128 treated by acupuncture
and traditional Chinese medicine were compared with 52 treated by western medicine as controls. Efficacy
rates and urodynamic parameters were significantly better in the acupuncture group (11). In contrast, in a
prospective study on the effect of acupuncture in BPS (12), no differences in frequency, voided volumes or
symptom scores were noted, and only one patient improved for a short period of time.
Hypnosis is a therapeutic adjunct in the management of cancer, surgical disease and chronic pain. Although
used in urological patients (13,14), there are no scientific data on its effect on BPS symptoms.
Physiotherapy. General body exercise may be beneficial in some BPS patients (15). An uncontrolled trial of
transvaginal manual therapy of the pelvic floor musculature (Thiele massage) in 21 BPS patients with high-tone
dysfunction of the pelvic floor resulted in significant improvement on several assessment scales (16). Langford
(17) has prospectively examined the role of specific levator ani trigger point injections in 18 women with CPP.
Each trigger point was identified by intravaginal palpation and injected with 5 mL of a mixture of 10 mL 0.25%
bupivacaine, 10 mL 2% lidocaine and 1 mL (40 mg) triamcinolone. Thirteen (72%) women improved with the
first trigger point injection, with six (33%) women being completely pain-free.
Intravaginal electrical stimulation was applied to 24 women with CPP in the form of ten 30-min applications,
two or three times weekly. Stimulation was effective in alleviating pain, as evaluated at the end of treatment
and 2 weeks, 4 weeks and 7 months after completion of treatment (P < 0.05). There were significantly fewer
complaints of dyspareunia following treatment (P = 0.0005) (18).
3.2.16.1 References
1. Parsons CL, Koprowski PF. Interstitial cystitis: successful management by increasing urinary voiding
intervals. Urology 1991 Mar;37(3):207-12.
http://www.ncbi.nlm.nih.gov/pubmed/2000675
2. Chaiken DC, Blaivas JG, Blaivas ST. Behavioral therapy for the treatment of refractory interstitial
cystitis. J Urol 1993 Jun;149(6):1445-8.
http://www.ncbi.nlm.nih.gov/pubmed/8501784
3. Webster DC, Brennan T. Use and effectiveness of physical self-care strategies for interstitial cystitis.
Nurse Pract 1994 Oct;19(10):55-61.
http://www.ncbi.nlm.nih.gov/pubmed/7529390
4. Rovner E, Propert KJ, Brensinger C, et al. Treatments used in women with interstitial cystitis: the
interstitial cystitis data base (ICDB) study experience. The Interstitial Cystitis Data Base Study Group.
Urology 2000 Dec;56(6):940-5.
http://www.ncbi.nlm.nih.gov/pubmed/11113737

UPDATE FEBRUARY 2012 65
5. Bade JJ, Peeters JM, Mensink HJ. Is the diet of patients with interstitial cystitis related to their
disease? Eur Urol 1997;32(2):179-83.
http://www.ncbi.nlm.nih.gov/pubmed/9286650
6. Gillespie L. Metabolic appraisal of the effects of dietary modification on hypersensitive bladder
symptoms. Br J Urol 1993 Sep;72(3):293-7.
http://www.ncbi.nlm.nih.gov/pubmed/8220989
7. Bologna RA, Gomelsky A, Lukban JC, et al. The efficacy of calcium glycerophosphate in the
prevention of food-related flares in interstitial cystitis. Urology 2001 Jun;57(6 Suppl 1):119-20.
http://www.ncbi.nlm.nih.gov/pubmed/11378102
8. Osborne JH, Manhattan D, Laumnn B. IC and Diet. In: Osborne JH, ed. The Interstitial Cystitis
Network Patient Handbook. Chapter 5. Santa Rosa, CA, USA: The Interstitial Cystitis Network,
1999;pp. 43-62 [access date February 2011].
9. Chang PL. Urodynamic studies in acupuncture for women with frequency, urgency and dysuria. J Urol
1988 Sep;140(3):563-6.
http://www.ncbi.nlm.nih.gov/pubmed/3411675
10. Chang PL, Wu CJ, Huang MH. Long-term outcome of acupuncture in women with frequency, urgency
and dysuria. Am J Chin Med 1993;21(3-4):231-6.
http://www.ncbi.nlm.nih.gov/pubmed/8135166
11. Zheng H, Wang S, Shang J, et al. Study on acupuncture and moxibustion therapy for female urethral
syndrome. J Tradit Chin Med 1998 Jun;18(2):122-7.
http://www.ncbi.nlm.nih.gov/pubmed/10437230
12. Geirsson G, Wang YH, Lindström S, et al. Traditional acupuncture and electrical stimulation of the
posterior tibial nerve. A trial in chronic interstitial cystitis. Scand J Urol Nephrol 1993;27(1):67-70.
http://www.ncbi.nlm.nih.gov/pubmed/8493470
13. Lynch DF Jr. Empowering the patient: hypnosis in the management of cancer, surgical disease and
chronic pain. Am J Clin Hypn 1999 Oct;42(2):122-30.
http://www.ncbi.nlm.nih.gov/pubmed/10624023
14. Barber J. Incorporating hypnosis in the management of chronic pain. In: Barber J, Adrian C, eds.
Psychological Approaches in the Management of Pain. New York: Brunner/Mazel, 1982; pp. 60-83.
15. Karper WB. Exercise effects on interstitial cystitis: two case reports. Urol Nurs 2004 Jun;24(3):202-4.
http://www.ncbi.nlm.nih.gov/pubmed/15311489
16. Oyama IA, Rejba A, Lukban JC, et al. Modified Thiele massage as therapeutic intervention for female
patients with interstitial cystitis and high-tone pelvic floor dysfunction. Urology 2004 Nov;64(5):862-5.
http://www.ncbi.nlm.nih.gov/pubmed/15533464
17. Langford CF, Udvari Nagy S, Ghoniem GM. Levator ani trigger point injections: An underutilized
treatment for chronic pelvic pain. Neurourol Urodyn 2007;26(1):59-62.
http://www.ncbi.nlm.nih.gov/pubmed/17195176
18. de Oliveira Bernardes N, Bahamondes L. Intravaginal electrical stimulation for the treatment of chronic
pelvic pain. J Reprod Med 2005 Apr;50(4):267-72.
http://www.ncbi.nlm.nih.gov/pubmed/15916211
3.2.17 Surgical treatment
When all efforts fail to relieve disabling symptoms, surgical removal of the diseased bladder is the ultimate
option (1-4). Three major techniques of bladder resection are common:
• supratrigonal(i.e.trigone-sparing)cystectomy
• subtrigonalcystectomy
• radicalcystectomyincludingexcisionoftheurethra.
All techniques require substitution of the excised bladder tissue, mostly performed with bowel segments.
Techniques without bladder removal. As early as 1967, Turner-Warwick reported that mere bladder
augmentation without removal of the diseased tissue was not appropriate (5). Sporadic reports that unresected
BPS bladders cease to cause symptoms when excluded from the flow or urine are scarce (6,7).
Supratrigonal cystectomy with subsequent bladder augmentation represents the most favoured continence-
preserving surgical technique. Various intestinal segments have been used for trigonal augmentation, including
ileum (8-16), ileocaecum (15-22), right colon (8,16,23), and sigmoid (10,12,13,18,22). Substituting gastric
segments (24,25) seems to be less helpful because the production of gastric acids may maintain dysuria and
persistent pain.
The therapeutic success of supratrigonal cystectomy has been reported in many studies. In 1966,
von Garrelts reported excellent results in 8/13 patients with a follow-up of 12-72 months (12). In 1977, Bruce et

66 UPDATE FEBRUARY 2012
al. achieved satisfactory relief of BPS symptoms by ileocystoplasty and colocystoplasty in eight patients (10).
Dounis and Gow have reported seven BPS patients whose pain and frequency were considerably improved
after supratrigonal cystectomy with ileocaecal augmentation (26).
In 1991, Kontturi et al. used segments of colon and sigmoid colon in 12 cases (22). All five patients
augmented with sigmoid colon remained symptom-free over 4.7 years of follow-up. Two of seven cases
augmented with colon required secondary cystectomy with formation of an ileal conduit. Nielsen et al. have
reported a series of eight patients undergoing supratrigonal cystectomy with ileocaecocystoplasty.
Although symptoms resolved in two patients, treatment failure in another six necessitated secondary
cystectomy and ileal conduit formation (17).
Linn et al. (27) have followed six BPS patients after supratrigonal cystectomy with ileocaecal
augmentation for a period of 30 months, and have reported that all patients were symptom-free and voided
spontaneously.
In 2002, Van Ophoven et al. (1) reported the long-term results of trigone-preserving cystectomy and
consecutive orthotopic substitution enteroplasty in 18 women with BPS, using ileocaecal (n = 10) or ileal
(n = 8) segments. At a mean follow-up of nearly 5 years, 14 patients were completely pain-free, 12 voided
spontaneously, and 15 had complete resolution of dysuria. Ileocaecal bowel segments showed superior
functional results, because in the group augmented with ileum, three patients required self-catheterisation
and one a suprapubic catheter. Overall, surgery achieved a significant improvement in diurnal and nocturnal
frequencies, functional bladder capacity and symptom scores, with only two treatment failures.
In more recent reports with longer follow-up, the debate on the outcome of BPS patients undergoing
cystectomy continues and results vary greatly between different surgeons and patient populations.
Chakravarti (28) presented a retrospective review of 11 patients, who had undergone a trigone-preserving
orthotopic substitution caecocystoplasty for intractable BPS Type 3 C and were followed up for a mean period
of 9 years. All had symptomatic relief and an increase in bladder capacity to normal. There was no mortality
and minimal postoperative morbidity, with two patients requiring intermittent self-catheterisation due to high
residual volumes. No significant urinary reflux or metabolic complications were noted. However, two patients
required cystectomy after 4 and 6 years, respectively, due to recurrent trigonal disease in one patient and
urethrotrigonal hypersensitivity following intermittent self-catheterisation in the other. One patient developed an
advanced adenocarcinoma in the caecal segment 7 years after the primary operation.
Blaivas et al. (29) have reported less favourable results. Long-term outcomes of augmentation
enterocystoplasty or continent urinary diversion were analysed in 76 patients with benign urological disorders,
including seven with a clinical diagnosis of BPS. The BPS patients all failed surgical treatment because of
persistent pelvic pain and failure to achieve adequate bladder capacity, rather than because of incontinence.
The authors currently consider BPS to be a contraindication for enterocystoplasty.
In contrast, Navalón et al. (30) have reported a 32-month follow-up of four women with refractory
BPS who underwent supratrigonal cystectomy with orthotopic substitution ileocystoplasty. Suprapubic pain
disappeared in all cases, as well as lower urinary tract symptoms, with good control of urinary frequency day
and night in the immediate postoperative period. All patients reported high satisfaction with the outcome.
Subtrigonal cystectomy. Although less popular, subtrigonal cystectomy has also been reported (27,31-34).
Subtrigonal resection has the potential of removing the trigone as a possible disease site, but at the cost of
requiring ureteral reimplantation with associated risks of leakage, stricture, and reflux. Nurse et al. reported
trigonal disease in 50% within their cohort (13/25) and blamed surgical failures on the trigone left in place (35).
In contrast, Linn et al. have indicated that the level of resection was not solely responsible for
treatment success. While completely curing six patients by supratrigonal resection, there were three failures
among 17 subtrigonal resections, and half of the successful subtrigonal resections required self-catheterisation
to support voiding of the ileocaecal augmentate (27). A recent report on female sexuality after cystectomy and
orthotopic ileal neobladder (36) describes eight patients. Pain was relieved in all eight, but only one regained a
normal sexual life postoperatively.
Selecting patients and technique. BPS is benign and does not shorten life, so that operative procedures rank
last in the therapeutic algorithm. However, severely refractory patients should not have to tolerate unsuccessful
conservative treatments for several years when surgical options are available.
Detailed counselling and informed consent must precede any irreversible type of major surgery,
which should only be undertaken by experienced surgeons. The choice of technique is influenced by the
experience of the surgeon. The appropriate extent of tissue resection should be based on the endoscopic
and histopathological findings. Some surgeons recommend preoperative cystoscopy and bladder capacity as
a prognostic parameter for operative success (7). Responders and failures following orthotopic substitution
differed in mean preoperative bladder capacity (200 vs. 525 mL, respectively) (17). These findings have been

UPDATE FEBRUARY 2012 67
supported by Peeker et al. (37), who found that patients with end-stage BPS Type 3 C had excellent results
following ileocystoplasty, whereas patients with non-ulcer disease were not helped. These results have recently
been confirmed by another study from the same institution.
A retrospective analysis of 47 patients fulfilling the NIH criteria, who underwent reconstructive surgery
using various techniques during 1978-2003 (38), resulted in complete symptom resolution in 32/34 patients
with classic Hunner-type disease, but only 3/13 patients with non-ulcer disease.
Cystectomy with formation of an ileal conduit still ranks first in current US practice trends in surgical BPS
therapy (39). For cosmetic reasons, however, techniques of continent diversion are preferred, particularly in
younger patients. After orthotopic bladder augmentation, particularly when removing the trigone, voiding may
be incomplete and require intermittent self-catheterisation. Patients considering these procedures should
be advised and must be considered capable of performing, accepting and tolerating self-catheterisation.
For patients with BPS who develop recurrent pain in the augmented bladder or continent pouch after
enterocystoplasty or continent urinary diversion, Elzawahri (40) has recommended retubularisation of a
previously used bowel segment to form a urinary conduit.
For younger patients, it may be important to know that pregnancies with subsequent lower-segment
Caesarean section after ileocystoplasty have been reported (41). Reconstructive surgery for refractory BPS
is an appropriate last resort only for well-selected patients with refractory end-stage disease. The decision to
embark on major reconstructive surgery should be preceded by a thorough preoperative evaluation, with an
emphasis on assessment to determine the relevant disease location and subtype.
A summary of the treatment options for BPS, including LE and GR is given in the next section. Figure
6 and 7 are algorithms for the diagnosis and therapy of BPS based on the information discussed above.
3.2.18 Conclusions and recommendations: treatment of BPS
Conclusions LE
None of the present existing treatments have effect on all BPS subtypes or phenotypes. 4
Conventional analgesics have little efficacy. Opioids are effective in controlling BPS pain. 2b
Corticosteroids are not recommended as long-term treatment. 3
Hydroxyzine has limited efficacy shown in RCT and is effective in associated non bladder diseases. 1b
Limited data exist on effectiveness of cimetidine in BPS. 2b
Amitriptyline is effective in pain and related symptoms of BPS. 1b
Oral pentosanpolysulphate sodium is effective in pain and related symptoms of BPS. 1a
Oral pentosanpolysulphate sodium plus subcutaneous heparin is effective in pain and related
symptoms of BPS especially in patients initially low responders to pentosanpolysulphate sodium alone.
1b
Only limited data exist on the effectiveness of antibiotics in the treatment of BPS. 2b
Insufficient data for the effectiveness of prostaglandins in BPS exist. Adverse effects are frequent. 3
Global response on cyclosporin A was superior to pentosanpolysulphate sodium, but associated with
more adverse effects.
1b
Duloxetin has shown no effect and tolerability is poor. 2b
Oxybutynin has limited effect in BPS pain, but data are scant. 3
Only insufficient data exist for the effectiveness of gabapentin in BPS. 3
Only insufficient data exist for the effectiveness of suplatast tosilate in BPS. 3
Preliminary data showed effectiveness of quercetin alone and in multimodal uncontrolled studies. 3
Intravesical lidocaine plus sodium bicarbonate is effective in the short term. 1b
Intravesical pentosanpolysulphate sodium is effective based on limited data and may enhance effect of
oral treatment.
1b
There are limited data on the effectiveness of intravesical heparin. 3
Intravesical hyaluronic acid may have long term effects in BPS patients with positive intravesical
modified KCl test.
2b
Intravesical chondroitin sulphate may be effective according to non-randomised studies. Published
RCTs are underpowered.
2b
Intravesical DMSO is effective in the treatment of BPS, but side effects have to be considered. 1b
Intravesical submucosal BTX-A injection plus hydrodistension has sustained and significantly improved
effect over hydrodistension alone.
1b

68 UPDATE FEBRUARY 2012
Only limited data exist on the effectiveness of BTX-A injection into detrusor or trigone. 3
Data on effectiveness of intravesical vanilloids are contradictory. Largest of RCTs without efficacy. 1b
Intravesical Bacillus Calmette Guérin (BCG) is not effective in BPS. 1b
Intravesical clorpactin has insufficient data to support effectiveness and high complication rates. 3
There is only insufficient data to support effectiveness of bladder distension. 3
Scarce data indicate electromotive drug administration may have a beneficial effect in patient subsets. 3
Transurethral resection (Coagulation and laser) may be effective in BPS type 3 C. 3
Sacral neuromodulation may be effective in BPS. 3
Pudendal nerve stimulation is superior to sacral nerve stimulation for the treatment of BPS. 1b
Bladder training may be effective in patients with predominant urinary symptoms and little pain. 3
Manual and physical therapy may have limited effects. 3
Avoidance of some food and drink avoids pain triggering. 3
Acupuncture: data contradictory. 3
Psychological therapy may be effective in ameliorating coping with disease. 3
No definitive conclusion on the effectiveness of surgical organ removal for BPS can be drawn based on
large variability results in reported series.
3
Recommendations GR
Subtype and phenotype-oriented therapy for BPS is recommended. A
Multimodal behavioural, physical and psychological techniques should always be considered alongside
oral or invasive treatments for BPS.
A
Opioids might be used in BPS in disease flare-ups. Long term application solely if all treatments failed. C
Corticosteroids are not recommended as long-term treatment. C
Hydroxyzine is recommended for use in BPS. A
Consider cimetidine as valid oral option before invasive treatments. B
Amitriptyline is recommended for use in BPS. A
Oral
pentosanpolysulphate sodium
is recommended for use in BPS. A
Treatment with oral
pentosanpolysulphate sodium
plus subcutaneous heparin is recommended
especially in low responders to
pentosanpolysulphate sodium
alone.
A
Antibiotics can be offered when infection is present or highly suspected. C
Prostaglandins are not recommended. Insufficient data on BPS, adverse effects considerable. C
Cyclosporin A might be used in
BPS
but adverse effects are significant and should be carefully
considered.
B
Duloxetin is not recommended for BPS treatment. C
Oxybutynin might be considered for the treatment of BPS. C
Gabapentin might be considered in oral treatment of BPS. C
Consider intravesical lidocain plus sodium bicarbonate prior to more invasive methods. A
Consider intravesical
pentosanpolysulphate sodium
before more invasive treatment alone or combined
with oral
pentosanpolysulphate sodium
.
A
Consider intravesical heparin before more invasive measures alone or in combination treatment. C
Consider intravesical hyaluronic acid before more invasive measures. B
Consider intravesical chondroitin sulphate before more invasive measures. B
Consider intravesical DMSO before more invasive measures. A
Consider intravesical bladder wall and trigonal injection of BTX-A if intravesical instillation therapies
failed.
C
Consider submucosal injection of BTX-A plus hydrodistension if intravesical instillation therapies failed. A
Intravesical therapy with Bacillus Calmette Guérin is not recommended in BPS. A
Intravesical therapy with clorpactin is not recommended in BPS. A
Intravesical therapy with vanilloids is not recommended in BPS. C
Bladder distension is not recommended as a treatment of BPS. C

UPDATE FEBRUARY 2012 69
Electromotive drug administration might be considered before more invasive measures. C
Consider transurethral resection (or coagulation or laser) of bladder lesions, but in BPS type 3 C only B
Neuromodulation might be considered before more invasive interventions. B
Consider bladder training in patients with little pain. B
Consider manual and physical therapy in first approach. B
Consider diet avoidance of triggering substances. C
Accupuncture is not recommended. C
Consider psychological therapy in multimodal approach. B
All ablative organ surgery should be last resort for experienced and BPS knowledgeable surgeons only. A
DMSO = dimethyl sulphoxide; BPS = bladder pain syndrome.
Figure 6: diagnosis and therapy of BPS
Figure 7: algorithm for BPS Type 3 C
Urine culture
Uroflowmetry
Cystoscopy with
hydrodistension
Bladder biopsy
Pelvic floor muscle
testing
Assessment
Grade A recommended
Micturition diary
Treatment
Grade B recommended
Not recommended
Standard: Hydroxyzine, Amitriptyline, Pentosanpolysulphate
Intravesical: PPS, DMSO, onabotulinum toxin A plus hydrodistension
Oral: Cimetidine, cyclosporin A
Intravesical: hyaluronic acid, chondroitin sulphate
Bacillus Calmette Guerin
Intravesical Chlorpactin
Electromotive drug administration for intravesical drugs
Neuromodulation, bladder training, physical therapy
Psychological therapy
Data on surgical treatment are largely variable
Phenotyping
ICSI score list
Other comments
Coagulation and laser only for Hunner’s lesions
Hunner lesion at cystoscopy
TUR / laser
Adequate:
* Retreat when necessary
Inadequate:
* Start other treatment
* Oral agents
* TENS
* Complimentary medicine
Inadequate relief:
* Start Intravesical therapy
Still inadequate response:
* Refer to specialist
pain management unit
Bladder Pain Syndrome
yes no

70 UPDATE FEBRUARY 2012
3.2.19 References
1. van Ophoven A, Oberpenning F, Hertle L. Long-term results of trigone-preserving orthotopic
substitution enterocystoplasty for interstitial cystitis. J Urol 2002 Feb;167(2 Pt 1):603-7.
http://www.ncbi.nlm.nih.gov/pubmed/11792927
2. Loch A, Stein U. [Interstitial cystitis. New aspects in diagnosis and therapy]. Urologe A 2004
Sep;43(9):1135-46.
http://www.ncbi.nlm.nih.gov/pubmed/15322757
3. Oberpenning F, van Ophoven A, Hertle L. [Chronic interstitial cystitis.] Deutsches Ärzteblatt 2002,
99:204-8. [article in German]
4. Oberpenning F, Van Ophoven A, Hertle L. Interstitial cystitis: an update. Curr Opin Urol 2002
Jul;12(4):321-32.
http://www.ncbi.nlm.nih.gov/pubmed/12072654
5. Warwick R, Ashkan M. The functional results of partial, subtotal and total cystoplasty with special
reference to ureterocecocystoplasty, selective sphincterotomy and cystoplasty. Br J Urol 1967
Feb;39(1):3-12.
http://www.ncbi.nlm.nih.gov/pubmed/5336762
6. Messing EM, Stamey TA. Interstitial cystitis: early diagnosis, pathology, and treatment. Urology 1978
Oct;12(4):381-92.
http://www.ncbi.nlm.nih.gov/pubmed/213864
7. Freiha FS, Faysal MH, Stamey TA. The surgical treatment of intractable interstitial cystitis. J Urol 1980
May;123(5):632-4.
http://www.ncbi.nlm.nih.gov/pubmed/7420547
8. Badenoch AW. Chronic interstitial cystitis. Br J Urol 1971 Dec;43(6):718-21.
http://www.ncbi.nlm.nih.gov/pubmed/5159574
9. Awad SA, Al-Zahrani HM, Gajewski JB, et al. Long-term results and complications of augmentation
ileocystoplasty for idiopathic urge incontinence in women. Br J Urol 1998 Apr;81(4):569-73.
http://www.ncbi.nlm.nih.gov/pubmed/9598629
10. Bruce PT, Buckham GJ, Carden AB, et al. The surgical treatment of chronic interstitial cystitis. Med J
Aust 1977 Apr;1(16):581-2.
http://www.ncbi.nlm.nih.gov/pubmed/875802
11. Christmas TJ, Holmes SA, Hendry WF. Bladder replacement by ileocystoplasty: the final treatment for
interstitial cystitis. Br J Urol 1996 Jul;78(1):69-73.
http://www.ncbi.nlm.nih.gov/pubmed/8795403
12. von Garrelts B. Interstitial cystitis: thirteen patients treated operatively with intestinal bladder
substitutes. Acta Chir Scand 1966 Oct;132(4):436-43.
http://www.ncbi.nlm.nih.gov/pubmed/5972716
13. Guillonneau B, Toussaint B, Bouchot O, et al. [Treatment of interstitial cystitis with sub-trigonal
cystectomy and enterocystoplasty.] Prog Urol 1993 Feb;3(1):27-31.
http://www.ncbi.nlm.nih.gov/pubmed/8485591
14. Koskela E, Kontturi M. Function of the intestinal substituted bladder. Scand J Urol Nephrol
1982;16(2):129-33.
http://www.ncbi.nlm.nih.gov/pubmed/7123162
15. Shirley SW, Mirelman S. Experiences with colocystoplasties, cecocystoplasties and ileocystoplasties
in urologic surgery: 40 patients. J Urol 1978 Aug;120(2):165-8.
http://www.ncbi.nlm.nih.gov/pubmed/671623
16. Webster GD, Maggio MI. The management of chronic interstitial cystitis by substitution cystoplasty.
J Urol 1989 Feb;141(2):287-91.
http://www.ncbi.nlm.nih.gov/pubmed/2913346
17. Nielsen KK, Kromann-Andersen B, Steven K, et al. Failure of combined supratrigonal cystectomy and
Mainz ileovcecocystoplasty in intractable interstitial cystitis: is histology and mast cell count a reliable
predictor for the outcome of surgery? J Urol 1990 Aug;144(2 Pt 1):255-8; discussion 258-9.
http://www.ncbi.nlm.nih.gov/pubmed/2374189
18. Hradec EA. Bladder substitution: indications and results in 114 operations. J Urol 1965 Oct;94(4):
406-17.
http://www.ncbi.nlm.nih.gov/pubmed/5320331
19. DeJuana CP, Everett JC Jr. Interstitial cystitis: experience and review of recent literature. Urology
1977 Oct;10(4):325-9.
http://www.ncbi.nlm.nih.gov/pubmed/919117
UPDATE FEBRUARY 2012 71
20. Utz DC, Zincke H.The masquerade of bladder cancer in situ as interstitial cystitis. J Urol 1974
Feb;111(2):160-1.
http://www.ncbi.nlm.nih.gov/pubmed/4810754
21. Whitmore WF 3rd, Gittes RF. Reconstruction of the urinary tract by cecal and ileocecal
cystoplasty:review of a 15-year experience. J Urol 1983 Mar;129(3):494-8.
http://www.ncbi.nlm.nih.gov/pubmed/6834531
22. Kontturi MJ, Hellström PA, Tammela TL, et al. Colocystoplasty for the treatment of severe interstitial
cystitis. Urol Int 1991;46(1):50-4.
http://www.ncbi.nlm.nih.gov/pubmed/2024372
23. Seddon JM, Best L, Bruce AW. Intestinocystoplasty in treatment of interstitial cystitis. Urology 1977
Nov;10(5):431-5.
http://www.ncbi.nlm.nih.gov/pubmed/919133
24. Leong CH. Use of the stomach for bladder replacement and urinary diversion. Ann R Coll Surg Engl
1978 Jul;60(4):283-9.
http://www.ncbi.nlm.nih.gov/pubmed/666231
25. Singla A, Galloway N. Early experience with the use of gastric segment in lower urinary tract
reconstruction in adult patient population. Urology 1997 Oct;50(4):630-5.
http://www.ncbi.nlm.nih.gov/pubmed/9338749
26. Dounis A, Gow JG. Bladder augmentation-a long-term review. Br J Urol 1979 Aug;51(4):264-8.
http://www.ncbi.nlm.nih.gov/pubmed/466001
27. Linn JF, Hohenfellner M, Roth S, et al. Treatment of interstitial cystitis: comparison of subtrigonal and
supratrigonal cystectomy combined with orthotopic bladder substitution. J Urol 1998 Mar;159(3):
774-8.
http://www.ncbi.nlm.nih.gov/pubmed/9474146
28. Chakravarti A, Ganta S, Somani B, et al. Caecocystoplasty for intractable interstitial cystitis: long-term
results. Eur Urol 2004 Jul;46(1):114-7.
http://www.ncbi.nlm.nih.gov/pubmed/15183556
29. Blaivas JG, Weiss JP, Desai P, et al. Long-term followup of augmentation enterocystoplasty and
continent diversion in patients with benign disease. J Urol 2005 May;173(5):1631-4.
http://www.ncbi.nlm.nih.gov/pubmed/15821519
30. Navalón Verdejo P, Ordoño Domínguez F, De la Torre Abril L, et al. [Orthotopic bladder substitution in
the treatment of interstitial cystitis.] Arch Esp Urol 2005 Sep;58(7):605-10.
http://www.ncbi.nlm.nih.gov/pubmed/16294782
31. Bejany DE, Politano VA. Ileocolic neobladder in the woman with interstitial cystitis and a small
contracted bladder. J Urol 1995 Jan;153(1):42-3.
http://www.ncbi.nlm.nih.gov/pubmed/7966787
32. Nurse DE, McCrae P, Stephenson TP, et al.The problems of substitution cystoplasty. Br J Urol 1988
May;61(5):423-6.
http://www.ncbi.nlm.nih.gov/pubmed/3395801
33. Lotenfoe RR, Christie J, Parsons A, et al. Absence of neuropathic pelvic pain and favorable
psychological profile in the surgical selection of patients with disabling interstitial cystitis. J Urol 1995
Dec;155(6):2039-42.
http://www.ncbi.nlm.nih.gov/pubmed/7500453
34. Hughes OD, Kynaston HG, Jenkins BJ, et al. Substitution cystoplasty for intractable interstitial cystitis.
Br J Urol 1995 Aug;76(2):172-4.
http://www.ncbi.nlm.nih.gov/pubmed/7663907
35. Nurse DE, Parry JR, Mundy AR. Problems in the surgical treatment of interstitial cystitis. Br J Urol
1991 Aug;68(2):153-4.
http://www.ncbi.nlm.nih.gov/pubmed/1822961
36. Volkmer BG, Gschwend JE, Herkommer K, et al. Cystectomy and orthotopic ileal neobladder: the
impact on female sexuality. J Urol 2004 Dec;172(6 Pt 1):2353-7.
http://www.ncbi.nlm.nih.gov/pubmed/15538266
37. Peeker R, Aldenborg F, Fall M. The treatment of interstitial cystitis with supratrigonal cystectomy
and ileocystoplasty: difference in outcome between classic and nonulcer disease. J Urol 1998
May;159(5):1479-82.
http://www.ncbi.nlm.nih.gov/pubmed/9554337
38. Rössberger J, Fall M, Jonsson O, et al. Long-term results of reconstructive surgery in patients with
bladder pain syndrome/interstitial cystitis: subtyping is imperative. Urology 2007 Oct;70(4):638-42.
http://www.ncbi.nlm.nih.gov/pubmed/17991529

72 UPDATE FEBRUARY 2012
39. Gershbaum D, Moldwin R. Practice trends for the management of interstitial cystitis. Urology 2001
Jun;57(6 Suppl 1):119.
http://www.ncbi.nlm.nih.gov/pubmed/11378100
40. Elzawahri A, Bissada NK, Herchorn S, et al. Urinary conduit formation using a retubularized bowel
from continent urinary diversion or intestinal augmentations: ii. Does it have a role in patients with
interstitial cystitis? J Urol 2004;171(4):1559-62.
http://www.ncbi.nlm.nih.gov/pubmed/15017220
41. Shaikh A, Ahsan S, Zaidi Z. Pregnancy after augmentation cystoplasty. J Pak Med Assoc
2006;56(10):465-7.
http://www.ncbi.nlm.nih.gov/pubmed/17144396
3.3 Genital pain syndrome
3.3.1 Scrotal pain syndrome
Scrotal pain syndrome is the occurrence of persistent or recurrent episodic pain localised within the organs of
the scrotum, and may be associated with symptoms suggestive of urinary tract or sexual dysfunction. There is
no proven infection or other obvious local pathology. Scrotal pain syndrome is often associated with negative
cognitive, behavioural, sexual or emotional consequences, as well as with symptoms suggestive of lower
urinary tract and sexual dysfunction. Scrotal pain syndrome is a generic term and is used when the site of the
pain is not clearly testicular or epididymal. The pain is not in the skin of the scrotum as such, but perceived
within its contents, in a similar way to idiopathic chest pain.
3.3.2 Pathogenesis
The pathogenesis of chronic scrotal pain is diverse and in most cases unknown. Pain in the scrotum can be
divided into direct pain localised in the scrotum, or referred pain coming from another place or system in the
body. The problem is that we cannot always make that division in clinical practice. Direct pain is located in the
testes, epididymis, inguinal nerves or the vas deferens.
3.3.2.1 Testicular pain syndrome
Testicular pain syndrome is the occurrence of persistent or recurrent episodic pain perceived in the testes,
and may be associated with symptoms suggestive of urinary tract or sexual dysfunction. There is no proven
infection or other obvious local pathology. Testicular pain syndrome is often associated with negative cognitive,
behavioural, sexual or emotional consequences, as well as with symptoms suggestive of lower urinary tract
and sexual dysfunction. Previous terms have included orchitis, orchialgia and orchiodynia. These terms are no
longer recommended.
3.3.2.2 Epididymal pain syndrome
Epididymal pain syndrome is the occurrence of persistent or recurrent episodic pain perceived in the
epididymis, and may be associated with symptoms suggestive of urinary tract or sexual dysfunction. There
is no proven infection or other obvious local pathology. Epididymal pain syndrome is often associated with
negative cognitive, behavioural, sexual or emotional consequences, as well as with symptoms suggestive of
lower urinary tract and sexual dysfunction.
Structural abnormalities of the epididymis can be visualised using ultrasound. Patients with multiple
cysts may have pain caused by the compression that these cysts exert on the epididymis. Another local entity
is chronic epididymitis (1). Chronic epididymis may be associated with signs of inflammation: inflammatory or
obstructive chronic epididymitis (2).
3.3.2.3 Nerves
The ilioinguinal and genitofemoral nerves are the most prominent afferent nerves for the scrotum (3). The
inguinal nerves are especially important. It is generally accepted that pain after inguinal surgery (hernia)
is a consequence of damage to the nerves inside the spermatic cord (4). This is based on the anatomical
knowledge that all nerves involved in testicular pain merge in the spermatic cord (5). This fact has
consequences for the choice of treatment. The pudendal nerve supplies the skin of the perineum and the
posterior side of the scrotum. Pain in this area is pathognomic for pudendal neuropathy.
3.3.2.4 Post-vasectomy pain syndrome
Postvasectomy scrotal pain syndrome is a scrotal pain syndrome that follows vasectomy. Postvasectomy
scrotal pain syndrome is often associated with negative cognitive, behavioural, sexual or emotional
consequences, as well as with symptoms suggestive of lower urinary tract and sexual dysfunction.
Postvasectomy pain may be as frequent as 1% following vasectomy, possibly more frequent. The mechanisms
are poorly understood and it is for that reason considered a special form of scrotal pain syndrome.

UPDATE FEBRUARY 2012 73
Pathogenetically, it is thought that post-vasectomy pain is caused by the fact that the vas deferens is no longer
patent. This may lead to congestion in the epididymis which in turn gives rise to pain because of dilatation
of hollow structures (6). Incidence of post-vasectomy pain is 2-20% among all men who have undergone a
vasectomy (7). In men with post-vasectomy pain, only 2-6% have a VAS score > 5 (8). In a large cohort study
of 625 men, the likelihood of scrotal pain after 6 months was 14.7%. The mean pain severity on a VAS score
was 3.4/10. In the pain group, 0.9% had quite severe pain, noticeably affecting their daily life. In this cohort,
different techniques were used to perform the vasectomy. The risk of scrotal pain was significantly lower in the
no-scalpel vasectomy group, at 11.7% compared with 18.8% in the scalpel group (9).
3.3.2.5 Post-inguinal hernia repair
Chronic pain after inguinal hernia surgery is a well recognised phenomenon. An international working group
has set up guidelines for prevention and management of postoperative chronic pain following inguinal hernia
surgery. They have stated that the most important way of preventing pain is to identify and preserve all three
inguinal nerves (10). Chronic scrotal pain is a complication of hernia repair, but in trials, it is seldom reported or
it is put under the term chronic pain (not specified). In studies that have explicitly mentioned scrotal pain, there
was a difference in incidence between laparoscopic and open hernia repair. In almost all studies, the frequency
of scrotal pain was significantly higher in the laparoscopic than in the open group (4,11-13). In one particular
study, there was no difference at 1 year but after 5 years, the open group had far fewer patients with scrotal
pain (14).
3.3.2.6 Referred pain
Growing knowledge of pain mechanisms has taught us that pain felt in organ A can be caused by dysfunction
of structure B. The best known referred pain is of myofascial origin, especially the trigger points (see Chapter
9). Problems inside the bladder or abdominal cavity can also give rise to pain in the scrotal area. When making
a treatment plan for patients with scrotal pain, it is important to remember this phenomenon.
3.3.3 Diagnosis
A physical examination is mandatory in patients with scrotal pain. Gentle palpation of each component of the
scrotum is performed to search for masses and painful spots. A rectal examination is done to look for prostate
abnormalities and to examine the pelvic floor muscles. Scrotal ultrasound has limited value in finding the
cause of the pain. In > 80% of patients, ultrasound does not show abnormalities that have clinical implications
(15,16). If physical examination is normal, ultrasound can be performed to reassure the patient that there is no
pathology that needs therapy (mainly surgery). Ultrasound can be used to diagnose hydroceles, spermatoceles,
cysts and varicoceles. When abnormalities such as cysts are seen, this may play a role in therapeutic decision
making. In general practice, it seems that many urologists are performing ultrasound examination in almost all
patients. Swiss urologists, for instance, perform it in 93% of cases (17).
3.3.4 Treatment
Treatment of chronic scrotal pain is based on the principles of treating chronic pain syndromes, described
throughout these guidelines. It is becoming increasingly clear that advances in the non-surgical management of
testicular pain are mainly based on the emergence of pain relief as a specialty. Knowing this, it seems obvious
that referring to a multidisciplinary pain team or pain centre should be considered in an early phase of the
consultation (18). By doing this, surgery can be postponed or even avoided.
3.3.4.1 Conservative treatment
For conservative treatment, apart from pharmacotherapy, myofascial therapy by specialised physiotherapists
should be considered. The pelvic floor muscles should be tested and will often be found overactive,
which means that they contract when relaxation is needed. An overactive pelvic floor should be treated by
physiotherapy (19-21). More specific myofascial trigger points are found in the pelvic floor, but also in the lower
abdominal musculature. Treatment consists of applying pressure to the trigger point and stretching the muscle
(22,23) (see Chapter 9).
3.3.4.2 Surgery
In a survey among Swiss urologists, it was found that 74% would do an epididymectomy, 7% an inguinal
orchiectomy, and 6% a denervation (17). In the literature, there is consensus on postponing surgery until there
is no other option. The only treatment that seems to be effective is microsurgical denervation. Epididymectomy
is a choice in selected cases and orchiectomy is the last resort.
3.3.4.1.1 Microsurgical denervation
Considering the fact that all the nerves for the scrotal organs merge into the spermatic cord, it seems

74 UPDATE FEBRUARY 2012
reasonable to cut all these nerves in patients with pain. All the studies that have been done were cohort
studies but their success rates were high. The size of effect was so remarkable that it is recommended
that randomised studies are performed to obtain better proof. The three cohort studies that are found were
consistent in the indication criteria, the diagnostic methods applied, and the surgical approach used. All
had a follow-up of at least 20 months. They included patients with chronic scrotal pain who did not respond
to conservative treatment. Ultrasound showed no abnormalities and a spermatic cord block showed pain
relief of > 50%. The surgical approach is inguinal. The cord is transected in such a way that all identifiable
arterial structures, including testicular, cremasteric, deferential arteries and lymphatic vessels are left intact.
The surgery is performed under magnification by loupe or microscope. Complete relief of pain is achieved
in 71-96% and partial relief in 9-17%. This means that 12-15% had no relief of pain after denervation. The
complication of testicular atrophy was seen in 3-7% of the operated patients (24-26). There is no difference in
success based on the cause of pain. The laparoscopic route for denervation seems feasible but the results are
unclear (27).
3.3.4.1.2 Epididymectomy
There is to date no hard evidence available, but expert opinion is clear that epididymectomy should be
reserved for patients who have undergone denervation but still have pain. Epididymectomy shows different
results in various groups of patients. Epididymectomy shows the best results in patients with pain after
vasectomy, or pain on palpation of the epididymis and when ultrasound shows multiple cysts. Patients with
chronic epididymitis show bad results with epididymectomy.
The percentage of patients that are cured ranges from 50 to 92% (1,6,28-30). These results are also
from cohort studies but the fact that assessment can help in predicting the chance of success makes further
studies worthwhile. One study in our search has yielded different results, namely, that post-vasectomy patients
fared worse and that ultrasound did not help in predicting the result of the operation. No reason was found for
this result (9).
3.3.4.1.3 Orchiectomy
Orchiectomy is seen as the last resort in patients with intrascrotal pain, who do not respond to any other
treatment. There have been no studies than can help in making a rational decision on whether to perform
orchiectomy.
3.3.4.1.4 Vaso-vasostomy
In post-vasectomy pain syndrome, a vaso-vasostomy might help to overcome the obstruction and thereby
improve the pain. Some studies have shown good results but the quality of these studies was limited. Results
are as high as 69-84% (31,32).
3.3.5 Conclusions and recommendations: scrotal pain syndrome
Conclusions LE
The nerves in the spermatic cord play an important role in scrotal pain. 2b
Ultrasound of the scrotal content is not of help in diagnostics nor treatment of scrotal pain. 2b
Post-vasectomy pain is seen in a substantial number of men undergoing vasectomy. 2b
Scrotal pain is more often noticed after laparoscopic then after open inguinal hernia repair. 1b
Microsurgical denervation of the spermatic cord is an effective therapy for scrotal pain syndrome. 2b
Vaso-vasostomy is effective in post-vasectomy pain. 2b
Orchiectomy is the last resort in treating scrotal pain syndrome. 4
Recommendations GR
We recommend to start with general treatment options for chronic pelvic pain (see chapter 10). A
We recommend informing about the risk of post-vasectomy pain when counselling patients planned
for vasectomy.
A
To reduce the risk of scrotal pain, we recommend open instead of laparoscopic inguinal hernia repair. A
We recommend that during inguinal hernia repair all the nerves in the spermatic cord are identified. A
For patients who are treated surgically, we recommend microsurgical denervation of the spermatic
cord.
A
For patients who do not benefit from denervation we recommend to perform epididymectomy. B

UPDATE FEBRUARY 2012 75
We recommend that orchiectomy is reserved as last resort when every other treatment has failed. C
Figure 8: assessment and treatment algorithm for scrotal pain syndrome
3.3.6 References
1. Padmore DE, Norman RW, Millard OH. Analyses of indications for and outcomes of epididymectomy.
J Urol. 1996 Jul;156(1):95-6.
http://www.ncbi.nlm.nih.gov/pubmed/8648848
2. Nickel JC, Siemens DR, Nickel KR, et al. The patient with chronic epididymitis: characterization of an
enigmatic syndrome. J Urol. 2002 Apr;167(4):1701-4.
http://www.ncbi.nlm.nih.gov/pubmed/11912391
3. Rab M, Ebmer AJ, Dellon AL. Anatomic variability of the ilioinguinal and genitofemoral
nerve:implications for the treatment of groin pain. Plast Reconstr Surg 2001 Nov;108(6):1618-23.
http://www.ncbi.nlm.nih.gov/pubmed/11711938
4. Eklund A, Montgomery A, Bergkvist L, et al. Chronic pain 5 years after randomized comparison of
laparoscopic and Lichtenstein inguinal hernia repair. Br J Surg. 2010 Apr;97(4):600-8.
http://www.ncbi.nlm.nih.gov/pubmed/20186889
5. Heidenreich A, Olbert P, Engelmann UH. Management of chronic testalgia by microsurgical testicular
denervation. Eur Urol. 2002 Apr;41(4):392-7.
http://www.ncbi.nlm.nih.gov/pubmed/12074809
6. Sweeney P, Tan J, Butler MR, et al. Epididymectomy in the management of intrascrotal disease: a
critical reappraisal. Br J Urol. 1998 May;81(5):753-5.
http://www.ncbi.nlm.nih.gov/pubmed/9634056
7. Nariculam J, Minhas S, Adeniyi A, et al. A review of the efficacy of surgical treatment for
andpathological changes in patients with chronic scrotal pain. BJU Int 2007 May;99(5):1091-3.
http://www.ncbi.nlm.nih.gov/pubmed/17244279
8. Manikandan R, Srirangam SJ, Pearson E, et al. Early and late morbidity after vasectomy: a comparison
of chronic scrotal pain at 1 and 10 years. BJU Int. 2004 Mar;93(4):571-4.
http://www.ncbi.nlm.nih.gov/pubmed/15008732
9. Leslie TA, Illing RO, Cranston DW, et al. The incidence of chronic scrotal pain after vasectomy:
aprospective audit. BJU Int 2007 Dec;100(6):1330-3.
http://www.ncbi.nlm.nih.gov/pubmed/17850378
10. Alfieri S, Amid PK, Campanelli G, et al. International guidelines for prevention and management of
post-operative chronic pain following inguinal hernia surgery. Hernia. 2011 Jun;15(3):239-49.
http://www.ncbi.nlm.nih.gov/pubmed/21365287
11. Andersson B, Hallén M, Leveau P, et al. Year: 2004. Laparoscopic extraperitoneal inguinal hernia
repair versus open mesh repair: a prospective randomized controlled trialSurgery 5: 464-72
http://www.ncbi.nlm.nih.gov/pubmed/12773973
12. Wright D, Paterson C, Scott N, et al. Five-year follow-up of patients undergoing laparoscopic or open
groin hernia repair: A randomized controlled trial. Ann Surg. 2002 Mar;235(3):333-7.
http://www.ncbi.nlm.nih.gov/pubmed/11882754
13. Hallén M, Bergenfelz A, Westerdahl J. Laparoscopic extraperitoneal inguinal hernia repair versus open
mesh repair: long-term follow-up of a randomized controlled trial.Surgery. 2008 Mar;143(3):313-7.
http://www.ncbi.nlm.nih.gov/pubmed/18291251
Semen culture
Uroflowmetry
Ultrasound
scrotum (see text)
Pelvic floor muscle
testing
Assessment
Grade A recommended
Phenotyping
Treatment
Grade B recommended
Other comments
General treatment options for chronic pelvic pain - chapter 10
Inform patients undergoing vasectomy about the risk of pain
Microsurgical denervation of the spermatic cord
Epididymectomy, in case patient did not benefit from denervation
Orchiectomy is a last resort option, when everything else has failed
Ultrasound has no clinical implications on the further treatment
although physicians tend to still use ultrasound to reassure the patient
For surgeons: open hernia repair yields less scrotal pain
For surgeons: identify all nerves during hernia repair

76 UPDATE FEBRUARY 2012
14. Grant AM, Scott NW, O’Dwyer PJ, et al. Five-year follow-up of a randomized trial to assess pain and
numbness after laparoscopic or open repair of groin hernia.Br J Surg. 2004 Dec;91(12):1570-4.
http://www.ncbi.nlm.nih.gov/pubmed/15515112
15. van Haarst EP, van Andel G, Rijcken TH, et al. Value of diagnostic ultrasound in patients with
chronicscrotal pain and normal findings on clinical examination. Urology 1999 Dec;54(6):1068-72.
http://www.ncbi.nlm.nih.gov/pubmed/10604710
16. Lau MW, Taylor PM, Payne SR. The indications for scrotal ultrasound. Br J Radiol. 1999
Sep;72(861):833-7.
http://www.ncbi.nlm.nih.gov/pubmed/10645188
17. Strebel RT, Leippold T, Luginbuehl T, et al. Chronic scrotal pain syndrome: management among
urologists in Switzerland. Eur Urol. 2005 Jun;47(6):812-6.
http://www.ncbi.nlm.nih.gov/pubmed/15925078
18. Messelink EJ. The pelvic pain centre. World J Urol 2001 Jun;19(3):208-12.
http://www.ncbi.nlm.nih.gov/pubmed/11469609
19. Cornel EB, van Haarst EP, Schaarsberg RW, et al. The effect of biofeedback physical therapy in
menwith Chronic Pelvic Pain Syndrome Type III. Eur Urol 2005 May;47(5):607-11.
http://www.ncbi.nlm.nih.gov/pubmed/15826751
20. Hetrick DC, Glazer H, Liu YW, et al. Pelvic floor electromyography in men with chronic pelvic
painsyndrome: a case-control study. Neurourol Urodyn 2006;25(1):46-9.
http://www.ncbi.nlm.nih.gov/pubmed/16167354
21. Rowe E, Smith C, Laverick L, et al. A prospective, randomized, placebo controlled, double-blind
studyof pelvic electromagnetic therapy for the treatment of chronic pelvic pain syndrome with 1 year
offollowup. J Urol 2005 Jun;173(6):2044-7.
http://www.ncbi.nlm.nih.gov/pubmed/15879822
22. Anderson RU, Wise D, Sawyer T, et al. Integration of myofascial trigger point release and
paradoxicalrelaxation training treatment of chronic pelvic pain in men. J Urol 2005 Jul;174(1):155-60.
http://www.ncbi.nlm.nih.gov/pubmed/15947608
23. Srinivasan AK, Kaye JD, Moldwin R. Myofascial dysfunction associated with chronic pelvic floor pain:
management strategies. Curr Pain Headache Rep 2007 Oct;11(5):359-64
http://www.ncbi.nlm.nih.gov/pubmed/17894926
24. Strom KH, Levine LA. Microsurgical denervation of the spermatic cord for chronic orchialgia: long-
term results from a single center. J Urol. 2008 Sep;180(3):949-53.
http://www.ncbi.nlm.nih.gov/pubmed/18639271
25. Levine LA, Matkov TG. Microsurgical denervation of the spermatic cord as primary surgical treatment
of chronic orchialgia. J Urol. 2001 Jun;165(6 Pt 1):1927-9.
http://www.ncbi.nlm.nih.gov/pubmed/11371883
26. Heidenreich A, Olbert P, Engelmann UH. Management of chronic testalgia by microsurgical
testiculardenervation. Eur Urol 2002 Apr;41(4):392-7.
http://www.ncbi.nlm.nih.gov/pubmed/12074809
27. Cadeddu JA, Bishoff JT, Chan DY, et al. Laparoscopic testicular denervation for chronic orchalgia. J
Urol. 1999 Sep;162(3 Pt 1):733-5; discussion 735-6.
http://www.ncbi.nlm.nih.gov/pubmed/10458355
28. Granitsiotis P, Kirk D. Chronic testicular pain: an overview. Eur Urol 2004 Apr;45(4):430-6.
http://www.ncbi.nlm.nih.gov/pubmed/15041105
29. Sweeney CA, Oades GM, Fraser M, et al. Does surgery have a role in management of chronic
intrascrotal pain? Urology. 2008 Jun;71(6):1099-102.
http://www.ncbi.nlm.nih.gov/pubmed/18436286
30. Calleary JG, Masood J, Hill JT. Chronic epididymitis: is epididymectomy a valid surgical treatment? Int
J Androl. 2009 Oct;32(5):468-72.
http://www.ncbi.nlm.nih.gov/pubmed/18380787
31. Nangia AK, Myles JL, Thomas AJ Jr. Vasectomy reversal for the post-vasectomy pain syndrome:
aclinical and histological evaluation. J Urol 2000 Dec;164(6):1939-42.
http://www.ncbi.nlm.nih.gov/pubmed/11061886
32. Myers SA, Mershon CE, Fuchs EF. Vasectomy reversal for treatment of the post-vasectomy pain
syndrome. J Urol. 1997 Feb;157(2):518-20.
http://www.ncbi.nlm.nih.gov/pubmed/8996346
3.4 Urethral pain syndrome
3.4.1 Definition
Urethral pain syndrome is the occurrence of chronic or recurrent episodic pain perceived in the urethra, in the

UPDATE FEBRUARY 2012 77
absence of proven infection or other obvious local pathology. Urethral pain syndrome is often associated with
negative cognitive, behavioural, sexual or emotional consequences, as well as with symptoms suggestive of
lower urinary tract, sexual, bowel or gynaecological dysfunction. Urethral pain syndrome may occur in men and
women.
3.4.2 Pathogenesis
Based on the definition, there is no well-known pathogenetic mechanism responsible for urethral pain
syndrome. There are no data available to answer the question: “how common is dysuria in the presence
of negative rigorous investigation of the bladder and urethra?” Some suggestions have been proposed.
The intimate relation of the urethra with the bladder (both covered with urothelium) makes it plausible that
pathology seen in the bladder is also found in the urethra and causes the same symptoms. This is the case in
classifying urethral pain syndrome as a form of BPS. It is obvious that what might cause pain in the bladder
could be responsible for urethral pain. Mechanisms thought to be basic for BPS also apply to the urethra. This
means that the specific testing with potassium is used to support the theory of epithelial leakage (1,2). Urethral
syndrome is supposed to be the same as BPS in that the epithelium is leaking, thereby causing pain.
Another possible mechanism is the neuropathic hypersensitivity following urinary tract infection (3).
Symptoms recorded in patients with urethral pain syndrome can also be classified as referred pain from other
organs or from the myofascial system. Attention to the phenomenon of referred pain is important. See Chapter
9 for more on the myofascial origin of the pain.
The relationship with gynaecological and obstetric aspects is unclear. In a small group of patients with
urethral pain, it has been found that grand multiparity and delivery without episiotomy were more often seen in
patients with urethral syndrome, using univariate analysis (4).
3.4.3 Treatment
There is no specific treatment that can be advised. Management should be multidisciplinary and multimodal
(5). Laser therapy of the trigonal region may be a specific treatment. One trial comparing two forms of
laser reported good results, but did not compare with sham treatment (6). The majority of publications on
treatment of urethral pain syndrome have come from psychologists. In a 2007 review of treatment, Kaur and
Arunkalaivanan have concluded that “treatment at its best” is by “behavioral therapy including biofeedback,
meditation, bladder retraining, and hypnosis has been used with some success”, but no reference is given, and
no trials of these arose from the search. Baldoni et al. (7) have reported high rates of anxiety and depression,
and worsening of symptoms related to stress in patients with urethral pain syndrome The only treatment trial
found was by Baldoni et al. The psychological model that he used is not entirely clear: they have described
how “in some cases” psychotherapy enables patients to recognise “the emotional implications” of their urinary
problem, leading to both physical and psychological improvement. “Emotional implications” could mean
either emotional consequences, consistent with a cognitive behavioural model of chronic pain in which those
consequences, rather than the pain itself, are targeted to improve QoL, or it could mean implications for -
exposure of - emotional conflict or similar psychological disorder, which is presumed to be the aetiology of the
urethral pain.
Baldoni et al. recruited 36 female patients diagnosed with urethral syndrome in an Italian urology clinic
after negative urography, cystoscopy and urine culture, and urodynamic examination. Thirteen women were
randomly selected for psychotherapy, but the method was not blind or free of possible bias. Psychotherapy
was 12-16 weekly 1-h sessions, with additional fortnightly group discussion, and focused on associations
between urinary symptoms and emotion. Four patients were also prescribed low-dose antidepressants. The
control group received usual care but no psychological treatment.
Assessment of symptoms at 6 months and four years after the end of treatment (with loss of two
patients from each arm) showed substantial improvement in total urinary symptoms and additionally in pelvic
pain, with 9/11 psychotherapy patients with normal levels of urinary function at 6 months, and 8/11 with
normal levels at 4 years. Control patients were unchanged at both follow-up points. The trial had significant
weaknesses; in particular, the non-blind assignment to treatment condition, the non-standardised measures,
and, for the purposes of this review, the combination of all urinary symptoms so that treatment effects on pain
were obscured. The authors have noted that the lack of any credible intervention with controls makes it difficult
to conclude that it was the particular treatment, rather than the general provision of treatment, which brought
about recorded improvement. However, the results can be taken as encouraging the trial of psychological
methods, using orthodox outcome measures and more rigorous methodology.

78 UPDATE FEBRUARY 2012
3.4.4 Conclusions and recommendations: urethral pain syndrome
Conclusions LE
Urethral pain syndrome may be a part of BPS. 2a
Urethral pain may be neuropathic hypersensitivity following urinary tract infection. 2b
There is no specific treatment for urethral pain syndrome. 4
In patients with significant distress associated with bladder or urethral symptoms, psychological
treatment may be worth using to reduce distress and thereby improve function and quality of life.
4
Recommendations GR
We recommend to start with general treatment options for chronic pelvic pain (see chapter 10). A
We recommend that patients with urethral pain syndrome are treated in a multidisciplinary and
multimodal programme.
B
When patients are distressed, we recommend referring them for pain-relevant psychological
treatment to improve function and quality of life.
B
Figure 9: assessment and treatment algorithm for urethral pain syndrome
3.4.5 References
1. Parsons CL, Zupkas P, Parsons JK. Intravesical potassium sensitivity in patients with interstitialcystitis
and urethral syndrome. Urology 2001 Mar;57(3):428-32; discussion 432-3.
http://www.ncbi.nlm.nih.gov/pubmed/11248610
2. Parsons CL. The role of a leaky epithelium and potassium in the generation of bladder symptoms in
interstitial cystitis/overactive bladder, urethral syndrome, prostatitis and gynaecological chronic pelvic
pain. BJU Int. 2011 Feb;107(3):370-5.
http://www.ncbi.nlm.nih.gov/pubmed/21176078
3. Kaur H, Arunkalaivanan AS. Urethral pain syndrome and its management. Obstet Gynecol Surv
2007May;62(5):348-51; quiz 353-4.
http://www.ncbi.nlm.nih.gov/pubmed/17425813
4 Gürel H, Gürel SA, Atilla MK. Urethral syndrome and associated risk factors related to obstetrics and
gynecology.Eur J Obstet Gynecol Reprod Biol. 1999 Mar;83(1):5-7.
http://www.ncbi.nlm.nih.gov/pubmed/10221602
5. Yoon SM, Jung JK, Lee SB, et al. Treatment of female urethral syndrome refractory to antibiotics.
Yonsei Med J. 2002 Oct;43(5):644-51.
http://www.ncbi.nlm.nih.gov/pubmed/12402379
6. Costantini E, Zucchi A, Del Zingaro M, et al. Treatment of urethral syndrome: a prospective
randomized study with Nd:YAG laser. Urol Int. 2006;76(2):134-8.
http://www.ncbi.nlm.nih.gov/pubmed/16493214
7. Baldoni F, Baldaro B, Trombini G. Psychotherapeutic perspectives in urethral syndrome. Stress
Medicine 1995; 11: 79-84.
8. Kaur H, Arunkalaivanan AS. Urethral pain syndrome and its management. Obstet Gynecol Surv. 2007
May;62(5):348-51.
http://www.ncbi.nlm.nih.gov/pubmed/17425813
Uroflowmetry
Micturition diary
Pelvic floor muscle
testing
Phenotyping
Assessment
Grade A recommended
Treatment
Grade B recommended
Other comments
General treatment options for chronic pelvic pain - chapter 10
Treat in a multidisciplinary and multimodal programme
Pain-relevant psychological treatment to improve QoL and function
Data on urethral pain are very sparse and of limited quality

UPDATE FEBRUARY 2012 79
4. GYNAECOLOGICAL ASPECTS OF CHRONIC
PELVIC PAIN
4.1 Introduction
Chronis pelvic pain in urological and gynaecological practice is often complex and difficult to treat. The aim
is to try and determine a remediable cause and treat it using the most effective available therapy. However,
in 30% of cases, no cause is ever determined and this presents a therapeutic challenge to the attendant
physician (1).
4.2 Clinical history
Taking a detailed medical history is essential to making a diagnosis. The nature, frequency and site of the pain,
and its relationship to precipitating factors and the menstrual cycle, may provide vital clues to the aetiology.
A detailed menstrual and sexual history, including any history of sexually transmitted diseases and vaginal
discharge is mandatory. Discrete inquiry about previous sexual trauma may be appropriate.
4.3 Clinical examination
Abdominal and pelvic examination will exclude any gross pelvic pathology (tumours, scarring, and reduced
uterine mobility), as well as demonstrating the site of tenderness if present. Abnormalities in muscle function
should also be sought. Clinical pelvic examination should be a single digit examination if possible, but in most
cases a gentle double digit examination is tolerable and sometimes necessary. The usual bimanual examination
can generate severe pain so the examiner must proceed with caution. The examination of a woman with
CPP can be very difficult, and many authors recommend that it should be directed to the determination of
cutaneous allodynia along the dermatomes of the abdomen (T11-L1) and the perineum (S3). The degree of
tenderness of the muscles and on the perineum (perineal body, levators and obturator internus) should be
determined.
4.3.1 Investigations
Vaginal and endocervical swabs to exclude infection are mandatory and cervical cytology screening is
advisable. Pelvic imaging, using ultrasound scanning or magnetic resonance, can provide useful information
about pelvic anatomy and pathology. Any areas of tenderness detected can provide information related to the
possible presence of current or pre-existing visceral disease (2,3). Laparoscopy is perhaps the most useful
invasive investigation to exclude gynaecological pathology (4,5) and to assist in the differential diagnosis of
CPP in women (6). Often it is combined with cystoscopy (7,8) and/or proctoscopy to help identify the site of
multi-compartment pain.
Psychological considerations around laparoscopy
There have been three diverse studies of laparoscopy. Elcombe et al. have shown, by comparing waiting time
for laparoscopy, that there was a distinct and lasting improvement in pain consequent on laparoscopy, which
was greater than the gradual improvement without further treatment before or after laparoscopy. Improvement
was related to beliefs about pain and its meaning in terms of serious disease, and not to medical variables (9).
In another study, showing women a photograph of their pelvic contents taken during laparoscopy
during post-laparoscopy feedback did not improve pain ratings or beliefs about pain more than feedback
without a photograph (10).
Peters et al. compared standard clinical care of patients with CPP (where organic causes of pelvic pain
were excluded first and diagnostic laparoscopy was routinely performed, before attention being given to
other causes such as psychological disturbances) with a second group, where an integrated approach was
chosen from the beginning (equal attention was given to somatic, psychological, dietary, environmental, and
physiotherapeutic factors and laparoscopy was not routinely performed) (11). Both groups were similar with
respect to clinical characteristics of the patients and the severity of their pain as assessed by various pain
parameters. Evaluation of the pain 1 year after the institution of treatment revealed that the integrated approach
improved pelvic pain significantly more often than the standard approach for three out of four pain parameters.
Though laparoscopy played no important role in the treatment of pelvic pain it was found to be an essential tool
to rule out any organic cause for the pain. Equal attention to both organic and other causative factors from the
beginning of therapy is more likely to result in a reduction of pelvic pain than just using a standard approach
(11). Pain and function improved somewhat more in the integrated group, but scoring was not standardised
and hard to interpret.

80 UPDATE FEBRUARY 2012
4.4 Pain associated with well-defined conditions
4.4.1 Dysmenorrhoea
Pain in association with menstruation may be primary or secondary. Primary dysmenorrhoea classically
begins at the onset of ovulatory menstrual cycles and tends to decrease following childbirth (6). Secondary
dysmenorrhoea suggests the development of a pathological process and it is essential to exclude
endometriosis (5), adenomyosis (12) and pelvic infection.
Treatment
Reassurance and an explanation of the cause of dysmenorrhoea are usually helpful, together with the use
of simple analgesics, followed by non-steroidal anti-inflammatory drugs (NSAIDs) (13), which are particularly
helpful if they are started before the onset of each menstrual cycle. NSAIDs are effective in dysmenorrhoea,
probably because of their effects on prostaglandin synthetase.
Suppression of ovulation using oral contraceptive tablets (either combined or progesterone only) or the use of
a levo-norgestrol intra-uterine device reduces dysmenorrhoea dramatically in most cases and may be used as
a therapeutic test. As a result of the chronic nature of the condition, potentially addictive analgesics should be
avoided and multidisciplinary pain management strategies, including psychology should be engaged.
4.4.2 Infection
In premenopausal women, a history of pelvic inflammatory disease (PID) must be excluded. Swabs to exclude
infections with organisms such as chlamydia and gonorrhoea, as well as vaginal and genital tract pathogens
(14), should be taken. Patients’ sexual contacts need to be traced in all cases with a positive culture. If there is
any doubt about the diagnosis, laparoscopy may be helpful.
Pelvic inflammatory disease can cause the same clinical findings as endometriosis and can lead to a chronic
pain state. Although PID often has a bacterial origin, viral infections such as primary herpes simplex infection
need to be excluded because they also present with severe pelvic/vaginal/vulvar pain (15). They are usually
associated with ulcerating lesions and inflammation, which may lead to urinary retention (16). Hospitalisation
and opiates may be needed to achieve adequate analgesia.
Treatment
Treatment of infection depends on the causative organisms. Subclinical chlamydial infection may lead to tubal
pathology, which can result in subfertility in the future. Thus, screening for this organism in sexually active
young women is essential to prevent this complication. Standard broad-spectrum antibiotics targeting Gram-
positive and negative organisms are normally recommended. Chronic PID is no longer common in developed
countries, but still poses a significant problem for women in developing countries.
4.4.3 Endometriosis and adenomyosis
The incidence of endometriosis is rising in the developed world. The precise aetiology is still a source of
debate, but an association with nulliparity is well known.
A diagnosis is usually made when a history of secondary dysmenorrhoea and often dyspareunia exists. On
examination, there is often tenderness in the lateral vaginal fornices, reduced uterine mobility, tenderness in the
recto-vaginal septum, and on occasion, adnexal masses. Laparoscopy is the most useful diagnostic tool (17-
19).
Endometriotic lesions affecting the urinary bladder or causing ureteric obstructions can occur, as well as
lesions affecting the bowel, which may lead to rectal bleeding in association with menstruation.
Adenomyosis is associated with augmented pain during menses. It is diagnosed by an ultrasound scan of the
uterus, which often shows cystic dilatation of the myometrium (20).
Treatment
As in primary dysmenorrhoea, analgesics and NSAIDs are helpful in easing pain at the time of menstruation.
Hormone treatment with progestogens or the oral contraceptive pill may halt progress of endometriosis, but is
not curative. A temporary respite may be obtained by using luteinising hormone releasing hormone analogues
to create an artificial menopause, although the resulting oestrogen deficiency does have marked long-term
side effects, such as reduced bone density and osteoporosis. Thus, these drugs are normally only used before
surgery to improve surgical outcome and reduce surgical complications in patients with endometriosis. Surgery
for endometriosis is challenging and the extensive removal of all endometriotic lesions is often thought to be
essential. This is still considered to be controversial, as there is at least one RCT showing no benefit in pain
relief in the removal of early endometriosis compared to sham surgery (21,22). Nevertheless, the best results
are achieved laparoscopically, by highly trained and skilled laparoscopic surgeons, in specialist centres (19,23).
A multidisciplinary team is required for the treatment of extensive disease, including a pain management team.
The pain associated with endometriosis is often not proportionate to the extent of the condition and, even after

UPDATE FEBRUARY 2012 81
extensive removal of the lesions and suppression of the condition, the pain may continue. In this situation,
multidisciplinary pain management strategies, including psychology, should be engaged.
In patients with adenomyosis, there is no curative surgery other than hysterectomy but patients can benefit
from hormonal therapy (oral or levo-norgestrol containing intra-uterine devices) and analgesics as outlined
above.
4.4.4 Gynaecological malignancy
The spread of gynaecological malignancy of the cervix, uterine body or ovary will cause pelvic pain depending
on the site of spread. Treatment is of the primary condition, but all physicians dealing with pelvic pain must be
fully aware of the possibility of gynaecological malignancy.
4.4.5 Injuries related to childbirth
Tissue trauma and soft tissue injuries occurring at the time of childbirth may lead to CPP related to the site of
injury. Dyspareunia is a common problem leading to long-term difficulties with intercourse and female sexual
dysfunction (24). This is often due to transient oestrogen deficiency, commonly seen in the postpartum period
and during breastfeeding. Denervation of the pelvic floor with re-innervation may also lead to dysfunction and
pain.
Treatment
Treatment with a short course of hormone replacement cream can be therapeutically beneficial. However, often
reassurance that the situation will improve on the cessation of breastfeeding is also helpful.
4.4.6 Pain associated with pelvic organ prolapse and prolapse surgery
Pelvic organ prolapse is often an asymptomatic condition, unless it is so marked that it causes back strain,
vaginal pain and skin excoriation (25). Prolapse is often a disease of older women, and it is often associated
with postmenopausal oestrogen deficiency, which may lead to pain associated with intercourse. Hormone
replacement therapy is usually helpful in this circumstance. However, in severe cases associated with a
“dragging pain”, the only options are specially designed supportive plastic vaginal devices or surgery.
In the past few years, pelvic organ prolapse surgery has gained a new dimension. Most tissue surgery is now
augmented by the use of non-absorbable mesh (usually in the form of “mesh kits”) (26-28). Although they may
have a role in supporting the vagina, they are also associated with several complications including bladder,
bowel and vaginal trauma (27). In a subset of these patients, chronic pain may ensue, because mesh insertion
may cause nerve and muscle irritation (23,24).
Clinical evaluation
It is essential that patients are fully evaluated clinically. They may also benefit from specialised imaging, using
contrast mediums if necessary, to identify problematic areas. Most patients can be treated by mesh-excisional
surgery (29,30), if appropriate, or multidisciplinary pain management strategies, including psychology, should
surgery not be relevant.
4.5 Vaginal and vulvar pain syndromes
Pain in the vagina or the female external genital organs (the vulva, which includes the labia, clitoris, and
entrance to the vagina) is most commonly due to infection or trauma. The latter is usually as a consequence of
childbirth or surgery. Pain is usually a precedent to dyspareunia.
When the pain persists for > 6 months, it can be diagnosed as “vulvodynia” or “chronic vaginal/vulvar pain
syndrome” with no known cause. It is still a poorly understood condition and often many doctors do not
recognise it as a real pain syndrome. Many women feel isolated because it remains a difficult condition to treat.
There are two main subtypes of vulvodynia: generalised vulvodynia, where the pain occurs in different areas
of the vulva at different times; and vulvar vestibulitis, where the pain is at the entrance of the vagina. In
generalised vulvodynia, the pain may be constant or occur occasionally, but touch or pressure does not initiate
it, although it may make the pain worse. In vulvar vestibulitis, the pain is described as a burning sensation that
comes on only after touch or pressure, such as during intercourse.
The causes of vulvodynia are many and include:
• Historyofsexualabuse
• Historyofchronicantibioticuse
• Hypersensitivitytoyeastinfections,allergiestochemicalsorothersubstances
• Abnormalinflammatoryresponse(geneticandnon-genetic)toinfectionandtrauma,
• Nerveormuscleinjuryorirritation
• Hormonalchanges
Although therapeutic options remain limited and require a multidisciplinary pain management approach, with
82 UPDATE FEBRUARY 2012
psychological and physiotherapy input, they can be treated effectively with physiotherapy, stretching exercises
and even botulinum toxin, though in the case of the latter the evidence is variable.
Psychological treatment of chronic vulvar pain
There are few published accounts of psychological treatment for chronic vulvar pain, distinct from provoked
vulvar pain (also known as vulvar vestibulitis, provoked vestibulodynia, or dyspareunia).
Three reviews in the past decade, all of provoked as well as chronic vulvar pain, have acknowledged the lack
of understanding of aetiology and maintenance of this problem, and emphasise different components of what
is known.
Damsted-Peterson et al. have described peripheral and central nervous system changes most consistent with
models of chronic pain, as well as local inflammation and pelvic floor tension, and recommend multimodal
treatment (31).
Lotery et al. have focused on local factors, and recommend education, support, and counselling, but provide
no evidence to support these (32). Nanke & Rief have described interaction of physiological, psychological and
interpersonal factors, and recommend biofeedback on the basis of uncontrolled studies (33).
The only RCT found has compared cognitive behavioural therapy (CBT), adapted for vulvar pain from a
previously published model, with supportive psychotherapy, for a mixed population of women with provoked
and chronic vulvar pain (34). CBT consists of behavioural therapy (for sexual problems, increasing general
activity, and pain control), relaxation, and cognitive coping skills. Supportive psychotherapy, also for 10 one
hour sessions, involves non-directive talking therapy by an accepting and reflective therapist. Follow-up to 1
year has shown that ~40% of patients with both conditions achieve at least 33% (clinically significant) pain
relief, with improvement in sexual and emotional function; CBT shows superiority in some outcomes.
4.6 Summary
Pain in association with urinary and gastrointestinal symptoms must be considered carefully. For example,
patients with bladder pain quite often present with dyspareunia due to bladder base tenderness, so though
the dyspareunia may be the focus it is the bladder component that is the main problem. Similarly, in those with
anal pain it may be the evacuatory dysfunction that is the main culprit. Conditions, such as pelvic congestion
has been cited as a cause of pelvic pain of unknown aetiology, but this diagnosis is not universally recognised
(15,16).
It is only when all the above conditions have been excluded that the physician may declare that the patient has
‘unexplained’ pelvic pain. Treating these patients remains a challenge for all physicians but quite clearly the
best results are obtained from a multidisciplinary approach that considers all possible causes.
4.6.1 Conclusions and recommendations: gynaecological aspects of chronic pelvic pain
Clinical state LE
Clinical history and examination
Mandatory to making a diagnosis 2a
Investigations
Mandatory to making a diagnosis 2a
Laparoscopy is well tolerated and does not
appear to have negative psychological effects
1b
Pain associated with well-defined conditions
Dysmenorrhoea: effective therapeutic options 3
Infection: effective therapeutic option 3
Endometriosis: effective therapeutic options
including medical and surgical care
1b
Gynaecological malignancy: effective therapeutic
options
3
Injuries related to childbirth: effective therapeutic
options
3
Pain associated with pelvic organ prolapse:
effective therapeutic options
3
Vaginal and vulvar pain syndrome
Diagnosis and therapeutic interventions 3
Psychological treatment (CBT or supportive
psychotherapy) can improve pain and sexual and
emotional function
1b

UPDATE FEBRUARY 2012 83
Recommendations GR
All women with pelvic pain should have a full gynaecological history and evaluation, and including
laparoscopy is recommended to rule out a treatable cause (e.g. endometriosis).
A
Provide therapeutic options such as hormonal therapy or surgery in well-defined disease states. B
Provide a multidisciplinary approach to pain management in persistent disease states. B
Recommend psychological treatment for refractory chronic vulvar pain. B
Use alternative therapies in the treatment of chronic gynaecological pelvic pain. C
Figure 10: assessment and treatment gynaecological aspects in chronic pelvic pain
4.7 References
1. Newham AP, van der Spuy ZM, Nugent F. Laparoscopic findings in women with chronic pelvic pain. S
Afr Med J. 1996 Sep;86(9 Suppl):1200-3.
http://www.ncbi.nlm.nih.gov/pubmed/9180785
2. Jarrell J, Giamberardino MA, Robert M. Bedside tests of viscera-somatic pain. J Obstet Gynaecol Can
2011 (submitted).
3. Jarrell J. Demonstration of cutaneous allodynia in association with chronic pelvic pain. J Vis Exp. 2009
Jun 23;(28).
http://www.ncbi.nlm.nih.gov/pubmed/19550406
4. Howard FM. The role of laparoscopy as a diagnostic tool in chronic pelvic pain. Baillieres Best Pract
Res Clin Obstet Gynaecol. 2000 Jun;14(3):467-94.
http://www.ncbi.nlm.nih.gov/pubmed/10962637
5. Jacobson TZ, Duffy JM, Barlow D, et al. Laparoscopic surgery for pelvic pain associated with
endometriosis. Cochrane Database Syst Rev. 2009 Oct 7;(4):CD001300.
http://www.ncbi.nlm.nih.gov/pubmed/19821276
6. Porpora MG, Gomel V. The role of laparoscopy in the management of pelvic pain in women of
reproductive age. Fertil Steril. 1997 Nov;68(5):765-79.
http://www.ncbi.nlm.nih.gov/pubmed/9389799
7. Wyndaele JJ, Van Dyck, J, Toussaint N. Cystoscopy and bladder biopsies in patients with bladder
pain syndrome carried out following ESSIC guidelines. Scand J Urol Nephrol. 2009;43(6):471-5.
http://www.ncbi.nlm.nih.gov/pubmed/19707951
8. Seracchioli R, Mannini D, Colombo FM, et al. Cystoscopy-assisted laparoscopic resection of
extramucosal bladder endometriosis. J Endourol. 2002 Nov;16(9):663-6.
http://www.ncbi.nlm.nih.gov/pubmed/12490020
9. Elcombe S, Gath D, Day A. The psychological effects of laparoscopy on women with chronic pelvic
pain. Psychol Med. 1997 Sep;27(5):1041-50.
http://www.ncbi.nlm.nih.gov/pubmed/9300510
10. Onwude JL, Thornton JG, Morley S, et al. A randomised trial of photographic reinforcement during
postoperative counselling after diagnostic laparoscopy for pelvic pain. Eur J Obstet Gynecol Reprod
Biol. 2004 Jan 15;112(1):89-94.
http://www.ncbi.nlm.nih.gov/pubmed/14687747
11. Peters AA, van Dorst E, Jellis B, et al. A randomized clinical trial to compare two different approaches
in women with chronic pelvic pain. Obstet Gynecol. 1991 May;77(5):740-4.
http://www.ncbi.nlm.nih.gov/pubmed/1826544
12. Wassong C, Shah B, Kanayama M, et al. Radiologic findings of pelvic venous congestion in an
adolescent girl with angiographic confirmation and interventional treatment. Pediatr Radiol. 2011 Sep
13.
http://www.ncbi.nlm.nih.gov/pubmed/21912968
Gynaecological
examination
Ultrasound
Laparoscopy (see
text)
Assessment
Grade A recommended
Treatment
Grade B recommended
Laparoscopy to rule out treatable causes
Hormonal therapy in well defined states
Multidisciplinary approach in persistent disease states
Psychological treatment for refractory chronic vulvar pain

84 UPDATE FEBRUARY 2012
13. Allen C, Hopewell S, Prentice A, et al. Nonsteroidal anti-inflammatory drugs for pain in women with
endometriosis. Cochrane Database Syst Rev. 2009 Apr 15;(2):CD004753.
http://www.ncbi.nlm.nih.gov/pubmed/19370608
14. Ness RB, Soper DE, Holley RL, et al. Effectiveness of inpatient and outpatient treatment strategies for
women with pelvic inflammatory disease: results from the Pelvic Inflammatory Disease Evaluation and
Clinical Health (PEACH) Randomized Trial. Am J Obstet Gynecol. 2002 May;186(5):929-37.
http://www.ncbi.nlm.nih.gov/pubmed/12015517
15. Corey L, Adams HG, Brown ZA, et al. Genital herpes simplex virus infections: clinical manifestations,
course, and complications. Ann Intern Med. 1983 Jun;98(6):958-72.
http://www.ncbi.nlm.nih.gov/pubmed/6344712
16. Young H, Moyes A, McMillan A, et al. Screening for treponemal infection by a new enzyme
immunoassay. Genitourin Med. 1989 Apr;65(2):72-8.
http://www.ncbi.nlm.nih.gov/pubmed/2666302
17. Fauconnier A, Chapron C, Dubuisson JB, et al. Relation between pain symptoms and the anatomic
location of deep infiltrating endometriosis. Fertil Steril. 2002 Oct;78(4):719-26.
http://www.ncbi.nlm.nih.gov/pubmed/12372446
18. Vercellini P, Crosignani PG, Abbiati A, et al. The effect of surgery for symptomatic endometriosis: the
other side of the story. Hum Reprod Update. 2009 Mar-Apr;15(2):177-88.
http://www.ncbi.nlm.nih.gov/pubmed/19136455
19. Vercellini P, Crosignani PG, Somigliana E, et al. Medical treatment for rectovaginal endometriosis:
what is the evidence? Hum Reprod. 2009 Oct;24(10):2504-14.
http://www.ncbi.nlm.nih.gov/pubmed/19574277
20. Kaminski P, Gajewska M, Wielgos M, et al. The usefulness of laparoscopy and hysteroscopy in the
diagnostics and treatment of infertility. Neuro Endocrinol Lett. 2006 Dec;27(6):813-7.
http://www.ncbi.nlm.nih.gov/pubmed/17187014
21. Jarrell J, Mohindra R, Ross S, et al. Laparoscopy and reported pain among patients with
endometriosis. J Obstet Gynaecol Can. 2005 May;27(5):477-85.
http://www.ncbi.nlm.nih.gov/pubmed/16100643
22. Jarrell J, Brant R, Leung W, et al. Women’s Pain Experience Predicts Future Surgery for Pain
Associated With Endometriosis. J Obstet Gynaecol Can. 2007 Dec;29(12):988-91.
http://www.ncbi.nlm.nih.gov/pubmed/18053384
23. Daniels J, Gray R, Hills RK, et al. Laparoscopic uterosacral nerve ablation for alleviating chronic pelvic
pain: a randomized controlled trial. JAMA. 2009 Sep 2;302(9):955-61.
http://www.ncbi.nlm.nih.gov/pubmed/19724042
24. Hay-Smith EJ. Therapeutic ultrasound for postpartum perineal pain and dyspareunia. Cochrane
Database Syst Rev. 2000;(2):CD000495.
http://www.ncbi.nlm.nih.gov/pubmed/10796210
25. Roovers JP, van der vaart CH, van der Blom JG, et al. A randomised controlled trial comparing
abdominal and vaginal prolapse surgery: effects on urogenital function. BJOG. 2004 Jan;111(1):50-6.
http://www.ncbi.nlm.nih.gov/pubmed/14687052
26. Withagen MI, Vierhout ME, Hendriks JC, et al. Risk factors for exposure, pain, and dyspareunia after
tension-free vaginal mesh procedure. Obstet Gynecol. 2011 Sep;118(3):629-36.
http://www.ncbi.nlm.nih.gov/pubmed/21860293
27. Niro J, Philippe AC, Jaffeux P, et al. [Postoperative pain after transvaginal repair of pelvic organ
prolapse with or without mesh]. Gynecol Obstet Fertil. 2010 Nov;38(11):648-52.
http://www.ncbi.nlm.nih.gov/pubmed/21030280
28. Lin LL, Haessler Al, Ho MH, et al. Dyspareunia and chronic pelvic pain after polypropylene mesh
augmentation for transvaginal repair of anterior vaginal wall prolapse. Int Urogynecol J Pelvic Floor
Dysfunct. 2007 Jun;18(6):675-8.
http://www.ncbi.nlm.nih.gov/pubmed/16988779
29. Walid MS, Heaton RL. Laparoscopic apical mesh excision for deep dyspareunia caused by mesh
banding in the vaginal apex. Arch Gynecol Obstet. 2009 Sep;280(3):347-50.
http://www.ncbi.nlm.nih.gov/pubmed/19127368
30. Margulies RU, Lewicky_Gaupp C, Fenner DE, et al. Complications requiring reoperation following
vaginal mesh kit procedures for prolapse. Am J Obstet Gynecol. 2008 Dec;199(6):678.e1-4.
http://www.ncbi.nlm.nih.gov/pubmed/18845282
31. Damstedt-Petersen C, Boyer SC, et al. Current perspectives in vulvodynia. Womens Health (Lond
Engl). 2009 Jul;5(4):423-36.
http://www.ncbi.nlm.nih.gov/pubmed/19586434

UPDATE FEBRUARY 2012 85
32. Lotery HE, McClure N, Galask RP. Vulvodynia. Lancet. 2004 Mar 27;363(9414):1058-60.
http://www.ncbi.nlm.nih.gov/pubmed/15065562
33. Nanke A, R. W. (2004). Biofeedback in somatoform disorders and related syndromes. Current Opinion
in Psychiatry 17: 133-138.
34. Masheb RM, Kerns RD, Lozano C, et al. A randomized clinical trial for women with vulvodynia:
Cognitive-behavioral therapy vs. supportive psychotherapy. Pain. 2009 Jan;141(1-2):31-40.
http://www.ncbi.nlm.nih.gov/pubmed/19022580
5. GASTROINTESTINAL ASPECTS OF CHRONIC
PELVIC PAIN
5.1 Introduction
This chapter describes CPP perceived to be associated with the gastrointestinal tract, which is mainly due to
functional disorders and cannot be explained by structural or specific well-defined diseases of the pelvis.
Some points to note:
• Theremaybeaconsiderableoverlapofthegastrointestinalwithotherpelvicpainsyndromes.
• Definedgastrointestinalconditionswithspecificstructuraldefectsanddiseasesmaycoexist.
Behavioural changes such as straining can lead to organic diseases such as rectal prolapse, solitary
rectal ulcer syndrome, or pudendal nerve injury with consecutive faecal incontinence.
• Somestructuralgastrointestinalabnormalities(e.g.,postpartumanalsphincterdefects,orsmall
rectoceles) are often observed in asymptomatic individuals and may be coincidental with the
gastrointestinal pelvic pain syndrome.
• Differentdiseasescanaggravatepreviouslyasymptomaticfunctionaldisorderswhichmaybecome
symptomatic such as faecal incontinence in patients with diarrhoea of different origins or anal fissure
in patients with dyssynergic defecation.
• Finally,weneedtoconsiderthatallfunctionaldisorderssuchasanorectalpainaredefinedonthe
basis of retrospectively evaluated longstanding symptoms, which ideally would have been registered
prospectively with symptom diaries (1,2).
5.2 Clinical history
Functional anorectal disorders are diagnosed by symptoms, supplemented by objective findings. The
predominant symptoms patients are interviewed about are discomfort or pain in relation to their bowel
habits, daily activities, and eating. A precise history of dysfunctional voiding or defecation should be asked,
ideally applying symptom questionnaires for urinary and anorectal symptoms (e.g., Rome III questionnaire
for anorectal pain). Excessive straining at most defecations, anal digitations in dyssynergic defecation, and a
sensation of anal blockage may be found in patients with chronic anal pain. History of anxiety and depression
with impaired QoL is often encountered in anorectal functional disorders and should be evaluated.
5.2.1 Clinical examination and investigations
At clinical examination, perianal dermatitis may be found as a sign of faecal incontinence or diarrhoea.
Fissures may be easily overlooked and should be searched thoroughly in patients with anal pain. Rectal digital
examination findings may show high or low anal sphincter resting pressure, a tender puborectalis muscle in
patients with the levator ani syndrome, and occasionally increased perineal descent. The tenderness during
posterior traction on the puborectalis muscle differentiates between “highly likely” and “possible” levator ani
syndrome and is used in most studies as the main inclusion criterion. Dyssynergic (paradoxical) contraction of
the pelvic muscles when instructed to strain during defecation is a frequent finding in patients with pelvic pain.
Attention should be paid to anal or rectal prolapse at straining, and ideally during bimanual examination by the
gynaecologist to diagnose an enterocele or cystocele.
5.2.2 Diagnostic assessment
The Rome III criteria for diagnosis of functional anorectal diseases include symptoms for each specific
functional disorder as listed below. The gastrointestinal diagnostic assessment should be performed in an
interdisciplinary manner, preferably at a pelvic floor centre by a dedicated team and appropriate testing. The
most frequently performed investigations are flexible rectosigmoidoscopy or colonoscopy, pelvic ultrasound,
anorectal endosonography and anorectal manometry combined with anal EMG and balloon expulsion test.

86 UPDATE FEBRUARY 2012
Three-dimensional anorectal ultrasound has become an indispensable readily available tool for the specialised
proctologist. Perineal ultrasound offers the advantage of sphincter imaging without insertion of the transducer
into the rectum. MRI in conjunction with MR defecography has become the most valuable imaging technique
to assess anorectal function dynamically. MRI studies outline simultaneously the anatomy of the pelvic floor
and allow us to visualise different structural and functional pathologies, by applying dynamic sequences
after filling of the rectum with a viscous contrast medium (e.g., ultrasound gel). The following pathologies
can be visualised: pelvic floor descent, an abnormal anorectal angle while squeezing and straining, rectal
intussusception, rectocele, enterocele and cystocele. However, limitations of MR defecography are the left
lateral position and the limited space for the patient, which may reduce the ability to strain and hereby reduce
the sensitivity of the method, underestimating the size of entero-and rectoceles as well as the amount of
intussusception. Surgical consultations should be available for all patients, plus referral to an urogynaecologist
or urologist when indicated. Biofeedback treatment, botulinum toxin injection, and percutaneous tibial nerve
and sacral nerve stimulation should be available as a complementary therapeutic option to medical and
surgical treatment.
5.3 Pain associated with well-defined conditions
5.3.1 Haemorrhoids
CPP is rare in haemorrhoidal disease because endoscopic and surgical treatment is mostly effective in acute
disease. The most frequent aetiology of pain without significant bleeding is thrombosed external haemorrhoids
or an anal fissure. Haemorrhoidal pain on defecation associated with bleeding is usually due to prolapsed or
ulceration of internal haemorrhoids. Anaemia from haemorrhoidal bleeding is rare but may arise in patients
on anticoagulation therapy, or those with clotting disorders. Different treatments of haemorrhoids have been
evaluated by two systematic Cochrane reviews. Excisional haemorrhoidectomy (EH) has been compared to
the less-invasive technique of rubber band ligation (RBL), and has been shown to increase pain, with more
complications and time off work. However, despite these disadvantages of EH, complete long-term cure of
symptoms is increased by surgery, and minor complications are accepted by patients. RBL is the choice of
treatment for grade II haemorrhoids, whereas EH should be reserved for grade III haemorrhoids or recurrence
after RBL (3). New stapler techniques of haemorrhoidopexy are associated with a higher long-term risk of
recurrence and prolapse compared to conventional EH. Further studies are needed (4).
5.3.2 Anal fissure
Anal fissures are tears in the distal anal canal and induce pain during and after defecation. The pain can last for
several minutes to hours. Persistence of symptoms beyond 6 weeks or visible transversal anal sphincter fibres
define chronicity. Fissures located off the midline are often associated with specific diseases such as Crohn’s
disease or anal cancer. Internal anal sphincter spasms and ischaemia are associated with chronic fissures.
Medical therapy with nitrates and calcium channel blockers resulting in sphincter relaxation is effective (5).
Botulinum A toxin injection is indicated for fissures that are refractory to topical nitrates. Surgery with lateral
internal sphincterotomy is the most studied procedure but carries the risk of postoperative faecal incontinence,
and may be replaced by fissure excision combined with botulinum toxin or anal advancement flap.
5.3.3 Proctitis
Abdominal and pelvic pain in patients with inflammatory bowel disease and proctitis are often difficult to
interpret. Faecal calprotectin may help to differentiate between inflammation and functional pain, to spare
steroids. Tricyclic antidepressants at low dose can be effective in this situation when acute exacerbation has
been ruled out (6,7).
5.3.4 Constipation
Constipation is usually not associated with CPP but is often associated and may induce increased pelvic
discomfort and psychological distress. Dyssynergic defecation is the most common aetiology and responsible
for 50% of causes of constipation. Dyssynergia describes an overactivity of pelvic floor muscles during
defecation and the partial or complete inability to relax voluntarily pelvic floor muscles. Stool diaries and
physiological testing followed by biofeedback treatment when indicated have been established as standard
care in randomised controlled trials (8).
5.4 Chronic anal pain syndrome
5.4.1 Diagnostic criteria for chronic anal pain syndrome (chronic proctalgia) according to the Rome III
criteria are as follows and must include all of the following:
1. Chronic or recurrent rectal pain or aching.
2. Episodes last at least 20 min.
3. Exclusion of other causes of rectal pain such as ischaemia, inflammatory bowel disease, cryptitis,
intramuscular abscess and fissure, haemorrhoids, prostatitis, and coccygodynia.

UPDATE FEBRUARY 2012 87
These criteria should be fulfilled for the past 3 months with symptom onset at least 6 months before diagnosis
(2).
The chronic anal pain syndrome includes the above diagnostic criteria and exhibits exquisite tenderness
during posterior traction on the puborectalis muscle. This common and debilitating condition is frustrating to
treat. Pathophysiology of pain is thought to be due to overactivity of the pelvic floor muscles. Chiarioni et al.
have recently published an RCT demonstrating that biofeedback treatment was superior to electrogalvanic
stimulation and massage for treatment of the levator ani syndrome. One hundred and fifty-seven patients
who had at least weekly rectal pain were investigated, but only patients with tenderness on traction of the
pelvic floor showed a significant treatment benefit. Eighty-seven percent of patients with tenderness of the
puborectalis muscle (Rome II: Highly likely Levator Ani Syndrome) reported adequate relief after one month of
biofeedback versus 45% for electrogalvanic stimulation, and 22% for massage. These results were maintained
at 12 months with adequate relief after nine sessions of biofeedback in 58% of the whole group (Rome II:
Highly likely and Possible Levator Ani Syndrome), after galvanic stimulation in 27% and massage in 21% of
patients. As previously described in dyssynergic defecation, the ability to expel a 50-ml water-filled balloon
and to relax pelvic floor muscles after biofeedback treatment were predictive of a favourable therapeutic
outcome (9). The pathophysiology of the chronic anal pain syndrome is therefore similar to that of dyssynergic
defecation, and this favours the role of the pelvic floor muscles in the pathophysiology of both conditions.
Other treatment modalities have been less successful.
5.4.2 Botulinum toxin in pelvic pain
Chronic pelvic pain associated with spasm of the levator ani muscles and treatment of the puborectalis and
pubococcygeus muscle by botulinum toxin appears to be promising in some women, as shown in a pilot
study (n = 12). The inclusion criteria were dependent only on vaginal manometry with overactivity of the pelvic
floor muscles, defined as a vaginal resting pressure > 40 cm H
2
O. Although dyspareunia and dysmenorrhoea
improved, non-menstrual pelvic pain scores were not significantly ameliorated (10). In the following double-
blinded, randomised, placebo-controlled trial, the same group defined pelvic floor myalgia according to the
two criteria of tenderness on contraction and hypertension (> 40 cm H
2
O) and included 60 women. In this
larger study, non-menstrual pelvic pain was significantly improved compared to that treated with placebo (VAS
score 51 vs. 22; P = 0.009). It was concluded therefore that botulinum toxin is effective for reducing pelvic-
floor-muscle associated pain with acceptable adverse effects such as occasional urinary and faecal stress
incontinence (11).
However, recently, a small RCT failed to show any benefit of botulinum toxin, and sacral nerve stimulation has
been reported to be somewhat beneficial in an uncontrolled study, showing improvement in less than half the
patients (12,13).
5.4.3 Intermittent chronic anal pain syndrome (proctalgia fugax) consists of all the following
diagnostic criteria, which should be fulfilled for 3 months and before 3 months:
1. Recurrent episodes of pain localised to the anus or lower rectum
2. Episodes last from several seconds to minutes
3. There is no anorectal pain between episodes.
Stressful life events or anxiety may precede the onset of the intermittent chronic anal pain syndrome. The
attacks may last from a few seconds to as long as 30 min. The pain may be cramping, aching or stabbing and
may become unbearable. However, most patients do not report it to their physicians and pain attacks occur
less than five times a year in 51% of patients. Due to the short duration of the episodes, medical treatment
and prevention is often not feasible. Inhaled beta-2 adrenergic agonist salbutamol was effective in an RCT in
patients with frequent symptoms and shortened pain duration (14). Other treatment options are topic diltiazem
and botulinum toxin (15). However, there is still some controversy as regards the duration of pain of intermittent
chronic and chronic anal pain syndrome and RCTs do often use different definitions extending the pain
duration in order to better evaluate the study-drug action.
5.5 Summary
Chronic pelvic pain is an interdisciplinary entity needing multispecialty and multidisciplinary diagnostic
assessment by gastroenterology, urology, gynaecology and pain teams as appropriate, with the input of
physicians, psychologists and physiotherapists amongst others. Anorectal pain is investigated best by
endoscopic and functional testing to rule out structural disease that can be treated specifically. CPP due to
functional disorders remains a therapeutic challenge that may respond to biofeedback therapy, electrogalvanic
syndrome and botulinum toxin in the case of levator ani syndrome and defecatory defects associated with
pelvic pain.

88 UPDATE FEBRUARY 2012
5.5.1 Conclusions and recommendations: anorectal pain syndrome
Conclusions on functional anorectal pain. LE
Tenderness on traction is the main criterion of the chronic anal pain syndrome. 1a
Biofeedback is the preferred treatment for the chronic anal pain syndrome. 1a
Electrogalvanic stimulation is less effective than biofeedback. 1b
Botulinum toxin is efficient in CPP with spasms. 1b
Sacral neurostimulation is effective in pelvic pain. 3
Inhaled salbutamol is effective in intermittent chronic anal pain syndrome. 3
Recommendations for functional anorectal pain GR
Functional testing is recommended in patients with anorectal pain. A
Biofeedback treatment is recommended in patients with pelvic pain and dyssynergic defecation. A
Botulinum toxin in women with pelvic pain and electrogalvanic stimulation can be considered in the
chronic anal pain syndrome.
B
Sacral neuromodulation is recommended in the chronic anal pain syndrome. C
Inhaled salbutamol is recommended in the intermittent chronic anal pain syndrome. C
Figure 11: assessment and treatment algorithm for anorectal pain syndrome
Endoscopy
Pelvic floor muscle
testing
Anorectal
manometry
Rectal balloon
expulsion test
Assessment
Grade A recommended
MRI-defecography
Treatment
Grade B recommended
Other comments
Biofeedback treatment
Botulinum toxine A in women with pelvic pain
Electro-galvanic stimulation
Sacral neuromodulation should be considered
Inhaled salbutamol should be considered in intermittent anal pain
syndrome

UPDATE FEBRUARY 2012 89
Figure 12: diagnosis algorithm for chronic anorectal pain
5.6 References
1. Whitehead WE, Bharucha AE. Diagnosis and treatment of pelvic floor disorders: what’s new and what
to do. Gastroenterology. 2010 Apr;138(4):1231-5.
http://www.ncbi.nlm.nih.gov/pubmed/20176023
2. Bharucha AE, Wald A, Enck P, et al. Functional anorectal disorders. Gastroenterology. 2006
Apr;130(5):1510-8.
http://www.ncbi.nlm.nih.gov/pubmed/16678564
3. Shanmugam V, Thaha MA, Rabindranath KS, et al. Rubber band ligation versus excisional
haemorrhoidectomy for haemorrhoids. Cochrane Database Syst Rev. 2005 Jul 20;(3):CD005034.
http://www.ncbi.nlm.nih.gov/pubmed/16034963
4. Jayaraman S, Colquhoun PH, Malthaner RA. Stapled versus conventional surgery for hemorrhoids.
Cochrane Database Syst Rev. 2006 Oct 18;(4):CD005393.
http://www.ncbi.nlm.nih.gov/pubmed/17054255
5. Nelson R. Non surgical therapy for anal fissure. Cochrane Database Syst Rev. 2003;(4):CD003431.
http://www.ncbi.nlm.nih.gov/pubmed/14583976
6. Keohane J, O’Mahony C, O’Mahony L, et al. Irritable bowel syndrome-type symptoms in patients
with inflammatory bowel disease: a real association or reflection of occult inflammation? Am J
Gastroenterol. 2010 Aug;105(8):1788.
http://www.ncbi.nlm.nih.gov/pubmed/20389294
7. Halpert A, Dalton CB, Diamant NE, et al. Clinical response to tricyclic antidepressants in functional
bowel disorders is not related to dosage. Am J Gastroenterol. 2005;100:664–71.
http://www.ncbi.nlm.nih.gov/pubmed/15743366
8. Rao SS, Valestin J, Brown CK, et al. Long-term efficacy of biofeedback therapy for dyssynergic
defecation: randomized controlled trial. Am J Gastroenterol. 2010 Apr;105(4):890-6.
http://www.ncbi.nlm.nih.gov/pubmed/20179692
9. Chiarioni G, Nardo A, Vantini I, et al. Biofeedback is superior to electrogalvanic stimulation and
massage for treatment of levator ani syndrome. Gastroenterology. 2010 Apr;138(4):1321-9.
http://www.ncbi.nlm.nih.gov/pubmed/20044997
Endoscopy normal
Tenderness of puborectalis muscle
yes
* Anorectal manometry
* Balloon expulsion test
* MRI-Defecography
Anorectal pain syndrome
Specific disease guidelines
* Biofeedback
* Electro stimulation
Chronic anorectal pain
no
yes no
Refer to specialist
pain management unit
yes no
Dysfunction present

90 UPDATE FEBRUARY 2012
10. Jarvis Sk, Abbott JA, Lenart MB, et al. Pilot study of botulinum toxin type A in the treatment of chronic
pelvic pain associated with spasm of the levator ani muscles. Aust N Z J Obstet Gynaecol. 2004
Feb;44(1):46-50.
http://www.ncbi.nlm.nih.gov/pubmed/15089868
11. Abbott JA, Jarvis SK, Lyons SD, et al. Botulinum toxin type A for chronic pain and pelvic floor spasm
in women: a randomized controlled trial. Obstet Gynecol. 2006 Oct;108(4):915-23.
http://www.ncbi.nlm.nih.gov/pubmed/17012454
12. Rao SS, Paulson J, Mata M, et al. Clinical trial: effects of botulinum toxin on levator ani syndrome—a
double-blind, placebo controlled study. Aliment Pharmacol Ther. 2009 May 1;29(9):985-91.
http://www.ncbi.nlm.nih.gov/pubmed/19222415
13. Falletto E, Masin A, Lolli P, et al. Is sacral nerve stimulation an effective treatment for chronic
idiopathic anal pain? Dis Colon Rectum. 2009 Mar;52(3):456-62.
http://www.ncbi.nlm.nih.gov/pubmed/19333046
14. Eckardt VF, Dodt O, Kanzler G, et al. Treatment of proctalgia fugax with salbutamol inhalation. Am J
Gastroenterol. 1996 Apr;91(4):686-9.
http://www.ncbi.nlm.nih.gov/pubmed/8677929
15. Atkin GK, Suliman A, Vaizey CJ. Patient characteristics and treatment outcome in functional anorectal
pain. Dis Colon Rectum. 2011 Jul;54(7):870-5
http://www.ncbi.nlm.nih.gov/pubmed/21654255
6. PERIPHERAL NERVE PAIN SYNDROMES
6.1 Neuropathic pain
Much has been written on the subject of peripheral neuropathic pain (1-4) including its diagnosis and
treatment. There are some fundamental principles that are worth considering:
1. Nerve injury is associated with changes both within the peripheral nervous system (PNS) and the
central neural axis including the higher centres. These changes serve to produce an increasing
disparity between stimulus and response (Chapter 2).
2. In the PNS, nerve damage may produce a neuroma that can provide a source of ongoing afferent
central activity. The neuroma may be discreet and palpable to touch or en-passage and not palpable.
Neuromas are sensitive and respond to: compression (e.g., by the surrounding tissue or digital
pressure), temperature change and adrenergic stimulation. Sympathetic nerve fibres can grow into
neuromas as well as the associated dorsal root ganglia, which may result in sensitivity to body
adrenaline changes such as through mood and environment with subsequent changes in pain.
3. Windup is a progressive increase in centrally elicited action potentials per unit peripheral stimulus.
A severe acute insult or a chronic repeated stimulus may result in a transient windup phenomenon
becoming permanent through immediate gene activation and neurochemical and structural neuronal
changes within the CNS. These long-term changes in central sensitisation are associated with
dysfunction of the afferent sensory nervous system and perception, as well as efferent motor,
vasomotor and pseudomotor activity within the pathways of the injured nerve (5).
4. These central changes may result in abnormal afferent processing for nerves other than those
originally damaged, so that increased perception (pain, allodynia and hyperaesthesia) from an area
greater than the expected pattern may occur. In the case of tissues with innervation that overlaps with
an injured nerve, somatic and visceral hypersensitivity (e.g., sensory urge with increased frequency of
voiding/evacuation) may be perceived from those tissues.
Essentially, what may be considered a simple nerve injury may be magnified by the CNS so that a whole
region may be involved and a non-specific regional pain syndrome may arise. There is also a suggestion
that involvement of both the peripheral and central nervous system in the control of the endocrine and
immunological system may also become abnormal. Certainly, there is a complex interaction between nerve
injury, emotional well being, disability and widespread pain. A proportion of patients go on to develop chronic
fatigue syndrome, fibromyalgia and immunological disorders (6-8).
6.2 Anatomy
When considering pelvic pain mechanisms, nerves associated with the pelvis/genitalia are generally divided
into thoraco-lumbar and sacral root afferents. The hypogastric plexus is mixed autonomic (sympathetic and
parasympathetic) and may contain afferents associated with pain.

UPDATE FEBRUARY 2012 91
6.2.1 The anterior groin nerves
The iliohypogastric nerve arises from L1 and its anterior branch supplies the skin above the pubis; its lateral
cutaneous branch is distributed to the anterolateral part of the buttock.
The ilioinguinal nerve is smaller than the iliohypogastric nerve; it also arises from L1 and is distributed to the
skin of the groin and mons pubis.
The genitofemoral nerve arises from L1 and L2. It passes through the psoas muscle, then down it to emerge
through the deep inguinal ring. Its genital branch supplies the cremaster muscle and a part of the anterior and
lateral scrotum. The femoral branch passes close to the external iliac artery, the deep circumflex iliac artery and
the femoral artery to be distributed to the upper part of the femoral triangle. The two branches of the femoral
branch may separate at any level, therefore, sensory phenomena associated with nerve damage depend upon
the level of the lesion and individual variability.
The lateral cutaneous nerve of the thigh arises from L2 and L3 and eventually leaves the abdomen behind
or through the inguinal ligament at a variable distance medial to the anterior superior iliac spine. In the thigh,
it divides into an anterior branch that supplies the anterolateral skin of the thigh, approximately 10 cm down
from the inguinal ligament to the knee. The posterior branch supplies the skin more laterally from the greater
trochanter, down to the mid-thigh.
The obturator nerve arises from L2-L4, descends through the psoas muscle, runs around the pelvis in close
proximity to the obturator internus muscle and obturator vessels, and leaves the pelvis via the obturator
foramen. This nerve has significant motor innervation, and its cutaneous branch is distributed primarily to the
skin on the medial aspect of the knee.
6.2.2 The posterior subgluteal triangle nerves
The posterior triangle area is the area defined superiorly by the upper border of the piriformis, inferiorly by the
lower border of quadratus femoris, laterally by the greater trochanter and medially by and lateral border of the
sacrum, the lateral borders of the sacrotuberal ligament and ischeal tuberosity. This region contains the sciatic
nerve, posterior femoral cutaneous nerve (which branches into the posterior cutaneous perineal branch and the
cluneal nerves), the nerve to the obturator internus muscle, and the pudendal nerve. These nerves pass deep
to the piriformis muscle and superficial to the superiour gemellus and obturator internus muscles. Injury in this
area may damage one or more of these nerves (Figure 13) (9-15).
6.2.3 Branches of the pudendal nerve
The pudendal nerve has its origins at the S2-S4 levels. S2 and S3 also contribute to the sciatic nerve and S4
to the coccygeal plexus and the annoccoccygeal nerves.
The pudendal nerve has three main branches: the inferior anorectal nerve, the superficial perineal nerve
(which terminates as cutaneous branches in the perineum and posterior aspect of the scrotum), and the deep
perineal nerve, which is distributed to the pelvic structures (innervating parts of the bladder, prostate and
urethra). This branch terminates as the dorsal nerve of the penis/clitoris, which innervates the glans.
In addition to sensory branches, the pudendal nerve provides motor innervation to anal and urethral sphincters,
as well as to the bulbospongiosus and ischiocavernous muscles (involved in the bulbocavernosal response,
orgasm and ejaculation). Autonomic fibres also pass with the pudendal nerve and are derived from the
presacral parasympathetic as well as sympathetic fibres via the hypogastric plexi.
6.2.4 Anatomical relations of the pudendal nerve (Figure 13)
The anatomy may be variable, however, the three roots that form the pudendal nerve usually merge anterior to
the sacrum and inferior to the piriformis muscle.
The pudendal nerve leaves the pelvis via the greater sciatic notch to enter the subgluteal region. In the
posterior subgluteal triangle (the area bordered by the inferior edge of the piriformis muscle, the sarotuberous
ligament medially and the upper border of the rectus femoris muscle inferiorly), the nerve emerges from under
the inferior border of the piriformis muscle with its associated pudendal artery and veins; it is medial to the
nerve innervating the obturator internus muscle, which is medial to the posterior femoral cutaneous nerve
(which divides into its cutaneous branch but also the inferior cluneal nerves and perineal nerves), which is
medial to the sciatic nerve. These anatomical relations are important for neurotracing techniques used for nerve
blocks and because symptoms in those nerve territories also help with diagnosis (16-20).
The pudendal nerve leaves the subgluteal region as it wraps around the superficial surface of the
ischeal spine/sacrospinal ligament to re-enter the pelvis (9,10) via the lesser sciatic notch (between the more
ventral sacrospinal ligament and the more dorsal sacrotuberal ligaments). This occurs 15% of the time at
the enthesis of the spine and the ligament; 75% of the time, it is more medial, and 10% of the time, it wraps
around the spine. The sacrotuberal ligament may have a sharp superior border, be wide, and as a result, close
to the spinosacral ligament, or be divided with the pudendal nerve passing through it. All of these features may

92 UPDATE FEBRUARY 2012
predispose to nerve injury.
As the pudendal nerve re-enters the pelvis below the levator muscles, it runs within a fascial canal medial to
the internal obturator muscle (Alcock’s canal).
The inferior anorectal branch may never be a true branch of the pudendal nerve, and may have its
origins directly from sacral the roots. As a consequence, pain associated with pudendal nerve injury may not
involve the anorectal area. Similarly, pain may only be perceived in the anorectal area if the main pudendal
nerve is not involved. In 11% of cases, the inferior anorectal nerve pierces the sacrospinal ligament, possibly
increasing the risk of entrapment. Other variations of the anorectal branch exist with the nerve branching
off from the main pudendal nerve at any point in the gluteal region or within the pelvis. In 56% of cases, the
pudendal nerve is a single trunk as it re-enters the pelvis. Some people have two or three pudendal nerve
trunks.
Figure 13: Anatomical relations of the pudendal nerve
Source: Drake, Vogel, & Mitchell: GRAY’s ANATOMY FOR STUDENTS, 2004 Elsevier Inc.
6.2.5 Afferent nerves and the genitalia
• Theafferentsfromtheskinofthegenitalspassviaacomplexofmultiplesensorynervesandthis
makes the anatomical diagnosis of nerve injury as a cause of pain difficult.
• Theanterolateralpartofthescrotum/labiamajorahasafferentsassociatedwiththegenitofemoral
nerve primarily; there may also be some involvement of the ilioinguinal and iliohypogastric nerves.
• Theposteriorscrotal/labiabranchesofthepudendalnervetransmitsensationfromtheposterior
scrotum/labia majora.
• Thepenisshaftisinnervatedonitsdorsalsurfacebythegenitofemoral,ilioinguinalandiliohypogastric
nerves, and the ventral surface by the perineal branches of the posterior femoral cutaneous nerve and
cutaneous branches of the pudendal nerve.
• Theglanspenis/clitorisisassociatedwiththedorsalnerveofthepenis/clitoris,theterminalbranchof

UPDATE FEBRUARY 2012 93
the pudendal nerve.
• Allthenervesthatareassociatedwiththescrotummayalsoreceiveafferentsfromthetestes,
although classically, the nerves from the testes are usually associated with the genitofemoral nerve
(thoracolumbar as opposed to sacral roots).
• Thesuperficialbranchesofthepudendal’ssuperficialperinealnerveandtheperinealbranchofthe
posterior femoral cutaneous nerve receive afferents from the perineal skin.
• Deeperafferentsfromtheperineumandfromsomeofthepelvicorganspasstothepudendalnerve
via its deep perineal branch.
6.2.6 Afferents in the autonomic plexus
The pelvic plexus is associated with both the parasympathetic and sympathetic nerves, and as well as
afferents associated with these pathways, afferents may travel back to the sacral and thoracolumbar roots
with these autonomic nerves. Sites for injury and possible intervention may thus include: the ganglion impar,
superior hypogastric plexus, inferior hypogastric plexus, and lumbar sympathetic trunk, as well as more central
spinal root areas.
6.3 Aetiology of nerve damage
6.3.1 Anterior groin nerves - aetiology of nerve damage
The primary afferents of the anterior groin nerves enter the spinal cord at the thoracolumbar level (T10 to L3).
Thoracolumbar spinal pathology and any pathology along the course of the nerve may result in neuropathic
pain in the distribution of these nerves. As well as neoplastic disease, infection and trauma, surgical incisions
and postoperative scarring may result in nerve injury (21-23).
6.3.2 Pudendal neuralgia - aetiology of nerve damage
Anatomical variations
Anatomical variations may predispose the patient to developing pudendal neuralgia over time or with repeated
low-grade trauma (such as sitting for prolonged periods of time or cycling) (9,10).
The pudendal nerve may be damaged due to local anatomical variation at the level of:
1. The piriformis muscle. For example, as part of a piriformis syndrome: in some cases, the nerve may
pass through the muscle and hence be trapped; or in other cases, muscle hypertrophy or spasm is
implicated.
2. The sacrospinal/sacrotuberous ligaments, possibly accounting for 42% of cases.
3. Within Alcock’s canal (medial to the obturator internus muscle, within the fascia of the muscle),
possibly accounting for 26% of cases.
4. Multiple levels in 17% of cases.
The site of injury determines the site of perceived pain and the nature of associated symptoms (e.g., the more
distal the damage, the less likely the anal region will be involved).
6.3.3 Surgery
In orthopaedic hip surgery, pressure from the positioning of the patient, where the perineum is placed hard
against the brace, can result in pudendal nerve damage (24,25). The surgery itself may also directly damage
the nerve. Pelvic surgery such as sacrospinous colpopexy is clearly associated with pudendal nerve damage
in some cases (26,27). In many types of surgery, including colorectal, urological and gynaecological, pudendal
nerve injury may be implicated.
6.3.4 Trauma
Fractures of the sacrum or pelvis may result in pudendal nerve/root damage and pain. Falls and trauma to
the gluteal region may also produce pudendal nerve damage if associated with significant tissue injury or
prolonged pressure.
6.3.5 Cancer
Tumours in the presacral space must be considered. Tumours invading the pudendal nerve may occur and
there may also be damage from surgery for pelvic cancer (13).
6.3.6 Birth Trauma
This is more difficult to be certain about (12). The pudendal neuralgia of birth trauma is thought to resolve in
most cases over a period of months. However, rarely, it appears to continue as painful neuropathy. Multiple
pregnancy and births may predispose to stretch neuropathy in later life.

94 UPDATE FEBRUARY 2012
6.3.7 Elderly women
Child birth (28) and repeated abdominal straining associated with chronic constipation (29) are thought to
predispose elderly women to postmenopausal pelvic floor descent and stretching of the pudendal nerve with
associated pain. Changes in the hormone status may also be a factor.
In the Urogenital Pain Management Centre, the commonest associations with pudendal neuralgia appear to
be: history of pelvic surgery; prolonged sitting (especially young men working with computer technology); and
postmenopausal older women. Trauma- and cancer-related pain is less frequent, cycling where as classical
appears to be rarely seen.
6.4 Diagnosis for pudendal neuralgia
6.4.1 Differential diagnosis of other disorders
Other forms of neuropathic pain (30,31).
As well as the pudendal nerve, there are several other nerves that may mimic the symptoms of pudendal
neuralgia if they are damaged.
Inferior cluneal nerve. This is a branch of the posterior femoral cutaneous nerve. This nerve is prone to injury
in the ischial region. Cluneal nerve injury produces a sensation of pain perceived more laterally than that for
pudendal neuralgia.
Sacral nerve roots. The S2-S4 nerve roots may be involved. This is an important differential diagnosis as
tumours must be excluded.
Cauda equina syndrome. Lumbar spinal pathology involving the cauda equina may result in an intractable
neuropathic pain.
Ilioinguinal, iliohypogastric and genitofemoral nerves. Injury to these nerves or their roots may occur from
thoracolumbar pathology, abdominal posterior wall conditions, surgery, and entrapment in the groin. The
pain may extend into the groin, anterior perineum and scrotum/labia majorum. If the femoral branch of the
genitofemoral nerve is involved, pain may extend into the inner thigh.
Referred spinal pain
Pain from thoracolumbar pathology may refer to the groin. Spinal pain may become associated with muscle
hyperalgesia and trigger points. The muscle associated pain may spread to involve a range of muscles,
including the pelvic floor muscles with resultant pelvic pain.
Musculoskeletal disorders
Trigger points associated with localised tenderness and pain may be detected in the piriformis, obturator
internus, levator ani, bulbocavernosal and ischeocavernosal muscles, as well as the gluteal, adductor, rectus
abdominus and spinal muscles. All of these may refer the pain to or close to the pelvis.
Pathology of the joints (sacroiliac, pubic symphysis, hip and spinal) may also refer into the pelvis.
Coccyx pain syndrome, a painful coccyx may occur for a number of reasons (Chapter 2).
6.4.2 Clinical presentation of pudendal neuralgia
6.4.2.1 Age
There is a wide age range, as one would expect with a condition that has so many potential causes. There is
a suggestion that, the younger the patient, the better the prognosis. Essentially, the sooner the diagnosis is
made, as with any compression nerve injury, the better the prognosis, and older patients may have a more
protracted problem (32-34).
6.4.2.2 Sex
Six out of ten cases are observed in women.
6.4.2.3 History
A proportion of patients will be able to relate the onset of pain to an acute event such as surgery, sepsis or
trauma, and occasionally, cycling for a prolonged period. Chronic injury is more frequent, such as associated
with sitting for prolonged periods over time. Many will be idiopathic.
The pain is classically perceived in the perineum from anus to clitoris/penis. However, less-specific pain
distribution may occur, and this may be due to anatomical variation, involvement of branches of the nerve
rather that the main nerve, CNS central sensitisation, and consequently, the involvement of other organs and
systems in a regional pain syndrome. Other nerves in the vicinity may also be involved, for example, inferior
cluneal nerve and perineal branches of the posterior femoral cutaneous nerve. The musculoskeletal system
may become involved, confusing the pain picture as aches and pains develop in the muscles due to immobility

UPDATE FEBRUARY 2012 95
and disability, possibly magnified by the CNS changes.
Burning is the most predominant adjective used to describe the pain. Crushing and electric may also be used,
indicating the two components - a constant pain often associated with acute sharp episodes. Many patients
may have the feeling of a swelling or foreign body in the rectum or perineum, often described as a golf or
tennis ball. The term pain has different meanings to patients and some would rather use the term discomfort or
numbness.
Aggravating factors include any cause of pressure being applied, either directly to the nerve or indirectly to
other tissue, resulting in pudendal traction. Allodynia is pain on light touch due to involvement of the CNS, and
may make sexual contact and the wearing of clothes difficult. These patients often remain standing, and as a
consequence, develop a wide range of other aches and pains. Soft seats are often less well tolerated, whereas
sitting on a toilet seat is said to be much better tolerated. If unilateral, sitting on one buttock is common. The
pain may be exacerbated by bowel or bladder evacuation.
6.4.2.4 Associated features
Pudendal nerve damage may be associated with a range of sensory phenomena. In the distribution of the
nerve itself, as well as unprovoked pain; the patient may have paraesthesia (pins and needles); dysaesthesia
(unpleasant sensory perceptions usually but not necessarily secondary to provocation, such as the sensation
of running cold water); allodynia (pain on light touch); or hyperalgesia (increased pain perception following a
painful stimulus, including hot and cold stimuli). Similar sensory abnormalities may be found outside of the area
innervated by the damaged nerve, particularly for the visceral and muscle hyperalgesia.
The cutaneous sensory dysfunction may be associated with superficial dispareunia, but also irritation
and pain associated with clothes brushing the skin. There may also be a lack of sensation and pain may
occur in the presence of numbness. Visceral hypersensitivity may result in an urge to defecate or urinate. This
is usually associated with voiding frequency, with small amounts urine being passed. Pain on visceral filling
may occur. Anal pain and loss of motor control may result in poor bowel activity, with constipation and/or
incontinence. Ejaculation and orgasm may also be painful or reduced.
Many of those suffering from pudendal neuralgia complain of fatigue and generalised muscle cramps,
weakness and pain. Being unable to sit is a major disability, and over time, patients struggle to stand and they
often become bedbound. The immobility produces generalised muscle wasting, and minimal activity hurts. As a
consequence of the widespread pain and disability, patients often have emotional problems, and in particular,
depression. Patients with CPP are also often anxious and have the tendency to catastrophise. Depression,
catastrophising and disability are all poor prognostic markers.
Cutaneous colour may change due to changes in innervation but also because of neurogenic oedema. The
patient may describe the area as swollen due to this oedema, but also to the lack of afferent perception.
6.4.2.5 Clinical examination
A full clinical examination of the spinal, muscular, nervous and urogenital systems is necessary to aid in
diagnosis of pudendal neuralgia, especially to detect signs indicating another pathology. Often there is little
to find in pudendal neuralgia and frequently findings are non-specific. The main pathognomonic features
are the signs of nerve injury in the appropriate neurological distribution, for example, allodynia or numbness.
Tenderness in response to pressure over the pudendal nerve may aid the clinical diagnosis. This may be
elicited by per rectal or per vaginal examination and palpation in the region of the ischeal spine and/or Alcock’s
canal. Muscle tenderness and the presence of trigger points in the muscles may confuse the picture. Trigger
points may be present in a range of muscles, both within the pelvis (levator ani and obturator internus muscles)
or externally (e.g., the piriformis, adductors, rectus abdominus or paraspinal muscles).
6.4.2.6 Investigations
Magnetic resonance imaging scans of the pelvis are usually normal although some practitioners claim them to
be useful (35,36). However, MRI scans of the pelvis and spine (mid thoracic to coccyx) are considered essential
to help with the differential diagnosis of pudendal neuralgia. Electrophysiological studies may reveal signs of
perineal denervation, increased pudendal nerve latency, or impaired bulbocavernosal reflex (25,34,37-39).
However, for an abnormality to be detected, significant nerve damage is probably necessary. Pain may be
associated with limited nerve damage, therefore, these investigations are often normal in patients thought to
have pudendal neuralgia.

96 UPDATE FEBRUARY 2012
6.5 Management of pain associated with nerve damage
The approach to managing a patient with pain following nerve damage is similar irrespective of the nerve
involved. There is a suggestion that early treatment has a better prognosis. The general principles are covered
in chapter 10 of this document.
6.5.1 Pudendal neuralgia and injections
The role of injections may be divided into two. First, an injection of local anaesthetic and steroid at the sight of
nerve injury may produce a therapeutic action. The possible reasons for this are related to the fact that steroids
may reduce any inflammation and swelling at the site of nerve irritation, but also because steroids may block
sodium channels and reduce irritable firing from the nerve. The second possible benefit of local infiltration is
diagnostic. It has already been indicated that when the pudendal nerve is injured there are several sites where
this may occur. Differential block of the pudendal nerve helps to provide information in relation to the site
where the nerve may be trapped (16-20,35,40-44).
Infiltration at the ischeal spine requires the use of a nerve stimulator/locator. Both motor (anal contraction)
and sensory endpoints may be noted. The anatomical endpoint may be localised by fluoroscopy, computed
tomography (CT) guidance, or the use of ultrasound. Ultrasound avoids any form of radiation, whereas CT
guidance involves a significant amount of radiation. Currently, fluoroscopy is probably the imaging technique
most frequently used because it is readily available to most anaesthetists that perform the block.
Currently, infiltration of the pudendal nerve within Alcock’s canal is primarily undertaken with the use of CT.
As well as injecting around the pudendal nerve, specific blocks of other nerves arising from the pelvis may be
performed. Similarly, trigger point injections into tender areas within muscles may also be considered. Pulsed
radiofrequency stimulation has also been suggested as a treatment (45).
6.5.2 Pudendal neuralgia and surgery
Decompression of an entrapped or injured nerve is a routine approach and probably should apply to the
pudendal nerve as it applies to all other nerves. There are several approaches and the approach of choice
probably depends upon the nature of the pathology. The most traditional approach is the transgluteal
approach; however, a transperineal approach may be an alternative, particularly if the nerve damage is thought
to be related to previous pelvic surgery (11,14,33,35,46-48).
Currently, there has been only one prospective randomised study (11). This suggests that, if the patient has
had the pain for < 6 years, 66% of patients will see some improvement with surgery (compared to 40% if
the pain has been present for > 6 years). Surgery is by no means the answer for all patients. On talking to
patients that have undergone surgery, providing the diagnosis was clear-cut, most patients are grateful to have
undergone surgery but many still have symptoms that need management.
6.5.3 Pudendal neuralgia and neuromodulation
Pudendal neuralgia represents a peripheral nerve injury and as such should respond to neuromodulation by
implanted pulse generators. However, it is important that the stimulation is perceived in the same site as the
perceived pain. Spinal cord stimulation (SCS) may be effective for thoraco-lumbar afferents. However, it is
difficult to obtain appropriate stimulation from SCS for the sacral nerves including pudendal. There is limited
experience with sacral root stimulation and as a result stimulation for pudendal neuralgia should only be
undertaken in specialised centres and in centres that can provide multidisciplinarycare (49-51).
6.6 Conclusions and recommendations: pudendal neuralgia
Conclusions LE
Multiple sensory and functional disorders within the region of the pelvis/urogenital system may occur
as a result of injury to one or more of many nerves. The anatomy is complex.
2
There is no single aetiology for the nerve damage and the symptoms and signs may be few or
multiple.
1
Investigations are often normal. 2
The peripheral nerve pain syndromes are frequently associated with negative cognitive, behavioural,
sexual, or emotional consequences.
1
There are multiple treatment options with varying levels of evidence. 1

UPDATE FEBRUARY 2012 97
Recommendations GR
It is important to rule out confusable diseases. A
If a peripheral nerve pain syndrome is suspected, early referral should occur to an expert in the field,
working within a multidisciplinary team environment.
B
Imaging and neurophysiology may help with the diagnosis, but the gold standard investigation is an
image and nerve locator guided local anaesthetic injection.
B
Neuropathic pain guidelines are well established. Standard approaches to management of
neuropathic pain should be utalised.
A
Figure 14: assessment and treatment algorithm for peripheral nerve pain syndrome
6.7 References
1. Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for
clinical and research purposes. Neurology. 2008 Apr 29;70(18):1630-5
http://www.ncbi.nlm.nih.gov/pubmed/18003941
2. Jensen TS, Madsen CS, Finnerup NB. Pharmacology and treatment of neuropathic pains. Curr Opin
Neurol. 2009 Oct;22(5):467-74.
http://www.ncbi.nlm.nih.gov/pubmed/19741531
3. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural
plasticity. J Pain. 2009 Sep;10(9):895-926.
http://www.ncbi.nlm.nih.gov/pubmed/19712899
4. Jensen TS, Baron R, Haanpää, et al. A new definition of neuropathic pain. Pain. 2011
Oct;152(10):2204-5.
http://www.ncbi.nlm.nih.gov/pubmed/21764514
5. Goebel, A. (2011). Complex regional pain syndrome in adults. Rheumatology (Oxford). 2011
Oct;50(10):1739-50.
http://www.ncbi.nlm.nih.gov/pubmed/21712368
6. Goebel, A, Baranowski A, Maurer K, et al. Intravenous immunoglobulin treatment of the complex
regional pain syndrome: a randomized trial. Ann Intern Med. 2010 Feb 2;152(3):152-8.
http://www.ncbi.nlm.nih.gov/pubmed/20124231
7. Nickel JC, Tripp DA, Pontari M, et al. Interstitial cystitis/painful bladder syndrome and associated
medical conditions with an emphasis on irritable bowel syndrome, fibromyalgia and chronic fatigue
syndrome. J Urol. 2010 Oct;184(4):1358-63.
http://www.ncbi.nlm.nih.gov/pubmed/20719340
8. Warren JW, Wesselmann U, Morozov V, et al. Numbers and types of nonbladder syndromes as risk
factors for interstitial cystitis/painful bladder syndrome. Urology. 2011 Feb;77(2):313-9.
http://www.ncbi.nlm.nih.gov/pubmed/21295246
9. Antolak SJ Jr, Hough DM, Pawlina W. et al. Anatomical basis of chronic pelvic pain syndrome: the
ischial spine and pudendal nerve entrapment. Med Hypotheses. 2002 Sep;59(3):349-53.
http://www.ncbi.nlm.nih.gov/pubmed/12208168
10. Mahakkanukrauh P, Surin P, Vaidhayakarn P. Anatomical study of the pudendal nerve adjacent to the
sacrospinous ligament. Clin Anat. 2005 Apr;18(3):200-5.
http://www.ncbi.nlm.nih.gov/pubmed/15768420
Extended
neurological tests
Extended history
on nature of pain
Standardised
questionnaires (1)
Assessment
Grade A recommended
Treatment
Grade B recommended
Refer to an expert when a peripheral nerve problem is suspected
Imaging may be of help (2)
Neurophysiology may be of help (3)
Treatment is as for any other nerve injury
http://publications.nice.org.uk/neuropathic-pan-cg96
1. Horowitz SH. The diagnostic workup of patients with neuropathic pain. Med Clin North Am. Jan 2007;91(1):21-30.
http://www.ncbi.nlm.nih.gov/pubmed/17164102
2. Kim S, Choi JY, Huh YM, et al. Role of magnetic resonance imaging in entrapment and compressive neuropathy - what,where, and
how to see the peripheral nerves on the musculoskeletal magnetic resonance image: part 1. Overview and lower extremity. Eur
Radiol. Jan 2007;17(1):139-149.
http://www.ncbi.nlm.nih.gov/pubmed/16572334
3. Labat JJ, Delavierre D, Sibert L, et al. [Electrophysiological studies of chronic pelvic and perineal pain]. Prog Urol. Vol 20. France:
2010 Elsevier Masson SAS; 2010:905-910.
http://www.ncbi.nlm.nih.gov/pubmed/21056364

98 UPDATE FEBRUARY 2012
11. Robert R, Labat JJ, Bensignor M, et al. Decompression and transposition of the pudendal nerve
in pudendal neuralgia: a randomized controlled trial and long-term evaluation. Eur Urol. 2005
Mar;47(3):403-8.
http://www.ncbi.nlm.nih.gov/pubmed/15716208
12. Ashton-Miller JA, DeLancey JO. Functional anatomy of the female pelvic floor. Ann N Y Acad Sci.
2007 Apr;1101:266-96.
http://www.ncbi.nlm.nih.gov/pubmed/17416924
13. Moszkowicz D, Alsaid B, Bessede T, et al. Where does pelvic nerve injury occur during rectal surgery
for cancer? Colorectal Dis. 2011 Dec;13(12):1326-34.
http://www.ncbi.nlm.nih.gov/pubmed/20718836
14. Robert R, Labat JJ, Khalfallah M, et al. [Pudendal nerve surgery in the management of chronic pelvic
and perineal pain]. Prog Urol. 2010 Nov;20(12):1084-8.
http://www.ncbi.nlm.nih.gov/pubmed/21056388
15. Filippiadis DK, Velonakis G, Mazioti A, et al. CT-guided percutaneous infiltration for the treatment of
Alcock’s neuralgia. Pain Physician. 2011 Mar-Apr;14(2):211-5.
http://www.ncbi.nlm.nih.gov/pubmed/21412375
16. Bolandard, F, Bazin JE. Nerve stimulator guided pudendal nerve blocks. Can J Anaesth. Canada. 52:
773; author reply 773-774.
http://www.ncbi.nlm.nih.gov/pubmed/16103396
17. Naja MZ, Al-Tannir MA, Maaliki H, et al. Nerve-stimulator-guided repeated pudendal nerve block for
treatment of pudendal neuralgia. Eur J Anaesthesiol. 2006 May;23(5):442-4.
http://www.ncbi.nlm.nih.gov/pubmed/16573866
18. Wey PF, Lions C, Rimmelé T, et al. [Nerve stimulator guided pudendal nerve block for postoperative
analgesia. An evaluation of professional practice]. Ann Fr Anesth Reanim. France. 26: 1087-1088.
http://www.ncbi.nlm.nih.gov/pubmed/17961968
19. Peng PW, Tumber PS. Ultrasound-guided interventional procedures for patients with chronic pelvic
pain - a description of techniques and review of literature. Pain Physician. 2008 Mar-Apr;11(2):215-24.
http://www.ncbi.nlm.nih.gov/pubmed/18354713
20. Kim S, Song S, Paek O, et al. Nerve-stimulator-guided pudendal nerve block by pararectal approach.
Colorectal Dis. 2011 Jul 13. doi: 10.1111/j.1463-1318.2011.02720.x. [Epub ahead of print].
http://www.ncbi.nlm.nih.gov/pubmed/21752174
21. Matejcik V. Anatomical variations of lumbosacral plexus. Surg Radiol Anat. 2010 Apr;32(4):409-14.
http://www.ncbi.nlm.nih.gov/pubmed/19696958
22. Hahn L. Treatment of ilioinguinal nerve entrapment - a randomized controlled trial. Acta Obstet
Gynecol Scand. 2011 Sep;90(9):955-60.
http://www.ncbi.nlm.nih.gov/pubmed/21615360
23. Klaassen Z, Marshall E, Tubbs RC, et al. Anatomy of the ilioinguinal and iliohypogastric nerves with
observations of their spinal nerve contributions. Clin Anat. 2011 May;24(4):454-61.
http://www.ncbi.nlm.nih.gov/pubmed/21509811
24. Goldet R, Kerdraon J, Amarenco G. [Traction on the orthopedic table and pudendal nerve injury.
Importance of electrophysiologic examination]. Rev Chir Orthop Reparatrice Appar Mot. 1998
Oct;84(6):523-30.
http://www.ncbi.nlm.nih.gov/pubmed/9846326
25. Amarenco G, Ismael SS, Bayle B, et al. Electrophysiological analysis of pudendal neuropathy following
traction. Muscle Nerve. 2001 Jan;24(1):116-9.
http://www.ncbi.nlm.nih.gov/pubmed/11150974
26. Alevizon SJ, Finan MA. Sacrospinous colpopexy: management of postoperative pudendal nerve
entrapment. Obstet Gynecol. 1996 Oct;88(4 Pt 2):713-5.
http://www.ncbi.nlm.nih.gov/pubmed/8841264
27. Fisher HW, Lotze PM. Nerve injury locations during retropubic sling procedures. Int Urogynecol J.
2011 Apr;22(4):439-41.
http://www.ncbi.nlm.nih.gov/pubmed/21060989
28. Kapoor DS, Thakar R, Sultan AH. Combined urinary and faecal incontinence. Int Urogynecol J Pelvic
Floor Dysfunct. 2005 Jul-Aug;16(4):321-8.
http://www.ncbi.nlm.nih.gov/pubmed/15729476
29. Amarenco G, Kerdraon J, Lanoe Y. [Perineal neuropathy due to stretching and urinary incontinence.
Physiopathology, diagnosis and therapeutic implications]. Ann Urol (Paris). 1990;24(6):463-6.
http://www.ncbi.nlm.nih.gov/pubmed/2176777

UPDATE FEBRUARY 2012 99
30. Darnis B, Robert R, Labat JJ, et al. Perineal pain and inferior cluneal nerves: anatomy and surgery.
Surg Radiol Anat. 2008 May;30(3):177-83.
http://www.ncbi.nlm.nih.gov/pubmed/18305887
31. Labat JJ, Robert R, Delavierre D, et al. [Symptomatic approach to chronic neuropathic somatic pelvic
and perineal pain]. Prog Urol. 2010 Nov;20(12):973-81.
http://www.ncbi.nlm.nih.gov/pubmed/21056374
32. Robert R, Prat-Pradal D, Labat JJ, et al. Anatomic basis of chronic perineal pain: role of the pudendal
nerve. Surg Radiol Anat. 1998;20(2):93-8.
http://www.ncbi.nlm.nih.gov/pubmed/9658526
33. Shafik A. Pudendal canal syndrome as a cause of vulvodynia and its treatment by pudendal nerve
decompression. Eur J Obstet Gynecol Reprod Biol. 1998 Oct;80(2):215-20.
http://www.ncbi.nlm.nih.gov/pubmed/9846672
34. Labat JJ, Riant T, Robert R, et al. Diagnostic criteria for pudendal neuralgia by pudendal nerve
entrapment (Nantes criteria). Neurourol Urodyn. 2008;27(4):306-10.
http://www.ncbi.nlm.nih.gov/pubmed/17828787
35. Filler AG. Diagnosis and treatment of pudendal nerve entrapment syndrome subtypes: imaging,
injections, and minimal access surgery. Neurosurg Focus. 2009 Feb;26(2):E9.
http://www.ncbi.nlm.nih.gov/pubmed/19323602
36. Insola A, Granata G, Padua L. Alcock canal syndrome due to obturator internus muscle fibrosis.
Muscle Nerve. 2010 Sep;42(3):431-2.
http://www.ncbi.nlm.nih.gov/pubmed/20665515
37. Lee JC, Yang CC, Kromm BG, et al. Neurophysiologic testing in chronic pelvic pain syndrome: a pilot
study. Urology. 2001 Aug;58(2):246-50.
http://www.ncbi.nlm.nih.gov/pubmed/11489711
38. Lefaucheur JP, Labat JJ, Amarenco G, et al. What is the place of electroneuromyographic studies in
the diagnosis and management of pudendal neuralgia related to entrapment syndrome? Neurophysiol
Clin. 2007 Aug-Sep;37(4):223-8.
http://www.ncbi.nlm.nih.gov/pubmed/17996810
39. Labat JJ, Delavierre D, Sibert L, et al. [Electrophysiological studies of chronic pelvic and perineal pain].
Prog Urol. 2010 Nov;20(12):905-10.
http://www.ncbi.nlm.nih.gov/pubmed/21056364
40. Thoumas, D, Leroi AM, Mauillon J, et al. Pudendal neuralgia: CT-guided pudendal nerve block
technique. Abdom Imaging. 1999 May-Jun;24(3):309-12.
http://www.ncbi.nlm.nih.gov/pubmed/10227901
41. Kovacs P, Gruber H, Piegger J, et al. New, simple, ultrasound-guided infiltration of the pudendal
nerve: ultrasonographic technique. Dis Colon Rectum. 2001 Sep;44(9):1381-5.
http://www.ncbi.nlm.nih.gov/pubmed/11584221
42. Antolak SJ Jr, Antolak CM. Therapeutic pudendal nerve blocks using corticosteroids cure pelvic pain
after failure of sacral neuromodulation. Pain Med. 2009 Jan;10(1):186-9.
http://www.ncbi.nlm.nih.gov/pubmed/19222779
43. Rigaud J, Riant T, Delavierre D, et al. [Somatic nerve block in the management of chronic pelvic and
perineal pain]. Prog Urol. 2010 Nov;20(12):1072-83.
http://www.ncbi.nlm.nih.gov/pubmed/21056387
44. Romanzi L. Techniques of pudendal nerve block. J Sex Med. 2010 May;7(5):1716-9.
http://www.ncbi.nlm.nih.gov/pubmed/20537059
45. Rhame EE, Levey KA, Ghraibo CG. Successful treatment of refractory pudendal neuralgia with pulsed
radiofrequency. Pain Physician. 2009 May-Jun;12(3):633-8.
http://www.ncbi.nlm.nih.gov/pubmed/19461829
46. Bautrant E, de Bisschop E, Vaini-Elies V, et al. [Modern algorithm for treating pudendal neuralgia: 212
cases and 104 decompressions]. J Gynecol Obstet Biol Reprod (Paris). 2003 Dec;32(8 Pt 1):705-12.
http://www.ncbi.nlm.nih.gov/pubmed/15067894
47. Possover M, Baekelandt J, Flaskamp C, et al. Laparoscopic neurolysis of the sacral plexus and
the sciatic nerve for extensive endometriosis of the pelvic wall. Minim Invasive Neurosurg. 2007
Feb;50(1):33-6.
http://www.ncbi.nlm.nih.gov/pubmed/17546541
48. Robert R, Labat JJ, Riant T, et al. Neurosurgical treatment of perineal neuralgias. Adv Tech Stand
Neurosurg. 2007;32:41-59.
http://www.ncbi.nlm.nih.gov/pubmed/17907474

100 UPDATE FEBRUARY 2012
49. Mayer RD, Howard FM. Sacral nerve stimulation: neuromodulation for voiding dysfunction and pain.
Neurotherapeutics. 2008 Jan;5(1):107-13.
http://www.ncbi.nlm.nih.gov/pubmed/18164489
50. Carmel M, Lebel M, Tu le M. Pudendal nerve neuromodulation with neurophysiology guidance:
a potential treatment option for refractory chronic pelvi-perineal pain. Int Urogynecol J. 2010
May;21(5):613-6.
http://www.ncbi.nlm.nih.gov/pubmed/20012596
51. Marcelissen T, Van Kerrebroeck P, de Wachter S. Sacral neuromodulation as a treatment for
neuropathic clitoral pain after abdominal hysterectomy. Int Urogynecol J. 2010 Oct;21(10):1305-7.
http://www.ncbi.nlm.nih.gov/pubmed/20386879
7. SEXOLOGICAL ASPECTS OF CHRONIC PELVIC
PAIN
7.1 Introduction
In general human sexuality has three aspects – sexual function, sexual self-concept, and sexual relationships.
Pain can affect self-esteem, ones ability to enjoy sex and relationships. Healthy sexuality is a positive and
life-affirming part of being human. The capacity to experience optimal comfort and satisfaction in sexual
expression also requires basic physical abilities. Essentially, these include intact sensory and motor processes,
and the ability to move with ease.
Chronic pain may hinder the ability to move freely, and thus, may limit the positions one can get into
to have sex. Second, chronic pain may affect the ability to respond sexually and conversely; in CPP the sex
act can be associated with pain that can be inhibiting. Research on male sexual dysfunction highlights the
importance of considering partners and the impact that male sexual problems have on their partners. Sexual
dysfunction occurs in an interpersonal context and has implications for both partners in a relationship. Chronic
pain also impacts the sexual and interpersonal functioning of couples; declines in sexual activity and reduced
relationship satisfaction have been noted among patients with chronic pain and their partners (1,2).
It is recommended that a biopsychosocial model of CPPS should be incorporated into future research, and that
research considers the role that sexual and relationship variables may play in couples’ adjustment.
The sexual-response cycle is divided into five phases: desire, arousal (excitement), plateau, orgasm and
resolution. They are actually all part of a continuous process of sexual response. There is much variation
among individuals, as well as between different sexual events and there are different models to describe the
sexual responses (3).
During the sexual response cycle, the different phases are controlled by a different part of the brain and spinal
cord. In each of these phases chronic pain and CPP in particular can cause disturbances (4).
• TheDesirePhasebeginsinthe“pleasurecenters”ofthebrainandcontrolsaperson’ssexualappetite
or drive. Pain or even the fear of pain can decrease desire, making the person uninterested in sex. In
some cases, however, having sex may actually help to relieve pain.
• TheArousalPhaseisassociatedwiththeswellingofthebloodvesselsinaman’spenisandina
woman’s labia, vagina, and clitoris. This swelling causes an erection in the penis and in the clitoris
and release of lubricating fluids. If a person experiences pain at the time of becoming excited, the
excitement may be reversed, in a man the penis will become limp and in a woman the lubrication will
stop, leading to dryness.
• TheOrgasmPhasedescribesagenitalreflexcontrolledbythespinalcord,whichcausesthegenital
muscles to contract, involuntarily releasing sexual tension and swelling that build up during the
excitement phase. In some cases, pain prevents people from reaching this phase.
7.2 General considerations
Pelvic pain in women (5) and in men (6) is associated with significant sexual dysfunction. While chronic pain
impacts all aspects of functioning, including work, family relationships, and social activities, the most frequent
complaint cited by patients with CPP is sexual dysfunction (7). Factors contributing to sexual dysfunction
in patients with chronic pain are multifactorial and contextual (8), and may be related to comorbidity with
depression (9,10), use of antidepressant medications (11), and relationship satisfaction (12), among many other
factors. There are reports of increased rates of past sexual abuse which may have negative impact on sexual

UPDATE FEBRUARY 2012 101
function (13,14). Chronic pelvic pain may have a higher association with sexual dysfunction than other types of
chronic pain. CPP specifically involves areas intimately connected to sexuality, which may negatively impact
one’s body image and sexual self-esteem (15), and also affects both partners in the relationship (16).
7.3 Pelvic floor involvement in sexual function and dysfunction
The pelvic floor of the male appears to have some impact on sexual function, although its exact role is unclear.
Erection is a neurovascular event in which the smooth and striated musculature of the corpora cavernosa and
pelvic floor play a role in facilitating and maintaining the erection (17). In ejaculation and orgasm the rhythmic
contraction of the bulbocavernous and ischiocavernous muscles is perceived as pleasurable. Ejaculation is
controlled by the sympathetic nervous system and performed with help of the pelvic floor muscles. Controlling
the pelvic floor muscles may delay the onset of ejaculation through an active relaxation of the pelvic floor
muscles. This is a learned technique, which may be mastered using pelvic floor biofeedback. Pelvic floor
exercise and biofeedback for the treatment of both erectile dysfunction (ED) and premature ejaculation (PE)
have been reported on in the literature.
Early studies maintained that strong pelvic floor muscles in women, particularly the ischiocavernous
muscle that attaches to the clitoral hood, were crucial for adequate genital arousal and attainment of orgasm
(18), and that weak muscles may provide insufficient activity necessary for vaginal friction or blood flow, and
inhibit orgasmic potential (19). It has also been proposed that sexual pleasure is enhanced for both partners
by genital responses provided by contraction of the levator ani (20). It stands to reason, therefore, that better
control over pelvic floor muscle contraction and relaxation could improve sexual function.
However, few studies are available to support this notion. In a Scandinavian randomised controlled
study pelvic floor muscle training has been demonstrated to improve QoL and sexual function in women with
urinary stress incontinence (20). In a Turkish study, improvement in sexual desire, performance during coitus,
and achievement of orgasm were reported in women (n=42) who received pelvic floor muscle re-education (21).
The effectiveness of physical therapy in treating sexual pain disorders has been reported upon in the
literature as well. Retrospective studies have reported on a success rate of 77% (22,23). Goetsch recently
reported her findings that physical therapy may serve as important adjunct to surgery for “vulvar vestibulitis”
(vulvar pain syndrome) (24).
7.4 Chronic pelvic pain and sexual dysfunction of the male
In the BACH study, Hu et al. found that men who reported having experienced sexual, physical, or emotional
abuse had increased odds (1.7 compared to 3.3) for symptoms suggestive of PPS. The authors suggested
that clinicians may wish to screen for abuse in men presenting with symptoms suggestive of PPS. Conversely,
clinicians may wish to inquire about pelvic pain in patients who have experienced abuse (25).
A key feature of PPS is chronic pain. Chronic pain and its treatment can impair our ability to express
sexuality. In a study in England 73% of patients with chronic pain had some degree of sexual problems as
result of the pain (8). These problems can occur because of several factors. Psychological factors like decrease
in self-esteem, depression and anxiety can contribute to loss of libido. Physiological factors like fatigue, nausea
and pain itself can cause sexual dysfunction. Pain medications (opioids, and the selective serotonin reuptake
inhibitors, SSRI) can also decrease libido (26) and delay ejaculation.
The evaluation of the effects of PPS on sexual function should take into consideration the adverse
effects of drug therapy of PPS on sexuality, as well as the more interesting direct interactions between the PPS
symptoms and disorders of libido, erectile function and ejaculation.
The number of studies on the effects of CPP on sexual function is limited. Sexual dysfunction is often ignored
because of a lack of standardised measurements. At the present, the most commonly used tool is the
international index of erectile function (IIEF) questionnaire (27). Post-ejaculation pain is not mentioned in this
questionnaire.
In the 1980s an association between PPS and sexual dysfunction was postulated (28). This study reported a
high incidence of decreased libido in patients with PPS, and they also concluded that this syndrome should
be viewed as a psychosomatic disorder. Where as psychology may play a role in the genesis of the pain,
nowadays, we would say there is little evidence to support PPS as being a psychiatric disorder, but rather a
biopsychological disorder in certain cases. For more information on this issue see Chapter 3.1.
In 2 reviews the relation between PPS and health status, with influence on sexual activity, were addressed
(29,30).
In a Chinese study of men with PPS 1768 males completed the questionnaires. The overall prevalence of
sexual dysfunction was 49%. Erectile dysfunction is the most investigated sexual dysfunction in PPS patients.
The reported prevalence of ED ranges from 15.1% to 48%, varying with the evaluation tools and populations
(31,32). Erectile dysfunction was prevalent in 27.4% of Italian men aged 25-50 (33), 15.2% among Turkish men
(significantly higher than control group) (34) and 43% among Finnish men with PPS (35). The prevalence of ED

102 UPDATE FEBRUARY 2012
was found to be higher in young men with PPS than in the general population.
According to other studies men with pelvic pain had higher chance of suffering from ED (36,37).
Recently, a significant correlation between “chronic prostatitis”, PPS symptoms (measured by NIH-CPSI) and
ED (measured by IIEF) was confirmed (38), while other studies using the same questionnaires were not able
to confirm such a correlation (27,39). Some studies also report ejaculatory dysfunction, mainly premature
ejaculation (6,22,31,32). According to the definition set up by the International Society for Sexual Medicine,
PE is “a male sexual dysfunction characterised by ejaculation which always or nearly always occurs prior to
or within about one minute of vaginal penetration, and inability to delay ejaculation on all or nearly all vaginal
penetrations” (40). The reported prevalence of PE varies widely in PPS patients, but unlike ED the prevalence
does not increase with age (32).
A study from Turkey concerning the interaction between PPS and premature ejaculation (PE)
according to intravaginal ejaculation latency time showed that 77% of men with PPS suffered from PE (34).
Screponi et al. (2001) reported the high incidence of prostatic inflammation symptoms in men with PE (41).
Premature ejaculation associated with PPS is hypothesised to be caused by infection or inflammation,
thus treatment with antibiotics should reduce PE symptoms. In 2 studies antibiotic treatment has shown a
significant increase in patients IELT (intravaginal ejaculation latency time). Despite these improvements, the
mean IELT was still very low and questionable. Before these results can be recommended further placebo
controlled, studies are mandatory (42,43).
Furthermore, there are reports which highlight the appearance of ejaculatory pain in patients with
PPS (44), while some studies suggested PPS symptoms improvement by increased ejaculatory frequency and
sexual activity (45,46).
The presence of pelvic pain may increase the risk for erectile dysfunction independently of age (47). On the
other hand, cross-sectional data suggest no improvement of lower urinary tract symptons (LUTS) by an
increased frequency of ejaculation (30). In a study bridging the gap between LUTS and ED, Muller and Mulhall
have speculated on the negative impact of PPS on QoL, leading to consecutive impairment of erectile function
(48). Although mental distress and impaired QoL related to illness could contribute to sexual dysfunction
observed in patients with PPS, the presence of erectile and ejaculatory disorders is more frequently related to
symptoms and imaging suggestive of a more severe inflammatory condition (6). These arguments are important
for the understanding of the close relationship between CPP symptoms, disturbed sexuality, impact on QoL,
and psychological implications including depression (29-32,49).
Sexual dysfunction heightens anger, frustration and depression, all of which place a strain on the
relationship and the partner. The female partners of men with sexual dysfunction and depression often present
with similar symptoms including pain upon intercourse and depressive symptoms. Men with PPS have
reported a high frequency of sexual relationship dissolution and psychological symptoms, such as depression
and suicidal thinking (29,48). Prostate pain syndrome patients reported greater sexual and relationship
problems: 45% reported an increase in pain during or following intercourse, and many reported avoiding sexual
relationships for fear of spreading an infection to their partner (50). On the other hand, Smith et al. found that
men with PPS did not report significant decrease of sexual satisfaction compared to control. The results of the
study suggested that while men with PPS and their partners may experience some sexual difficulties, PPS may
not have a large negative impact on patients’ intimate relationships (51). Aubin et al. found that men appeared
open to the initiation of sex and assumed their partners were sexually satisfied (52).
There is a consensus that therapeutic strategies reducing symptoms, especially against pelvic pain,
are of relevance in relation to changes of sexuality. On the other hand, having sex and intimacy can yield
positive experiences that will reduce the pain. The central nervous system plays an important role in this
mechanism.
7.5 Chronic pelvic pain and sexual dysfunction of the female
Chronic pelvic pain is a clinical condition that results from the complex interactions of physiological and
psychological factors and has a direct impact on the social, marital, and professional lives of women. Chronic
pelvic pain leads to substantial impairment in QoL and several sexual dysfunctions (53-56).
It seems reasonable to expect that pain, extreme fatigueness, depressive mood and pain drugs will
affect women’s sexuality. Women with pain may report a variety of sexual problems ranging from decreased
pleasure and frequency of intercourse, superficial or deep dyspareunia, and problems in reaching orgasm to
a total aversion toward sexual intimacy of any kind. Ter Kuile et al. found in their study that women with CPP
reported significantly more pain, depression, and anxiety symptoms and were physically more impaired than
women in the control group. In comparison with controls, women with CPP reported significantly more sexual
avoidance behavior, non-sensuality, and complaints of “vaginismus” (57).
Chronic pelvic pain is more directly associated with sexual dysfunction than chronic pain at other
sites. In one study of CPP patients’ feelings and beliefs about their pain or illness, 40 out of 64 participants
cited sexual dysfunction as one of the chief problems the illness had caused, making it the most frequent

UPDATE FEBRUARY 2012 103
complaint (58). Collett and colleagues (59) also found that patients with CPP reported more sexual problems
than women with any other type of chronic pain problem.
The quality of intimate relationships is closely connected with sexual function (60). Satisfaction
with the sexual relationship appears to be associated with higher marital functioning (61). In addition to its
relationship with marital dissatisfaction, sexual dissatisfaction is related to sexual dysfunction. In cases in
which one partner suffers from chronic pain, the ability of both partners to cope with the pain and the extent
to which partners are supportive of the chronic pain sufferer have been found to be a predictor of sexual
functioning (61).
In community-based studies in the UK (7), New Zealand (54) and Australia (62), a substantially larger
proportion of the women with CPP reported dyspareunia (varying between 29% and 42%) than women without
CPP (varying between 11% and 14%). Only a few studies have investigated sexual problems within clinical
populations (59,63,64). The study of Veritt et al. shows that all of the sexual function domains (desire, arousal,
lubrication, orgasm, satisfaction, and pain) were significantly lower in women with CPP than in women without
CPP (64). In line with the results of the community based studies, patients with CPP reported more sexual
problems such as dyspareunia, problems with desire or arousal and lubrication than women without CPP (63-
65).
One study of patients enrolled in chronic pain treatment programs in England has reported that 73%
had pain-related sexual problems (8). Approximately two-thirds of patients in another study have reported
reduced frequency in their sexual relations as a result of CPP (66).
One study demonstrated that CPP patients reported worse sexual function with regard to desire, arousal,
lubrication, orgasm, satisfaction, and more frequent and severe pain with vaginal penetration than women
without sexual dysfunction (67).
Maruta et al. interviewed 50 chronic pain sufferers and their spouses, of whom 78% of the pain sufferers and
84% of partners described deterioration, including cessation of their sex life (1). In another study, in patients
with back pain, half reported decreased frequency of sex since the onset of chronic pain (8)
The female sexual function index (FSFI) has been developed as a brief, multidimensional self-report
instrument for assessing the key dimensions of sexual function in women, which includes desire, subjective
arousal, lubrication, orgasm, satisfaction, and pain. The study of Veritt FF et al. showed that when FSFI was
used women with CPP reported worse sexual function in all subscales and total score than did women without
CPP; the largest differences between women with CPP and without CPP were seen for the domains of pain
and arousal; the correlations of FSFI corresponded well to each other; the total score and the subscales of the
FSFI had high levels of internal consistency and test–retest reliability when assessed in a sample of women
with CPP; and finally, that the FSFI showed good ability to discriminate between women with and without CPP
(67).
Some studies report a significant association between sexual abuse before the age of 15 years and
later CPP (13). It is suggested that there is increased frequency of sexual abuse or trauma history, anxiety and
depression in women with CPP (68-72). While the study of Fry et al. with 164 women with CPP show that child
sexual abuse did not apparently differ in prevalence from that in the general population, which must throw into
question previous assertions about its widespread and general role in CPP.
7.6 Treatment of sexual dysfunctions and CPP
Couples often benefit from early referral for relationship and sexual counseling during their treatment course
(73). Specific behavioral strategies for women who have urogenital complaints and female sexual dysfunction
often include exploring alternatives to sexual intercourse (manual or oral pleasuring), different coital positions
(female superior or side lying), and pacing, such as limiting thrusting to less than that that causes. Planning for
the time of intercourse is important, and scheduling a clinic visit after intercourse might be useful to identify
specific sites and causes of postcoital flares. Other behavioral changes involve pre- and postcoital voiding,
application of ice packs to the genital or suprapubic area (73,74), and use of vaginal dilators before penile
penetration. An alternative is to use natural dilators such as different fingers or sex toys. Hypoallergenic
non-irritating lubricants can be used to reduce vulvar, urethra, and vaginal friction, and women with signs of
vulvovaginal atrophy may benefit from introital application of minimally absorbed locally applied oestrogen
cream (75). In patients with an overactive pelvic floor, referral for physical therapy, myofascial release, and
internal pelvic floor muscle massage may offer relief (4).
7.7 In summary
Problems with sexual functioning resulting from CPP have to be addressed and assessed by the health-care
professional. The attention directed toward these patients must be focused not only on the disease but also
on the woman as a whole. As treatment solely of the underlying disease is not acceptable, the care of these
suffering women should also address the emotional, sexual, and social problems that the disease causes.

104 UPDATE FEBRUARY 2012
7.8 Conclusions and recommendations: sexological aspects in CPP
Conclusions LE
Chronic pain can lead to decline in sexual activity and satisfaction and may reduce relationship
satisfaction.
2a
Patients who reported having sexual, physical or emotional abuse show a higher rate of reporting
symptoms of PPS.
2b
Sexual dysfunctions are prevalent in patient with PPS. 2b
In men with PPS the most prevalent sexual complains are erectile dysfunction and ejaculatory
dysfunctions.
3
In females with CPPS all sexual function domains are lower. The most reported dysfunctions are
sexual avoidance, dyspareunia and “vaginismus”.
2a
Vulvar pain syndrome is associated with BPS. 3
Women with BPS suffer significantly more from fear of pain, dyspareunia and less desire. 2a
Pelvic floor muscle function is involved in the excitement and orgasm phases of sexual response. 3
Chronic pain can cause disturbances in each of the sexual response cycle phases. 2b
Pelvic floor muscle physical therapy may offer relief of pain and reduction in sexual complains. 2b
Recommendations GR
Clinicians may screen for abuse in patients presenting with symptoms suggestive for prostate pain
syndrome without suggesting a causal relation with the pain.
B
The biopsychosocial model should be applied in the evaluation of the effect of prostate pain
syndrome on the sexual function of the patient.
B
The biopsychosocial model should be incorporated in research in the role of chronic pelvic pain in
sexual dysfunction.
B
Behavioral strategies should be offered to the patient and his/her partner to cope with sexual
dysfunctions.
B
Training of the pelvic floor muscles is recommended to improve quality of life and sexual function. B
Figure 15: assessment and treatment algorithm for sexological aspects in chronic pelvic pain
7.9 References
1. Maruta T, Osborne D, Swanson DW et al. Chronic pain patients and spouses. Marital and sexual
adjustment. Mayo Clin Proc 1981 May;56(5):307–10.
http://www.ncbi.nlm.nih.gov/pubmed/7230895
2. Flor H, Turk DC, Scholtz OB. Impact of chronic pain on the spouse: Marital, emotional and physical
consequences. J Psychosom Res 1987;31(1):63–71.
http://www.ncbi.nlm.nih.gov/pubmed/3820147
3. Human sexuality (5° ed ). MASTERS William, JOHNSON Virginia, KOLODNY Robert. © 1995-2011
LAVOISIER S.A.S
History of sexual
functioning
History of negative
experiences
Ask about abuse
Psychiatric history
History of
relationship
Assessment
Grade A recommended
Treatment
Grade B recommended
Refer to sexologist when sexual dysfunction or trauma is present
Screen for sexual abuse
Use a bio-psycho-social model in treating the pain
Offer behavioral strategies to cope with sexual dysfunctions
Offer partner treatment
Refer for pelvic floor physiotherapy
UPDATE FEBRUARY 2012 105
4. Rosenbaum TY, Owens A. The role of pelvic floor physical therapy in the treatment of pelvic and
genital pain-related sexual dysfunction. J Sex Med 2008 Mar;5(3):513–23.
http://www.ncbi.nlm.nih.gov/pubmed/18304280
5. Randolph ME, Reddy DM. Sexual functioning in women with chronic pelvic pain: The impact of
depression, support, and abuse. J Sex Res 2006 Feb;43(1):38–45.
http://www.ncbi.nlm.nih.gov/pubmed/16817066
6. Trinchieri A, Magri V, Cariani L et al. Prevalence of sexual dysfunction in men with chronic prostatitis/
chronic pelvic pain syndrome. Arch Ital Urol Androl 2007 Jun;79(2):67–70.
http://www.ncbi.nlm.nih.gov/pubmed/17695411
7. Zondervan KT, Yudkin PL, Vessey MP et al. The prevalence of chronic pelvic pain in women in the
United Kingdom: A systematic review. Br J Obstet Gynaecol 1998 Jan;105(1):93–9.
http://www.ncbi.nlm.nih.gov/pubmed/9442169
8. Ambler N, Williams AC, Hill P et al. Sexual difficulties of chronic pain patients. Clin J Pain 2001
Jun;17(2):138–45.
http://www.ncbi.nlm.nih.gov/pubmed/11444715
9. Averill PM, Novy DM, Nelson DV et al. Correlates of depression in chronic pain patients: A
comprehensive examination. Pain 1996 Apr;65(1):93–100.
http://www.ncbi.nlm.nih.gov/pubmed/8826495
10. Philipp M, Delini-Stula A, Baier D et al. Assessment of sexual dysfunction in depressed patients and
reporting attitudes in routine daily practice: Results of the postmarketing observational studies with
moclobemide, a reversible MAO-A inhibitor. Int J Psychiatry Clin Pract 1999;3:257–64.
11. Ferguson JM. The effects of antidepressants on sexual functioning in depressed patients: A review.
J Clin Psychiatry 2001;62 Suppl 3:22–34.
http://www.ncbi.nlm.nih.gov/pubmed/11229450
12. Coates R, Ferroni EA. Sexual dysfunction and marital disharmony as a consequence of chronic lumbar
spinal pain. Sex Marital Ther 1991;6:65–9.
13. Lampe A, Solder E, Ennemoser A et al. Chronic pelvic pain and previous sexual abuse. Obstet
Gynecol 2000 Dec;96(6):929–33.
http://www.ncbi.nlm.nih.gov/pubmed/11084180
14. Rellini A, Meston CM. Sexual abuse and female sexual dysfunction: Clinical implications. Urodinamica
2004;14:80–3.
15. Heinberg LJ, Fisher BJ, Wesselmann U et al. Psychological factors in pelvic/urogenital pain: The
influence of site of pain versus sex. Pain 2004 Mar;108(1-2):88–94.
http://www.ncbi.nlm.nih.gov/pubmed/15109511
16. Smith KB, Tripp D, Pukall C et al. Predictors of sexual and relationship functioning in couples with
chronic prostatitis/chronic pelvic pain syndrome. J Sex Med 2007 May;4(3):734–44.
http://www.ncbi.nlm.nih.gov/pubmed/17451490
17. McMahon CG, Abdo C, Incrocci L et al. Disorders of orgasm and ejaculation in men. J Sex Med 2004
Jul;1(1):58–65.
http://www.ncbi.nlm.nih.gov/pubmed/16422984
18. Graber B, Kline-Graber G. Female orgasm: Role of the pubococcygeus muscle. J Clin Psychiatry 1979
Aug;40(8):348–51.
19. Shafik A. The role of the levator ani muscle in evacuation, sexual performance, and pelvic floor
disorders. Int Urogynecol J Pelvic Floor Dysfunct 2000 Dec;11(6):361–76.
http://www.ncbi.nlm.nih.gov/pubmed/11147745
20. Bo K, Talseth T, Vinsnes A. Randomized controlled trial on the effect of pelvic floor muscle training on
quality of life and sexual problems in genuine stress incontinent women. Acta Obstet Gynecol Scand
2000 Jul;79(7):598–603.
http://www.ncbi.nlm.nih.gov/pubmed/10929962
21. Beji NK, Yalcin O, Erkan HA. The effect of pelvic floor training on sexual function of treated patients.
Int Urogynecol J Pelvic Floor Dysfunct 2003 Oct;14(4):234–8.
http://www.ncbi.nlm.nih.gov/pubmed/14530833
22. Anderson, Wise D, Sawyer T et al. Sexual dysfunction in men with CP/CPPS: Improvement after
trigger point release. Paradoxical relaxation training.J Urol 2006 Oct;176(4 Pt 1):1534–8.
http://www.ncbi.nlm.nih.gov/pubmed/16952676
23. Bergeron S, Brown C, Lord MJ et al. Physical therapy for vulvar vestibulitis syndrome: A retrospective
study. J Sex Marital Ther 2002 May-June;28(3):183–92.
http://www.ncbi.nlm.nih.gov/pubmed/11995597

106 UPDATE FEBRUARY 2012
24. Goetsch MF. Surgery combined with muscle therapy for dyspareunia from vulvar vestibulitis: An
observational study. J Reprod Med 2007 Jul;52(7):597–603.
http://www.ncbi.nlm.nih.gov/pubmed/17847757
25. Hu JC, Link CL, McNaughton-Collins M et al. The Association of Abuse and Symptoms Suggestive of
Chronic Prostatitis/Chronic Pelvic Pain Syndrome: Results from the Boston Area Community Health
Survey. J Gen Intern Med 2007 Nov;22(11):1532–7.
http://www.ncbi.nlm.nih.gov/pubmed/17763912
26. Fleming MP, Paice JA. Sexuality and chronic pain. Journal of Sex Education and Therapy
2001.26:204-214.
27. Rosen RC, Riley A, Wagner G et al. The international index of erectile function (IIEF): A
multidimensional scale for assessment of erectile dysfunction. Urology 1997 Jun;49(6):822-30.
http://www.ncbi.nlm.nih.gov/pubmed/9187685
28. Keltikangas-Jarvinen L, Jarvinen H, Lehtonen T. Psychic disturbances in patients with chronic
prostatis. Ann Clin Res. 1981 Feb;13(1):45-9.
29. Berghuis JP, Heiman JR, Rothman I et al. Psychological and physical factors involved in chronic
idiopathic prostatitis. J Psychosom Res. 1996 Oct;41(4):313-25.
http://www.ncbi.nlm.nih.gov/pubmed/8971661
30. Jacobsen SJ, Jacobson DJ, Rohe DE et al. Frequency of sexual activity and prostatic health: fact or
fairy tale? Urology. 2003 Feb;61(2):348-53.
http://www.ncbi.nlm.nih.gov/pubmed/12597946
31. Lee SW, Liong ML, Yuen KH et al. Adverse impact of sexual dysfunction in chronic prostatitis/chronic
pelvic pain syndrome. Urology 2008 Jan;71(1):79-84.
http://www.ncbi.nlm.nih.gov/pubmed/18242370
32. Liang CZ, Zhang XJ, Hao ZY et al. Prevalence of sexual dysfunction in Chinese men with chronic
prostatitis. BJU Int 2004 Sep;94(4):568-70.
http://www.ncbi.nlm.nih.gov/pubmed/15329114
33. Bartoletti R, Cai T, Mondaini N et al. Prevalence, incidence estimation, risk factors and
characterization of chronic prostatitis/chronic pelvic pain syndrome in urological hospital outpatients
in Italy: Results of a multicenter case-control observational study. J Urol 2007 Dec;178(6):2411-5.
http://www.ncbi.nlm.nih.gov/pubmed/17937946
34. Gonen M, Kalkan M, Cenker A et al. Prevalence of premature ejaculation in Turkish men with chronic
pelvic pain syndrome. J Androl 2005 Sep-Oct;26(5):601–3.
http://www.ncbi.nlm.nih.gov/pubmed/16088036
35. Mehik A, Hellstrom P, Sarpola A et al. Fears, sexual disturbances and personality features in men with
prostatitis: A population-based cross-sectional study in Finland. BJU Int 2001 Jul;88(1):35-8.
http://www.ncbi.nlm.nih.gov/pubmed/11446842
36. Weidner W, Wagenlehner FM, Marconi M et al. Acute bacterial prostatitis and chronic prostatitis/
chronic pelvic pain syndrome: andrological implications. Andrologia. 2008 Apr;40(2):105-12.
http://www.ncbi.nlm.nih.gov/pubmed/18336460
37. O’Leary MP, Fowler FJ, Lenderking WR et al. A brief male sexual function inventory for urology.
Urology. 1995 Nov;46(5):697-706.
http://www.ncbi.nlm.nih.gov/pubmed/7495124
38. Qiu YC, Xie CY, Zeng XD et al. Investigation of sexual function in 623 patients with chronic prostatitis.
Zhonghua Nan Ke Xue. 2007 Jun;13(6):524-6.
http://www.ncbi.nlm.nih.gov/pubmed/17615977
39. Davis SN, Binik YM, Carrier S: Sexual dysfunction and pelvic pain in men: A male sexual pain
disorder? J Sex Marital Ther 2009; 35:182-205
40. McMahon CG, Abdo C, Incrocci L et al. Disorders of orgasm and ejaculation in men. J Sex Med 2004
Jul;1(1):58–65.
http://www.ncbi.nlm.nih.gov/pubmed/16422984
41. Screponi E, Carosa E, Di Stasi SM et al. Prevalence of chronic prostatitis in men with premature
ejaculation. Urology. 2001 Aug;58(2):198-202.
http://www.ncbi.nlm.nih.gov/pubmed/11489699
42. Hennenfent BR, Feliciano AE. Changes in white blood cell counts in men undergoing thrice-weekly
prostatic massage, microbial diagnosis and antimicrobial therapy for genitourinary complaints. Br J
Urol 1998 Mar;81(3):370-6.
http://www.ncbi.nlm.nih.gov/pubmed/9523654
43. El-Nashaar A, Shamloul R. Antibiotic treatment can delay ejaculation in patients with premature
ejaculation and chronic bacterial prostatitis. J Sex Med 2007 Mar;4(2):491-6.
http://www.ncbi.nlm.nih.gov/pubmed/17367444

UPDATE FEBRUARY 2012 107
44. Ilie CP, Mischianu DL, Pemberton RJ. Painful ejaculation. BJU international 2007 Jun;99(6):1335-9.
http://www.ncbi.nlm.nih.gov/pubmed/17346279
45. Shoskes DA, Landis JR, Wang Y et al. Impact of post-ejaculatory pain in men with category III chronic
prostatitis/chronic pelvic pain syndrome. J Urol 2004 Aug;172(2):542-7.
http://www.ncbi.nlm.nih.gov/pubmed/15247725
46. Weidner W, Ludwig M, Miller J. Therapy in male accessory gland infection--what is fact, what is
fiction? Andrologia. 1998;30 Suppl 1:87-90.
http://www.ncbi.nlm.nih.gov/pubmed/9629448
47. Marszalek M, Wehrberger C, Temml C et al. Chronic Pelvic Pain and Lower Urinary Tract Symptoms
in Both Sexes: Analysis of 2749 Participants of an Urban Health Screening Project. Eur Urol. 2009
Feb;55(2):499-507.
http://www.ncbi.nlm.nih.gov/pubmed/18395963
48. Muller A, Mulhall JP. Sexual dysfunction in the patient with prostatitis. Curr Opin Urol. 2005
Nov;15(6):404-9.
http://www.ncbi.nlm.nih.gov/pubmed/16205492
49. Tripp DA, Nickel JC, Ross S et al. Prevalence, symptom impact and predictors of chronic
prostatitislike symptoms in Canadian males aged 16-19 years. BJU international 2009
Apr;103(8):1080-4.
http://www.ncbi.nlm.nih.gov/pubmed/19007369
50. Egan KJ, Krieger JL. Psychological problems in chronic prostatitis patients with pain. Clinical Journal
of Pain 1994 Sep;10(3):218–26.
http://www.ncbi.nlm.nih.gov/pubmed/7833580
51. Smith KB, Pukall CF, Tripp DA, Nickel JC. Sexual and Relationship Functioning in Men with Chronic
Prostatitis/Chronic Pelvic Pain Syndrome and Their Partners. Arch Sex Behav 2007;36:301–311.
52. Aubin S, Berger RE, Heiman JR, Ciol MA: The association between sexual function, pain, and
psychological adaptation of men diagnosed with chronic pelvic pain syndrome type III. J Sex Med
2008;5:657-667.
53. Gunter J. Chronic pelvic pain: An integrated approach to diagnosis and treatment. Obstet Gynecol
Surv 2003 Sep;58(9):615–23.
http://www.ncbi.nlm.nih.gov/pubmed/12972837
54. Grace V, Zondervan K. Chronic pelvic pain in women in New Zealand: Comparative well-being,
comorbidity, and impact on work and other activities. Health Care Women Int 2006 Aug;27(7):585–99.
http://www.ncbi.nlm.nih.gov/pubmed/16844672
55. Latthe P, Latthe M, Say L, Gulmezoglu M et al. WHO systematic review of prevalence of chronic pelvic
pain: A neglected reproductive health morbidity. BMC Public health 2006 Jul 6;6:177.
http://www.ncbi.nlm.nih.gov/pubmed/16824213
56. Pearce C, Curtis M. A multidisciplinary approach to self care in chronic pelvic pain. Br J Nurs 2007
Jan 25-Feb 7;16(2):82–5.
http://www.ncbi.nlm.nih.gov/pubmed/17353816
57. ter Kuile MM, Weijenborg PTM, Spinhoven P. Sexual functioning in women with chronic pelvic pain:
The role of anxiety and depression. J Sex Med 2010 May;7(5):1901–10.
http://www.ncbi.nlm.nih.gov/pubmed/19678881
58. Fry RPW, Crisp AH, Beard RW. Patients’ illness models in chronic pelvic pain. Psychother Psychosom
1991;55(2-4):158–63.
http://www.ncbi.nlm.nih.gov/pubmed/1891563
59. Collett BJ, Cordle CJ, Stewart CR et al. A comparative study of women with chronic pelvic pain,
chronic nonpelvic pain and those with no history of pain attending general practitioners. Br J Obstet
Gynecol 1998 Jan;105(1):87–92.
http://www.ncbi.nlm.nih.gov/pubmed/9442168
60. McCabe MP, Jupp JJ. Intercorrelations among general arousability, emerging and current sexual
desire, and severity of sexual dysfunction in women. Psychol Rep. 1989 Aug;65(1):147-54.
http://www.ncbi.nlm.nih.gov/pubmed/2780925
61. Flor H, Kerns RD, Turk DC. The role of spouse reinforcement, perceived pain, and activity levels of
chronic pain patients. J Psychosoma Res 1987;31(2):251-9.
http://www.ncbi.nlm.nih.gov/pubmed/3585827
62. Pitts MK, Ferris JA, Smith AM et al. Prevalence and correlates of three types of pelvic pain in a
nationally representative sample of Australian women. Med J Aust 2008 Aug 4;189(3):138–43.
http://www.ncbi.nlm.nih.gov/pubmed/18673099

108 UPDATE FEBRUARY 2012
63. Florido J, Perez-Lucas R, Navarrete L. Sexual behavior and findings on laparoscopy or laparotomy in
women with severe chronic pelvic pain. Eur J Obstet Gynecol Reprod Biol 2008 Aug;139(2):233–6.
http://www.ncbi.nlm.nih.gov/pubmed/18403089
64. Verit FF, Verit A, Yeni E. The prevalence of sexual dysfunction and associated risk factors in women
with chronic pelvic pain: A cross-sectional study. Arch Gynecol Obstet 2006 Aug;274(5):297–302.
http://www.ncbi.nlm.nih.gov/pubmed/16705463
65. Phillips NA. The clinical evaluation of dyspareunia. Int J Impot Res 1998 May;10 Suppl 2:S117–20.
http://www.ncbi.nlm.nih.gov/pubmed/9647973
66. Paice J. Sexuality and chronic pain. Am J Nurs 2003 Jan;103(1):87–9.
http://www.ncbi.nlm.nih.gov/pubmed/12544064
67. Verit FF, Verit A. Validation of the Female Sexual Function Index in women with chronic pelvic pain.
J Sex Med 2007 Nov;4(6):1635–41.
http://www.ncbi.nlm.nih.gov/pubmed/17888066
68. Roelofs K, Spinhoven P. Trauma and medically unexplained symptoms towards an integration of
cognitive and neurobiological accounts. Clin Psychol Rev 2007 Oct;27(7):798–820.
http://www.ncbi.nlm.nih.gov/pubmed/17728032
69. McGowan LPA, Clark-Carter DD, Pitts MK. Chronic pelvic pain: A meta-analytic review. Psychol
Health 1998;13:937–51.
70. Leonard LM, Follette VM. Sexual functioning in women reporting a history of child abuse. Review of
the empirical literature and clinical implications. Annu Rev Sex Res 2002;13:346–88.
http://www.ncbi.nlm.nih.gov/pubmed/12836736
71. Angst J. Sexual problems in healthy and depressed persons. Int Clin Psychopharmacol 1998 Jul;13
Suppl 6:S1–4.
http://www.ncbi.nlm.nih.gov/pubmed/9728667
72. Walker EA, Katon WJ, Hansom J, et al. Psychiatric diagnoses and sexual victimization in women with
chronic pelvic pain. Psychosomatics 36:531–540, 1995.
http://www.ncbi.nlm.nih.gov/pubmed/7501783
73. Kellogg-Spadt S, Whitmore KE. Role of the female urologist/urogynecologist. In: Goldstein I,
Meston CM, Davis SR, Traish AM, eds. Women’s sexual function and dysfunction: Study, diagnosis
and treatment. Vol. 17. London: Taylor and Francis; 2006:708–14.
74. Webster DC, Brennan T. Use and effectiveness of sexual self-care strategies for interstitial cystitis.
Urol Nurs 1995 Mar;15(1):14–22.
http://www.ncbi.nlm.nih.gov/pubmed/7792618
75. Hayes RD, Bennett CM, Fairley CK et al. What can prevalence studies tell us about female sexual
difficulty and dysfunction? J Sex Med 2006 Jul;3(4):589–95.
http://www.ncbi.nlm.nih.gov/pubmed/16839314

UPDATE FEBRUARY 2012 109
8. PSYCHOLOGICAL ASPECTS OF CHRONIC
PELVIC PAIN
This chapter first addresses general issues concerning the psychological contribution to pelvic pain and its
presenting problems, and assessment and treatment, and then it describes the same areas in relation to CPP
in women. This is by far the area with the greatest psychological contribution to pelvic and urogenital pain, and
exemplifies many of the problems raised in the first part of the chapter.
8.1 Understanding the psychological components of pain
8.1.1 Neurophysiology of pain
Models that integrate the psychological factors consistently found to be relevant in the maintenance of
persistent pelvic and urogenital pain with current neurobiological understanding of pain are few but of high
quality. Symptom-related anxiety and central pain amplification may be measurably linked, as in IBS (1).
Bajaj et al. (2) have demonstrated central sensitisation in symptomatic endometriosis, and this model is
more extensively dealt with in Chapter 4. The various mechanisms of facilitation, amplification, and failure of
inhibition, mean that there should be no expectation of a simple relationship between physical findings, pain
experienced, and resulting distress and restriction of activities. Difficulty disengaging even from expected
painful stimuli, undergone voluntarily and within tolerable levels, is characteristic in people struggling with
chronic pain (3). However, difficult as it is to relieve chronic pain, the pain system is plastic and treatment
attempts are not entirely unsuccessful.
8.1.2 Sexual abuse and trauma
Many studies have reported high rates of childhood sexual abuse in adults with persistent pain, usually
in hospital care samples, and particularly by women with pelvic pain (4). However, all these studies are
retrospective, and there appears to be a relationship between poor study quality and likelihood of reporting
this association (5). The only prospective investigation into the relationship between childhood sexual abuse,
physical abuse, or neglect, and “medically unexplained pain”, including pelvic pain, used court records
concerning sexual abuse before the age of 11 years to establish a definite history, comparing those with such
a history with demographically matched classmates (6). The conclusions of this study were that physically and
sexually abused individuals were not at risk for increased pain symptoms, although those individuals with pain
problems as adults were more likely to report earlier sexual or physical abuse or neglect; however, this did not
correspond with the established early history of abuse.
The correlation between childhood victimisation and pain symptoms is less straightforward than
previously thought, and may be more about retrospective explanatory frameworks used by women for pain
for which no major pathology is found than about occurrence or extent of abuse. In particular, findings of
depression and/or post-traumatic stress disorder in adult women reporting childhood sexual abuse are
common, with or without pain. Disentangling the influences and inferences requires prospective studies or
careful comparisons rather than, as in many published studies, comparing women with a history of sexual
abuse and CPP with women without either (7). No studies have been found about sexual or physical abuse in
childhood and pelvic pain in men, although it is evident that they suffer other adverse effects on psychological
and physical health (8,9).
8.1.3 Interpreting psychological differences
An important review (7) of CPP in women identifies as problematic the notion that women without physical
findings to which pain can be causally attributed differ in psychological characteristics from women with
physical findings. They have critically examined the methodologies of studies purporting to show such
differences, and the bias introduced by sampling and by unsuitable measures. They argue for better
methodology in replication of these studies, particularly those sampling life events, and for greater use of
idiographic methods.
In summary, women with pelvic pain often have other ‘medically unexplained’ symptoms, and
current or lifetime anxiety and depression disorder; they may have a history of physical or sexual abuse in
childhood but the significance of this for pelvic pain is unclear. Studies that invoke ‘medically unexplained’
or ‘psychosomatic’ or ‘somatoform’ disorders do not engage with current understanding of pain, such as
viscerovisceral cross sensitisation in relation to multiple pain sites (10), referring instead to a dualistic model in
which absence of physical findings is taken to indicate psychological origins of the complaint of pain (11,12).
At the extreme, pain is overshadowed by diagnosis as a sexual problem (‘dyspareunia’) when pain is in fact the
central problem and not contingent only on sexual activity (13).

110 UPDATE FEBRUARY 2012
8.2 Psychological assessment of pain
The report of anxiety, depression and sexual problems is sufficiently common for these to be important in
assessment and in planning treatment. Distress, described in the patient’s terms or within a psychodiagnostic
framework, is best understood in the context of pain and the meaning of pain to the individual.
Anxiety probably refers to fears of missed pathology as the cause of pain (cancer being foremost
among these) and to uncertainties about the possibilities of treatment and the likely prognosis if treated or
untreated. A question such as that suggested by Howard (14), “What do you believe or fear is the cause of your
pain?” is more suitable than a general anxiety questionnaire.
Depression is also commonly found in men and women with persistent pelvic pain (15). In a study
comparing men and women with low back pain, and women with pelvic pain and men with urogenital pain (16),
it was found that, when differences in age and pain duration and severity were taken into account, there were
no differences in depression according to pain site, and pain site predicted disability.
However, there is a risk when using diagnostic or standard assessment instruments of attributing
pain-related problems to neurovegetative signs of depression (17,18). As Stones et al. (19) has cautioned:
“Psychological distress may be a consequence and not a cause of persistent pain: while identification of
depression is important as part of treatment, caution is required before attribution of causality” (p416).
Pain ratings themselves may be predicted by cognitive and emotional variables (20). Furthermore,
target outcomes of pain severity, distress and disability co-vary only partly, and improvement in one does not
necessarily imply improvement in the others. Therefore, it is particularly important when the primary outcome is
pain to anchor its meaning in a study such as that by Gerlinger et al. (21), who determined clinically important
differences in pain in relation to overall satisfaction with treatment.
There are many measures of restricted function, or disability, most suited to musculosketal pain and
mobility problems rather than the difficulties of the individual with pelvic or urogenital pain. Some include one
or more items related to sexual activity, but there has perhaps been an over-emphasis on the effects of pain on
sexual performance, although the overall relationship may be more important (22).
In the Cochrane review of pelvic pain in women (23), the outcomes of pharmacotherapy, surgery and
physical therapy trials consist of pain scores (patient-rated and physican-estimated); functional measures such
as urinary peak flow rate (for persistent pelvic pain in men); examination findings such as pelvic tenderness
(women); and uptake of further treatment following the trial treatment. A few trials have included QoL, but
none has measured mood change. This indicates a general but mistaken assumption that improvement in pain
leads to resolution of other problems. Furthermore, if all treatments sampled the same domains of pain in their
evaluation, comparison across treatments, by medical personnel and patients, would be more easily achieved
(24). Suggested instruments for assessment in each of these domains can be found in the consensus paper by
Turk et al (25).
8.3 Psychological issues in the treatment of pain
Provision of information that is personalised and responsive to the presenting problem and the concerns
of the patient, conveying belief and concern, is a powerful way to allay anxiety (26). It can be helpful to
provide additional written information or direct the patient to reliable sources. Many practitioners rely on
locally produced material or pharmaceutical products of variable quality, although they endorse the need for
independent materials for patients (27).
Ideally, treatment arises from general principles and practice in the field of chronic pain, with specific
study of the population of concern and design of appropriate treatment trials (28). The field of pelvic pain
shows a curious phenomenon whereby few of the mainstream psychologically based treatments are subjected
to trials and published, but instead there are often rather idiosyncratic versions of treatment components, or
combinations of interventions, published in single, often underpowered trials. It is hard to conclude anything
from these, as is seen in the psychological treatment section of several other chapters.
Psychological interventions may be directed at the pain itself, with the intended outcome of reducing
pain and its consequent impact on life, or adjustment to pain, with improved mood and function and reduced
health care use, with or without pain reduction. The major psychologically based treatment that improves
adjustment, which is aimed more at reducing distress and disability than pain, is cognitive behavioural therapy,
for which there has been > 10 systematic reviews (29), although its effects may be small and maintenance
in the longer term is uncertain. For less disabled and distressed patients, this can be delivered in part over
the internet (30). A systematic review of short-term psychodynamic psychotherapy (31) has reported similar
improvements in “somatic disorders”, which often includes pelvic pain, although it was not among the trials
reviewed. Pain-focused interventions, again with no trials in pelvic pain, have been subjected to systematic
review, including hypnotherapy (32) and autogenic training (33).
However, all these systematic reviews suffer from heterogeneity among the trials, shortcomings in
trial methodology, and little longer-term follow-up to establish maintenance of treatment gains. The crucial
question, of what works best for whom, is unanswered and possibly unanswerable given the complexity of

UPDATE FEBRUARY 2012 111
variables, outcomes, and the difficulties in standardising treatments.
8.4 Female pelvic pain
8.4.1 Psychological risk factors in development and maintenance of pelvic pain
A thorough review from nearly 15 years ago (34) argues against division of aetiology into organic versus
psychogenic, and concludes that, given the methodological problems of many studies, the evidence for
sexual abuse as a risk factor is uncertain. A large review and meta-analysis of risk factors, including physical
pathology, psychological distress, and sexual abuse (35) drew mainly on retrospective studies, which
introduced various biases. Pelvic pain and distress may be variously related, each as the consequence of the
other, or arising independently.
The only systematic review (5) of risk factors for chronic non-cyclical pelvic pain in women included
the following as well as medical variables: sexual or physical abuse (ORs from 1.51 to 3.49); psychological
problems such as anxiety (OR: 2.28, 95% CI: 1.41- 3.70) and depression (OR: 2.69, 95% CI: 1.86-3.88);
hysteria, i.e., multiple somatic problems (OR: 4.83, 95% CI: 2.50-9.33); and psychosomatic symptoms (OR:
8.01, 95% CI: 5.16-12.44). The terms hysteria and psychosomatic symptoms can best be understood as
multiple somatic symptoms not associated with or indicative of any serious disease process, and personality
variables are not reliably associated with pelvic pain in women. Although some of these risk factors are
doubtless interrelated - history of sexual abuse and depression, for instance - such effects cannot be
disentangled from the studies available.
Issues of early trauma such as childhood sexual or physical abuse as a risk factor are addressed in
more detail earlier in this chapter, but it is important to say that better quality studies, including one prospective
study using court records of childhood abuse (6), have reported a weaker or no relationship, or not one
which is specific to pelvic pain (5, 36-38). However, another systematic review (9) has concluded that there is
some evidence for a specific relationship between rape and CPP (and also with fibromyalgia and functional
gastrointestinal disorders). It is also important to recognise the possible role of recent sexual assault on the
presentation of pelvic pain (4,39).
There have been fewer studies of maintenance of or recovery from pelvic pain in relation to
psychological factors. Weijenborg et al. (40) have found that, in 25% of women treated surgically, recovery
from pelvic pain over a mean 3 years follow-up was not predicted by pain variables at baseline, nor by a
general measure of psychological distress or sociodemographic variables, or reports of childhood sexual
abuse.
Studies that have described pelvic pain as medically unexplained or psychosomatic, due to the lack of
physical findings, have been discarded. This is because such a distinction is unhelpful and is not informed by
our understanding of pain mechanisms (11). When diagnostic investigations are used to assign symptoms to
physical and mental origins, with no suggested connection between them, and with interest only in the former
type of symptoms, explanations are often experienced by women as scepticism about the reality or severity of
the pain (41). This can undermine the therapeutic relationship between the patient and the doctor (42). Ehlert et
al. (43) have found that women with pelvic pain with and without laparoscopic findings do not differ from one
another; only from pain-free controls, as anticipated by Savidge & Slade (7). Distress, described in the patient’s
terms or within a psychodiagnostic framework, is best understood in the context of pain and the meaning
of pain to the individual (7). In a large primary care study, Zondervan et al. (44) have noted the tendency to
attribute pelvic pain without obvious pathology to a psychological cause, and that it is increasingly recognised
as unhelpful; depression and anxiety are common in any chronic pain, not pelvic pain alone. They have found
that restriction by pain does not distinguish between women who do and do not seek healthcare, and that
there may be an anxiety-related cause of the pain in both groups.
8.4.2 Psychological assessment of pelvic pain
Anxiety and post-traumatic stress symptoms are common in some women with CPP (44,45), and may account
for substantial variance in health status and treatment use. Negative investigative findings do not necessarily
resolve women’s anxieties about what might be causing pain (26). Depression may be related to pain in various
ways, as described above. Until measures are available that are adequately standardised in patients with
pain, anxiety and distress may be best assessed by questions about concerns about the cause of pain, its
implications, and its consequences for everyday life (46).
Reference to the studies of the IMMPACT group (24) is recommended for guidance on outcome
measures suitable for pain trials.
8.4.3 Psychological factors in treatment of persistent pelvic pain
Untreated, there is a significant rate of symptom improvement. In one study, 25% of patients reported recovery
(nearly half with total recovery) over a 3-4-year period, and neither pain nor distress at baseline, nor intervention
received, was found to be associated with recovery (40). This recovery rate should be borne in mind when

112 UPDATE FEBRUARY 2012
interpreting results of treatment trials.
There is one Cochrane systematic review and meta-analysis of treatments for pelvic pain, excluding
that due to endometriosis, IBS, and chronic PID (47). All treatments were included (although the update
protocols split surgical from non-surgical (48), and outcomes were mainly pain scores, QoL, and resource use,
including healthcare resources. The 14 treatment trials included counselling, psychoeducation, reassurance,
and emotional disclosure, as well as a multicomponent pain management programme. The authors concluded
in favour of educational counselling combined with ultrasound scanning, which improved pain and mood; and a
multidisciplinary rehabilitative approach including surgery, pharmacotherapy, physiotherapy, and psychosocial
intervention, which improved function but not pain. Emotional disclosure (a stress reduction method) through
writing brought about a small improvement in some pain scores.
Several other reviews make positive comments on psychological involvement (49), and recommend
addressing psychological concerns from the outset rather than after other treatment has failed. Psychological
interventions may be directed (1) at the pain itself, with the intended outcome of reducing pain and its
consequent impact on life, or (2) at adjustment to pain, with improved mood and function and reduced health
care use, with or without pain reduction.
In the first category are relaxation and biofeedback methods of controlling and decreasing pain by
reducing muscle tension, and this is applied in mainly uncontrolled trials to pelvic floor retraining both in men
and women. The only RCT (50) applied a specific type of cognitively enhanced physical therapy to overall
muscle tension, but not to the pelvic floor, combined with normal gynaecological treatment compared with
gynaecological treatment alone. Pain was reduced by 50% and motor function improved in various aspects by
10 h of physical therapy, with particular attention to tension and relaxation and to the thoughts and emotions
that interfere with balanced posture and movement.
In the second category, multicomponent pain management, involving education, physical retraining,
behavioural change, and increasing activity, relaxation and cognitive therapy, is often applied to mixed groups
of chronic pain patients, including those with pelvic pain. A systematic review and meta-analysis (51) which
shows a good outcome for mixed chronic pain or back pain groups across pain experience, mood, coping,
and activity, cannot with confidence be extrapolated to women with pelvic pain alone. The only RCTs in CPP
used elements of this approach in combination with medroxyprogesterone acetate (MPA) or placebo (52).
Combination of MPA and psychological therapy outperformed other treatment methods in the long term, with
nearly three quarters of women reporting > 50% pain relief.
Several single treatments with benefits in other chronic pain or chronic health problems have been
tried in pelvic pain. Norman et al. (53) have compared emotional disclosure by writing about pain with writing
about positive events as a control. The differences were small but in favour of emotional disclosure on one
measure of pain appraisal, particularly in women with more distress at baseline. Given the extent of problems
associated with pelvic pain, this intervention on its own is unlikely to produce much change, but could be
combined with other components described above.
In a different intervention, Fenton et al. (54) have conducted a small RCT of transcranial direct current
stimulation compared to sham stimulation. Pain reduction was greater in the treatment group, in the first week
only, as was reduction in disability.
8.5 Conclusions and recommendations: psychological aspects of CPP
Conclusions LE
There is no evidence that distress generates complaints of pelvic pain, or that multiple symptoms
suggest unreality of pain.
2b
Current or recent sexual abuse should be assessed as possible contributory factors in pelvic pain. 2a
Psychological intervention in general can produce benefits in pain, mood, and quality of life,
depending on its content and focus.
1a
Psychologically informed physical therapy can improve pain and function. 1b
Combined exercise and cognitive behavioural therapy with medroxyprogesterone acetate can reduce
pain in a majority of women with pelvic pain.
1b
Transcranial direct current stimulation may reduce pain in the short term. 1b

UPDATE FEBRUARY 2012 113
Recommendations GR
Psychological distress is common in pelvic pain in women but should be interpreted in the context of
pain.
A
Ask the patient what she thinks may be wrong to cause pain, to allow the opportunity to inform and
reassure as appropriate.
B
Try psychological interventions in combination with medical and surgical treatment, or alone. A
Figure 16: assessment and treatment algorithm for psychological aspects of chronic pelvic pain
8.6 References
1. Berman SM, Naliboff BD, Suyenobu B, et al. Reduced brainstem inhibition during anticipated visceral
pain correlates with enhanced brain response to the visceral stimulus in women with irritable bowel
syndrome. J Neurosci. 2008 Jan 9;28(2):349-59.
http://www.ncbi.nlm.nih.gov/pubmed/18184777
2. Bajaj P, Bajaj P, Madsen H, et al. Endometriosis is associated with central sensitisation: a
psychophysical controlled study. J Pain. 2003 Sep;4(7):372-80.
http://www.ncbi.nlm.nih.gov/pubmed/14622679
3. Eccleston C, Crombez G. Worry and chronic pain: a misdirected problem solving model. Pain. 2007
Dec 5;132(3):233-6.
http://www.ncbi.nlm.nih.gov/pubmed/17961924
4. Hilden M, Schei B, Swahnberg K, et al. A history of sexual abuse and health: a Nordic multicentre
study. BJOG. 2004 Oct;111(10):1121-7.
http://www.ncbi.nlm.nih.gov/pubmed/15383115
5. Latthe P, Mignini L, Gray R, et al. Factors predisposing women to chronic pelvic pain: systematic
review. BMJ. 2006 Apr 1;332(7544):749-55.
http://www.ncbi.nlm.nih.gov/pubmed/16484239
6. Raphael KG, Widom CS, Lange G. Childhood victimization and pain in adulthood: a prospective
investigation. Pain. 2001 May;92(1-2):283-93.
http://www.ncbi.nlm.nih.gov/pubmed/11323150
7. Savidge CJ, Slade P. Psychological aspects of chronic pelvic pain. Journal of J Psychosom Res. 1997
May;42(5):433-44.
http://www.ncbi.nlm.nih.gov/pubmed/9194016
8. Leserman J. Sexual abuse history: prevalence, health effects, mediators, and psychological treatment.
Psychosom Med. 2005 Nov-Dec;67(6):906-15.
http://www.ncbi.nlm.nih.gov/pubmed/16314595
9. Paras ML, Murad MH, Chen LP, et al. Sexual abuse and lifetime diagnosis of somatic disorders. A
systematic review and meta-analysis. JAMA. 2009 Aug 5;302(5):550-61.
http://www.ncbi.nlm.nih.gov/pubmed/19654389
10. Malykhina AP. Neural mechanisms of pelvic organ cross-sensitisation. Neuroscience. 2007 Nov
9;149(3):660-72.
http://www.ncbi.nlm.nih.gov/pubmed/17920206
11. Grace VM. Pitfalls of the medical paradigm in chronic pelvic pain. Baillieres Best Pract Res Clin Obstet
Gynaecol. 2000 Jun;14(3):525-39.
http://www.ncbi.nlm.nih.gov/pubmed/10962640
12. Sharpe M, Carson A. ‘Unexplained’ somatic symptoms, functional syndromes, and somatization: do
we need a paradigm shift? Ann Intern Med. 2001 May 1;134(9 Pt 2):926-30.
http://www.ncbi.nlm.nih.gov/pubmed/11346330
13. Binik YM. The DSM diagnostic criteria for dyspareunia. Arch Sex Behav. 2010 Apr;39(2):292-303.
http://www.ncbi.nlm.nih.gov/pubmed/19830537
14. Howard FM. Chronic pelvic pain. Obstet Gynecol. 2003 Mar;101(3):594-611.
http://www.ncbi.nlm.nih.gov/pubmed/12636968
Psychological
history
Investigate pain-
related beliefs and
behavior
Assessment
Grade A recommended
Treatment
Grade B recommended
Interpret psychological distress in the context of pain
Psychological interventions as adjuvant to other modalities
Ask the patient what he or she believes may be the problem that
causes the pain
114 UPDATE FEBRUARY 2012
15. Fitzgerald MP, Link CL, Litman HJ, et al. Beyond the lower urinary tract: the association of urologic
and sexual symptoms with common illnesses. Eur Urol. 2007 Aug;52(2):407-15.
http://www.ncbi.nlm.nih.gov/pubmed/17382458
16. Heinberg LJ, Fisher BJ, Wesselman U, et al. Psychological factors in pelvic/urogenital pain: the
influence of site of pain versus sex. Pain. 2004 Mar;108(1-2):88-94.
http://www.ncbi.nlm.nih.gov/pubmed/15109511
17. Pincus T, Williams A. Models and measurements of depression in chronic pain. J Psychosom Res
1999;47:211-219.
http://www.ncbi.nlm.nih.gov/pubmed/10576470
18. Lorencatto C, Petta CA, Navarro MJ, et al. Depression in women with endometriosis with and without
chronic pelvic pain. Acta Obstet Gynecol Scand. 2006;85(1):88-92.
http://www.ncbi.nlm.nih.gov/pubmed/16521687
19. Stones RW, Selfe SA, Fransman S, et al. Psychosocial and economic impact of chronic pelvic pain.
Baillieres Best Pract Res Clin Obstet Gynaecol. 2000 Jun;14(3):415-31.
http://www.ncbi.nlm.nih.gov/pubmed/10962635
20. Tripp DA, Nickel JC, Wang Y, et al. Catastrophizing and pain-contingent rest predict patient
adjustment in men with chronic prostatitis/chronic pelvic pain syndrome. J Pain 2006 Oct;7 (10):
697-708.
http://www.ncbi.nlm.nih.gov/pubmed/17018330
21. Gerlinger C, Schumacher U, Faustman T, et al. Defining a minimally clinically important difference for
endometriosis-associated pelvic pain measured on a visual analog scale: analyses of two placebo-
controlled, randomized trials. Health Qual Life Outcomes. 2010 Nov 24;8:138.
http://www.ncbi.nlm.nih.gov/pubmed/21106059
22. Smith KB, Pukall CF. A systematic review of relationship adjustment and sexual satisfaction among
women with provoked vestibulodynia. J Sex Res. 2011 Mar;48(2-3):166-91.
http://www.ncbi.nlm.nih.gov/pubmed/21409713
23. Stones W, Cheong YC, Howard FM. Interventions for treating chronic pelvic pain in women (review).
Cochrane Database Syst Rev. 2000;(4):CD000387.
http://www.ncbi.nlm.nih.gov/pubmed/11034686
24. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials:
IMMPACT recommendations. Pain. 2005 Jan;113(1-2):9-19.
http://www.ncbi.nlm.nih.gov/pubmed/15621359
25. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT
recommendations. Pain. 2003 Dec;106(3):337-45.
http://www.ncbi.nlm.nih.gov/pubmed/14659516.
26. McGowan L, Luker K, Creed F, et al. ‘How do you explain a pain that can’t be seen?’: The narratives
of women with chronic pelvic pain and their disengagement with the diagnostic cycle. Br J Health
Psychol. 2007 May;12(Pt 2):261-74.
http://www.ncbi.nlm.nih.gov/pubmed/17456285
27. EAU Survey: What do you tell your patients?
http://www.uroweb.org/news/?act=showfull&aid=246
28. Nickel JC, Tripp D, Teal V, et al. Interstitial Cystitis Collaborative Trials Group. Journal of Urology
2007; 177: 1832-1836.
http://www.ncbi.nlm.nih.gov/pubmed/17437831
29. Eccleston C, Williams AC, Morley S. Psychological therapies for the management of chronic pain
(excluding headache) in adults. Cochrane Database Syst Rev. 2009 Apr 15;(2):CD007407.
http://www.ncbi.nlm.nih.gov/pubmed/19370688
30. Macea DD, Gajos K, Daglia Calil YA, et al. The efficacy of web-based cognitive behavioral
interventions for chronic pain: a systematic review and meta-analysis. Journal of Pain 2010;11:
917-929.
http://www.ncbi.nlm.nih.gov/pubmed/20650691
31. Abbass A, Kisely S, Kroenke K. Short-term psychodynamic psychotherapy for somatic disorders.
Psychother Psychosom. 2009;78(5):265-74.
http://www.ncbi.nlm.nih.gov/pubmed/19602915
32. Flammer E, Alladin A. The efficacy of hypnotherapy in the treatment of psychosomatic disorders:
meta-analytical evidence. Int J Clin Exp Hypn. 2007 Jul;55(3):251-74.
http://www.ncbi.nlm.nih.gov/pubmed/17558717
33. Stetter F, Kupper S. Autogenic training: a meta-analysis of clinical outcome studies. Appl
Psychophysiol Biofeedback. 2002 Mar;27(1):45-98.
http://www.ncbi.nlm.nih.gov/pubmed/12001885
UPDATE FEBRUARY 2012 115
34. Fry RP, Crisp AH, Beard RW. Sociopsychological factors in chronic pelvic pain: a review.
J Psychosom Res. 1997 Jan;42(1):1-15.
http://www.ncbi.nlm.nih.gov/pubmed/9055210
35. Zondervan K, Barlow DH. Epidemiology of chronic pelvic pain. Baillieres Best Pract Res Clin Obstet
Gynaecol. 2000 Jun;14(3):403-14.
http://www.ncbi.nlm.nih.gov/pubmed/10962634
36. Raphael KG, Chandler HK, Ciccone DS. Is childhood abuse a risk factor for chronic pain in adulthood?
Curr Pain Headache Rep. 2004 Apr;8(2):99-110.
http://www.ncbi.nlm.nih.gov/pubmed/14980144
37. Davis MA, Luecken LJ, Zautra AJ. Are reports of childhood abuse related to the experience of chronic
pain in adulthood? A meta-analytic review of the literature. Clin J Pain. 2005 Sep-Oct;21(5):398-405.
http://www.ncbi.nlm.nih.gov/pubmed/16093745
38. Maniglio R. The impact of child sexual abuse on health: a systematic review of reviews. Clin Psychol
Rev. 2009 Nov;29(7):647-57.
http://www.ncbi.nlm.nih.gov/pubmed/19733950
39. Campbell R, Lichty LF, Sturza M, et al. Gynecological health impact of sexual assault. Res Nurs
Health. 2006 Oct;29(5):399-413.
http://www.ncbi.nlm.nih.gov/pubmed/16977640
40. Weijenborg PT, Greeven A, Dekker FW, et al. Clinical course of chronic pelvic pain in women. Pain.
2007 Nov;132 Suppl 1:S117-23.
http://www.ncbi.nlm.nih.gov/pubmed/17689866
41. Savidge CJ, Slade P, Steward P, et al. Women’s perspectives on their experiences of chronic pelvic
pain and medical care. J Health Psychol. 1998 Jan;3(1):103-16..
http://www.ncbi.nlm.nih.gov/pubmed/22021346
42. Price J, Farmer G, Harris J, et al. Attitudes of women with chronic pelvic pain to the gynaecological
consultation: a qualitative study. BJOG. 2006 Apr;113(4):446-52.
http://www.ncbi.nlm.nih.gov/pubmed/16489938
43. Ehlert U, Heim C, Hellhammer DH. Chronic pelvic pain as somatoform disorder. Psychother
Psychosom. 1999 Mar-Apr;68(2):87-94.
http://www.ncbi.nlm.nih.gov/pubmed/10026460
44. Zondervan KT, Yudkin PL, Vessey MP, et al. The community prevalence of chronic pelvic pain in
women and associated illness behaviour. Br J Gen Pract. 2001 Jul;51(468):541-7.
http://www.ncbi.nlm.nih.gov/pubmed/11462313
45. Meltzer-Brody S, Leserman J, Zolnoun D, et al. Trauma and posttraumatic stress disorder in women
with chronic pelvic pain. Obstet Gynecol. 2007 Apr;109(4):902-8.
http://www.ncbi.nlm.nih.gov/pubmed/17400852
46. Allaire C, Taenzer P. History-taking, physical examination and psychological assessment. In: Jarrell
JF, Vilos GJ (editors) Consensus guidelines for the management of chronic pelvic pain. J Obstet
Gynaecol Can. 2005 Sep;27(9):869-910.
http://www.ncbi.nlm.nih.gov/pubmed/19830953
47. Stones RW, Mountfield J. Interventions for treating chronic pelvic pain in women. Cochrane Database
Syst Rev. 2000;(4):CD000387.
http://www.ncbi.nlm.nih.gov/pubmed/11034686
48. Cheong YC, Smotra G, Farquhar C. Non surgical interventions for the management of chronic pelvic
pain. Protocol. Cochrane Library 2010; issue 11.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD008797/abstract
49. Bordman R, Jackson B. Below the belt. Approach to chronic pelvic pain. Can Fam Physician. 2006
Dec;52(12):1556-62.
http://www.ncbi.nlm.nih.gov/pubmed/17279236
50. Haugstad GK, Haugstad TS, Kirste UM, et al. Mensendieck somatocognitive therapy as treatment
approach to chronic pelvic pain: Results of a randomized controlled intervention study. Am J Obstet
Gynecol. 2006 May;194(5):1303-10.
http://www.ncbi.nlm.nih.gov/pubmed/16647914
51. Morley SJ, Eccleston C, Williams ACdeC. Systematic review and meta-analysis of randomised
controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults,
excluding headache. Pain. 1999 Mar;80(1-2):1-13.
http://www.ncbi.nlm.nih.gov/pubmed/10204712

116 UPDATE FEBRUARY 2012
52. Farquhar CM, Rogers V, Franks S, et al. A randomized controlled trial of medroxyprogesterone
acetate and psychotherapy for the treatment of pelvic congestion. Br J Obstet Gynaecol. 1989
Oct;96(10):1153-62.
http://www.ncbi.nlm.nih.gov/pubmed/2531611
53. Norman SA, Lumley MA, Dooley JA, et al. For whom does it work? Moderators of the effects of written
emotional disclosure in a randomized trial among women with chronic pelvic pain. Psychosom Med.
2004 Mar-Apr;66(2):174-83.
http://www.ncbi.nlm.nih.gov/pubmed/15039501
54. Fenton BW, Palmieri PA, Boggio P, et al. A preliminary study of transcranial direct current stimulation
for the treatment of refractory pelvic pain. Brain Stimul. 2009 Apr;2(2):103-7.
http://www.ncbi.nlm.nih.gov/pubmed/20633407
9. PELVIC FLOOR FUNCTION AND CHRONIC
PELVIC PAIN
9.1 Introduction
The pelvic floor is made up of muscles and fascia. The muscles usually function as a composite, although
the anterior and posterior components may act in isolation. The pelvic floor has three functions: support,
contraction and relaxation.
9.2 Function
In its resting state, the pelvic floor supports the bladder and the urethra in the anterior compartment, the uterus
and the vagina in the middle compartment, and the rectum and the anus in the posterior compartment. The
integrity of the support function depends on the anatomical position of the muscles, on the resting tone and on
the integrity of the fascia. When intra-abdominal pressure rises, the pelvic floor muscles must respond with a
contraction occurring simultaneously or before the pressure rise. The latter is termed an anticipatory response
or feed-forward loop. Contraction of the pelvic floor muscles results in inward movement of the perineum and
upward movement of the pelvic organs. In many situations, other muscles such as the abdominal, adductor
and gluteal muscles also contract. There are two types of contraction that can be distinguished: a voluntary
contraction, resulting from impulses arising in the cerebral cortex, and a reflex contraction. These contractions
not only maintain support of the pelvic organs, they close the urethra, anus and vagina, thus avoiding loss of
urine or stools. Contractions also form a defence against introduction of foreign objects into the anus or vagina,
and in women, they can protect against sexual penetration. Additionally, detrusor muscle inhibition occurs in
parallel with pelvic floor muscle contraction. Pelvic floor muscle contractions play an important role in sexual
function. During the arousal phase, pelvic floor muscle contractions are used to increase vasocongestion.
During the final phase of the sexual response cycle, a series of involuntary contractions is associated with
the physical sensations of orgasm. Pelvic floor muscle relaxation results in a decrease or termination of the
squeezing of the urethra, vagina and anus. The perineum and the pelvic organs return to their anatomical
resting position. Relaxation of the pelvic floor muscles is needed for voiding, defecation and for sexual
intercourse. The muscles of the pelvic floor are integrated in the total muscular girdle of the pelvis, yielding the
stability needed for bearing the trunk. Instability in its turn leads to compensatory pelvic floor muscle (over)
activity.
9.3 Dysfunction
Pelvic floor dysfunction should be classified according to “The standardisation of terminology of pelvic floor
muscle function and dysfunction” (1). This is an international multidisciplinary report from the International
Continence Society. By palpation of the pelvic floor muscles, the contraction and relaxation are qualified.
Voluntary contraction can be absent, weak, normal or strong, and voluntary relaxation can be absent, partial or
complete. Involuntary contraction and relaxation is absent or present.
Based on these signs, pelvic floor muscles can be classified as follows:
• non-contractingpelvicfloor
• non-relaxingpelvicfloor
• non-contracting,non-relaxingpelvicfloor.
Based on symptoms and signs, the following conditions are possible:
• normalpelvicfloormuscles

UPDATE FEBRUARY 2012 117
• overactivepelvicfloormuscles
• underactivepelvicfloormuscles
• non-functioningpelvicfloormuscles.
Normal pelvic floor muscles relax during urination and contract during coughing. Overactive pelvic
floor muscles do not relax during micturition, defecation or during sex and cause dysfunctional voiding,
overactive bladder, constipation and dyspareunia (2). Underactive pelvic floor muscles do not contract
sufficiently to keep the patient dry. Non-functioning pelvic floor muscles do not show any activity whatsoever
and can cause every type of pelvic organ dysfunction.
Overactivity tends to develop over a protracted period, with many causes. A psychological mechanism
that is thought to play a role is that contraction of the pelvic floor muscles closes some of the exits of the body
(anus and vagina), and helps to keep urine and stool inside. It gives women a defence mechanism against
unwanted vaginal penetration of any type. The pelvic floor muscles also help to postpone micturition, which
can be of benefit in a social or working environment. In summary, the pelvic floor muscles assist in adaptation
to different situations in life.
9.4 Pelvic floor muscles and myofascial pain
Chronic pelvic pain can simply be a form of myalgia, due to misuse of muscles, in this case, the pelvic floor
muscles. Studies in the field of chronic prostatitis support the idea that patients with CPP have more muscle
spasm and increased muscle tone and pain when palpating the pelvic floor muscles (3). Muscle relaxation can
diminish spasm and pain (4). Repeated or chronic muscular overload can activate trigger points in the muscle.
A report from the Chronic Prostatitis Cohort Study showed that 51% of patients with prostatitis and only 7% of
controls had any muscle tenderness. Tenderness in the pelvic floor muscles was only found in the CPP group
(5).
9.4.1 Muscular aspects
The relationship between muscular dysfunction (especially overactivity) and pelvic pain has been found in
several studies. Rectal pain treated with pelvic floor muscle therapy is only relieved when patients learn to
relax their pelvic floor muscles (6). The vast majority (92.2%) of men visiting a tertiary centre for pelvic pain
had dysfunction of the pelvic floor muscles. This finding was true regardless of evidence of inflammation
(prostatitis or cystitis) (7). This relationship has been found in chronic prostatitis (8), BPS (9) and vulvar pain
(10). Dysfunction of the pelvic floor directly affects function of the pelvic viscera and vice versa. Both systems
can act as the primary signal to the spinal cord, with a cascade of reactions ascending to the CNS as a result.
The muscle itself ends up with a diminished length, leading to restrictions even when it is in a relaxed state.
9.4.2 Neurological aspects
In 1999, the first ideas about the neurological aspects of the pelvic floor muscles in relation to CPP were
published. The probability of CNS breakdown in the regulation of pelvic floor function was suggested as a
mechanism for development of CPP. Of the patients presenting with pelvic pain, 88% had poor to absent
pelvic floor function (11). Basic studies on the role of neurogenic inflammation have also elucidated some
important phenomena. Irritation of the prostate, bladder and pelvic floor muscles results in expression of C-fos-
positive cells in the CNS. There appears to be convergence of afferent information onto central pathways.
Once the central changes have become established, they become independent of the peripheral input that
initiated them (12).
9.4.3 Myofascial trigger points
Repeated or chronic muscular overload can activate trigger points in the muscle. Trigger points are defined as
hyperirritable spots within a taut band. Other criteria for trigger points are: recognition of the pain as ‘familiar’,
and pain on stretching the muscle. Apart from pain, trigger points prevent full lengthening of the muscle,
thereby restricting the range of movement. Pain as a result of these trigger points is aggravated by specific
movements and alleviated by certain positions. Positions and movements in which the shortened muscle is
stretched are painful. Patients know which activities and postures influence pain. Trigger points can be located
within the pelvic floor muscles and in adjacent muscles such as the abdominal, gluteal and ileopsoas muscles.
Pain is aggravated by pressure on the trigger point (e.g., pain related to sexual intercourse). Pain also worsens
after sustained or repeated contractions (e.g., pain related to voiding or defecation).
9.5 Diagnostics of pelvic floor muscle function
Diagnosing pelvic floor muscle function in patients with CPP starts by taking a complete functional history
of the pelvic organ function. The following items certainly should be addressed: lower urinary tract function,
anorectal function, sexual function, gynaecological items, presence of pain and psycho-social aspects.

118 UPDATE FEBRUARY 2012
9.5.1 Physical examination
After taking a history, physical examination should be done. Special attention must be paid to the abdominal,
inguinal and genital areas, but also to the pelvic alignment. The patient should be asked to point at the location
of maximal pain and at the secondary pain points. Palpation of the abdomen with special attention to the
muscles may yield pain points that are important for making a treatment plan. A vaginal or rectal examination
should be performed to assess the function of the pelvic floor muscles, according to the ICS report. This
assessment has been tested and shows satisfactory face validity and intra-observer reliability. It can therefore
be considered suitable for use in clinical practice (13). Rectal examination is a good way to test the pelvic floor
muscle function in men (14).
9.5.2 Electromyography and pressure measurement (EMG)
Additional examination can be done using electromyography. This is preferably done using an intravaginal or
intra-anal probe. This measures the electrical activity of the pelvic floor muscles as a group. It does not reveal
anything about the efficacy of the contraction or relaxation. There is good correlation between digital palpation
and intravaginal surface EMG (15). To measure the effect of pelvic floor muscle contraction, a pressure probe
can be used. The measurement of anal pressure is reliable (16), Performance of EMG in different positions
gives more insight into the properties of the pelvic floor. EMG is one of the most used input methods for
biofeedback. Intraluminal pressure can also be used for this purpose.
9.5.3 Imaging
Anatomical imaging of the pelvic floor muscles can be done using MRI. It is still debatable whether MRI can
be of help in diagnosing pudendal entrapment. Functional imaging can be done using techniques such as
video-urodynamics (pelvic floor muscles in relation to bladder function) or defecography (pelvic floor muscles
in relation to defecation). The reason for this is to exclude disease-specific pain. Repeated imaging studies may
be detrimental for the patient because they emphasise somatic causes of the pain.
9.5.4 Myofascial trigger points
There is no accepted reference standard for the diagnosis of trigger points. Data on the reliability of physical
examination are conflicting. Reliability is relatively good for tenderness and for recognisable referred pain. It is
lower for taut band recognition and local twitch response. The reliability improves when examination is done by
experts, who are specially trained in diagnosing trigger points. Other techniques are used for diagnosing trigger
points but none have become standard. Among these are imaging techniques and EMG (17).
In a cohort study of 72 men with CPP, the relationship between the locations of the trigger point and
the referred pain was examined. Ninety percent of the patients showed tenderness in the puborectalis muscle
and 55% in the abdominal wall muscles. Of the patients in whom trigger points were found in the puborectalis,
93% reported pain in the penis and 57% in the suprapubic region. Patients with trigger points in the abdominal
muscles reported pain in the penis (74%), perineum (65%) and rectum (46%) (18).
9.6 Treatment of pelvic floor muscle pain
Treating pelvic floor overactivity and myofascial trigger points should be considered in the management
of CPP. Treatment should be done by specialised physiotherapists who are trained not only in the
musculoskeletal aspects of pain, but also in the psychological mechanisms and the role of the CNS in chronic
pain.
9.6.1 Pelvic floor muscle exercise
For patients with CPP and dysfunction of the pelvic floor muscles, it is very helpful to learn how to relax the
muscles when the pain starts. By doing this, the circle of pain-spasm-pain can be interrupted. In the case of
shortened muscles, relaxation alone is not enough. Stretching of the muscle is mandatory to regain length and
function. Studies on physical therapy for pelvic floor pain syndrome have been sparse. A single blinded RCT
with myofascial physical therapy and general massage was carried out in patients with prostate or bladder
pain. The global response rate to treatment with massage was significantly better in the prostate than in
the bladder pain group (57% vs. 21%). In the prostate pain group, there was no difference between the two
treatment arms. In the bladder pain group, myofascial treatment did significantly better than the massage.
Massage only improved complaints in the prostate pain group. The fact that the prostate pain group consisted
of only men is mentioned as a possible confounding factor (19).
9.6.2 Biofeedback and electrostimulation
Biofeedback can be helpful in the treatment of pelvic floor pain in the process of recognising the action of
the muscles. Visualising the action of the pelvic floor muscles by using biofeedback is an eye opener to many
patients. Biofeedback should always be used in consultation with the patient. Special care should be taken

UPDATE FEBRUARY 2012 119
when there is a history of negative physical or sexual experiences. The numbers of patients in most studies
concerning biofeedback have been small but the results are promising. In a cohort study, 31 patients with
CPPS participating in a pelvic floor biofeedback re-education programme were followed. The mean chronic
prostatitis symptom index decreased from 23.6 to 11.4. They also measured the pelvic floor muscle activity
by EMG using an anal probe. The resting amplitude was taken as a parameter for the ability to relax the pelvic
floor muscles. This parameter was 4.9 μV at the start and 1.7 μV at the end of the treatment, so the relaxation
improved markedly. There was also a correlation between the decline in EMG values and improvement in
prostatitis symptom score (20).
In a study among patients with levator ani syndrome, biofeedback was found to be the most effective
therapy. Other modalities used were electrostimulation and massage. Adequate relief was reported by 87%
in the biofeedback group, 45% for electrostimulation, and 22% for massage (6). A review on biofeedback in
pelvic floor dysfunction has shown that biofeedback is better than placebo or sham treatment. An odds ratio of
5.8 favouring biofeedback has been calculated based on three studies (21).
9.6.3 Myofascial trigger point release
The treatment of myofascial trigger points has different options. There are three groups of treatment: (1) manual
therapy: pressure and release, compression, spray and stretch; (2) dry needling: putting a solid filiform needle
directly in the trigger point, repeatedly and in an up and down pecking motion; and (3) wet needling: injection
of lidocaine or botulinum toxin into the trigger point. The evidence for all the different treatments is weak. In
most studies, no significant difference between these techniques has been found. One problem is that most
of the studies were small and heterogeneous with regard to the patients and methods. This is especially true
for comparing any technique with sham or placebo treatment. For manual therapy, central trigger points are
treated by stretching the muscle because this inactivates it. Trigger points lying in the attachment of the muscle
to the bone are treated using direct manual therapy. Other well-known techniques such as biofeedback and
neuromuscular stimulation have been used in the treatment of trigger points. There is no evidence that manual
techniques are more effective than no treatment (22). In most studies of dry needling, it has been compared
with wet needling. Different systematic reviews have come to the conclusion that, although there is an effect
of needling on pain, it is neither supported nor refuted that this effect is better than placebo (23). Other reviews
have concluded that the same is true for the difference between dry and wet needling (24,25).
9.6.4 Botulinum A toxin
Botulinum A toxin (BTX-A) is an inhibitor of acetylcholine release at the neuromuscular junction and has a
paralysing effect on striated muscles. BTX-A has been injected into trigger points. It is more expensive than
lidocaine and has not been proven to be more effective (26). Reviews do not support the injection of BTX-A into
trigger points (27).
Pelvic floor muscle overactivity plays a role in CPP. BTX-A, as a muscle relaxant, can be used to
reduce the resting pressure in the pelvic floor muscles. In women with high resting pressure in the pelvic
floor muscles, it has been found that BTX-A lowers this pressure significantly. The magnitude of reduction
was significantly higher than that in the placebo group. On the pain score (VAS), no intergroup differences
were found in this relatively small randomised study (28). BTX-A can also be injected at the sphincter level
to improve urination or defecation. Relaxation of the urethral sphincter alleviates the bladder problems and
secondarily the spasm. In a cohort study of 13 patients with CPP, BTX-A was injected into the external urethral
sphincter. Subjectively, 11 patients reported a substantial change in pain symptoms, from 7.2 to 1.6 on a visual
analogue scale (29).
9.6.5 Pain management
The physiotherapist is part of the pain management team, together with the pain doctor and the psychologist.
The therapeutic options for physiotherapists may not be the same in every country. Physiotherapists can either
specifically treat the pathology of the pelvic floor muscles, or more generally treat myofascial pain if it is part of
the pelvic pain syndrome.
9.7 Conclusions and recommendations: pelvic floor function
Conclusions LE
The ICS classification is suitable for clinical practice. 2a
Overactivity of the pelvic floor muscles is related to chronic pelvic pain, prostate, bladder and vulvar
pain.
2a
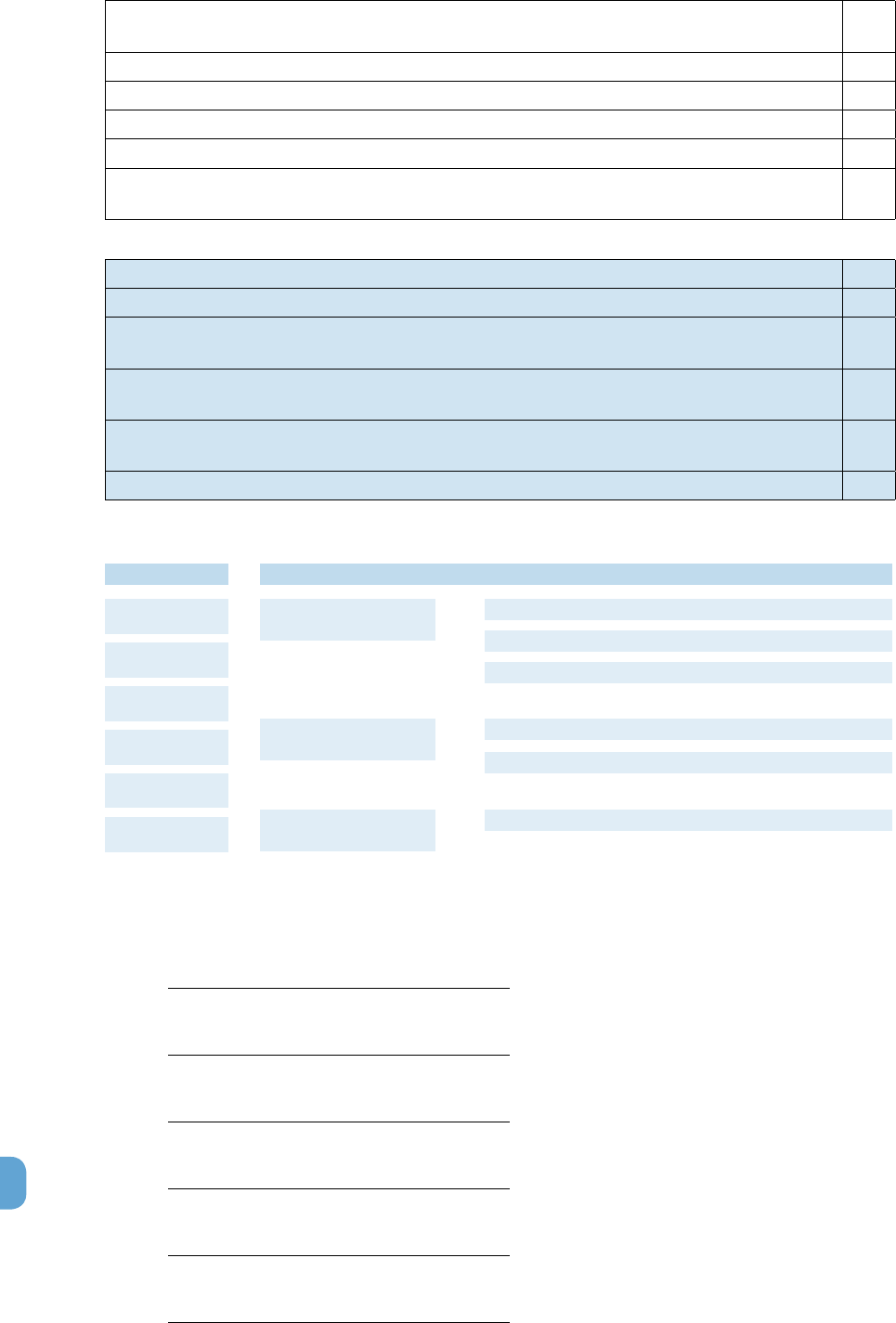
120 UPDATE FEBRUARY 2012
The overactivity of the pelvic floor muscles is an input to the central nervous system causing central
sensitisation.
2b
There is no accepted standard for diagnosing myofascial trigger points. 2a
There is a relation between the location of trigger point and the region where the pain is perceived. 3
Myofascial treatment is effective in prostate- and bladder pain syndrome. 1b
Biofeedback improves the outcome of myofascial therapy for pelvic floor dysfunction. 1a
Trigger point release is effective in treating muscle and referred pain, but there is no preference from
one method over another.
1a
Recommendations GR
The use of the ICS classification on pelvic floor muscle function and dysfunction is recommended. A
In patients with chronic pelvic pain syndrome it is recommended to actively look for the presence of
myofascial trigger points.
B
In patients with chronic pelvic pain syndrome it is recommended to apply pelvic floor muscle
treatment as first line treatment.
B
In patients with an overactive pelvic floor biofeedback is recommended as therapy adjuvant to
muscle exercises.
A
When myofascial trigger points are found treatment by pressure or needling is recommended. A
Figure 17: assessment and treatment pelvic floor function
9.8 References
1. Messelink EJ, Benson T, Berghmans B et al. Standardisation of terminology of pelvic floor muscle
function and dysfunction: report from the pelvic floor clinical assessment group of the International
Continence Society. Neurourol Urodyn. 2005;24(4):374-80.
http://www.ncbi.nlm.nih.gov/pubmed/15977259
2. Messelink EJ. The overactive bladder and the role of the pelvic floor muscles. BJU Int 1999
Mar;83Suppl 2:31-5.
http://www.ncbi.nlm.nih.gov/pubmed/10210602
3. Hetric DC, Ciol MA, Rothman I, et al. Musculoskeletal dysfunction in men with chronic pelvic pain
syndroime type III: a case-control study. J Urol. 2003 Sep;170(3):828-31.
http://www.ncbi.nlm.nih.gov/pubmed/12913709
4. Clemens JQ, Nadler RB, Schaeffer AJ, et al. Biofeedback, pelvic floor re-education, and bladder
training for male chronic pelvic pain syndrome. Urology. 2000 Dec 20;56(6):951-5.
http://www.ncbi.nlm.nih.gov/pubmed/11113739
5. Shoskes DA, Berger R, Elmi A.,et al. Muscle tenderness in Men with Chronic Prostatitis/Chronic Pelvic
Pain syndrome: The Chronic Prostatitis Cohort Study. J Urol. 2008 Feb;179(2):556-60
http://www.ncbi.nlm.nih.gov/pubmed/18082223
6. Chiarioni G, Nardo A, Vantini I, et al. Biofeedback Is Superior to Electrogalvanic Stimulation and
Massage for Treatment of Levator Ani Syndrome. Gastroenterology. 2010 Apr;138(4):1321-9.
http://www.ncbi.nlm.nih.gov/pubmed/20044997
Palpation of the
muscles
Testing of pelvic
floor function
Pelvic floor muscle
EMG
Test for myofascial
Trigger points
Standardised
questionnaires
Assessment
Grade A recommended
History of all the
involved organs
Treatment
Grade B recommended
Other comments
Use the International Continence Society classification of dysfunction
Use biofeedback in combination with muscle exercises
Look actively for the presence of myofascial trigger points
Apply pelvic floor muscle therapy as first line treatment
Treat myofascial trigger points using pressure or needling
The role and options of a physiotherapist may differ between countries

UPDATE FEBRUARY 2012 121
7. Zermann DH, Ishigooka M, Doggweiler R, Schmidt RA. Chronic prostatitis: a myofascial pain
syndrome? Infect Urol 1999;12:84-6.
8. Shoskes DA, Berger R, Elmi A, et al. Muscle tenderness in Men with Chronic Prostatitis/Chronic Pelvic
Pain syndrome: The Chronic Prostatitis Cohort Study. J Urol. 2008 Feb;179(2):556-60.
http://www.ncbi.nlm.nih.gov/pubmed/18082223
9. Peters KM. Prevalence of Pelvic floor dysfunction in patients with Interstitial Cystitis. Urology. 2007
Jul;70(1):16-8.
http://www.ncbi.nlm.nih.gov/pubmed/17656199
10. Reissing ED, Brown C, Lord MJ, et al. Pelvic floor muscle functioning in women with vulvar vestibulitis
syndrome. J Psychosom Obstet Gynaecol. 2005 Jun;26(2):107-13.
http://www.ncbi.nlm.nih.gov/pubmed/16050536
11. Zermann DH, Ishigooka M, Doggweiler R, et al. Neurourological insights into the etiology of
genitourinary pain in men. J Urol. 1999 Mar;161(3):903-8.
http://www.ncbi.nlm.nih.gov/pubmed/10022711
12. Ishigooka M, Zermann DH, Doggweiler, et al. Similarity of distributions of spinal C-fos and
plasma extravasation after acute chemical irritation of the bladder and the prostate. J Urol. 2000
Nov;164(5):1751-6.
http://www.ncbi.nlm.nih.gov/pubmed/11025764
13. Slieker-ten Hove MC, Pool-Goudzwaard AL, Eijkemans MJ, et al. Face validity and reliability of the first
digital assessment scheme of pelvic floor muscle function conform the new standardized terminology
of the International Continence Society. Neurourol Urodyn. 2009;28(4):295-300.
http://www.ncbi.nlm.nih.gov/pubmed/19090583
14. Wydaele JJ, Van Eetvelde B. Reproducibility of digital testing of the pelvic floor muscles in men. Arch
Phys Med Rehabil. 1996 Nov;77(11):1179-81.
http://www.ncbi.nlm.nih.gov/pubmed/8931532
15. Romanzi LJ, Polaneczky M, Glazer HI. Simple test of pelvic muscle contraction during pelvic
examination: correlation to surface electromyography. Neurourol Urodyn. 1999;18(6):603-12
http://www.ncbi.nlm.nih.gov/pubmed/10529708
16. Dorey G, Swinkels A. Test Retest Reliability of Anal Pressure Measurements in Men with Erectile
Dysfunction. Urol Nurs. 2003 Jun;23(3):204-12.
http://www.ncbi.nlm.nih.gov/pubmed/12861738
17. Lucas N, Macaskill P, Irwig L, et al. Reliability of physical examination for diagnosis of myofascial
trigger points: a systematic review of the literature. Clin J Pain. 2009 Jan;25(1):80-9.
http://www.ncbi.nlm.nih.gov/pubmed/19158550
18. Anderson RU, Sawyer T, Wise D, et al. Painful myofascial trigger points and pain sites in men with
chronic prostatitis/chronic pelvic pain syndrome. J Urol. 2009 Dec;182(6):2753-8.
http://www.ncbi.nlm.nih.gov/pubmed/19837420
19. FitzGerald MP, Anderson RU, Potts J, et al. Randomized multicenter feasibility trial of myofascial
physical therapy for the treatment of urological chronic pelvic pain syndromes. J Urol. 2009
Aug;182(2):570-80.
http://www.ncbi.nlm.nih.gov/pubmed/19535099
20. Cornel EB, van Haarst EP, Schaarserg RW, et al. The effect of biofeedback physical therapy in men
with chronic pelvic pain syndrome type III. Eur Urol. 2005 May;47(5):607-11.
http://www.ncbi.nlm.nih.gov/pubmed/15826751
21. Koh CE, Young CJ, Young JM, et al. Systematic review of randomized controlled trials of the
effectiveness of biofeedback for pelvic floor dysfunction. Br J Surg. 2008 Sep;95(9):1079-87.
http://www.ncbi.nlm.nih.gov/pubmed/18655219
22. de las Penas CF, Sohrbeck Campo M, Fernandez Carnero J, et al. Manual therapies in myofascial
trigger point treatment: a systematic review.
23. Tough EA, White AR, Cummings TM, et al. Acupuncture and dry needling in the management of
myofascial trigger point pain: a systematic review and meta-analysis of randomised controlled trials.
Eur J Pain. 2009 Jan;13(1):3-10.
http://www.ncbi.nlm.nih.gov/pubmed/18395479
24. Cummings TM, White AR. Needling therapies in the management of myofascial trigger point pain: a
systematic review. Arch Phys Med Rehabil. 2001 Jul;82(7):986-92.
http://www.ncbi.nlm.nih.gov/pubmed/11441390
25. Scott NA, Guo B, Barton PM, et al. Trigger point injections for chronic non-malignant musculoskeletal
pain: a systematic review. Pain Med. 2009 Jan;10(1):54-69.
http://www.ncbi.nlm.nih.gov/pubmed/18992040

122 UPDATE FEBRUARY 2012
26. Kamanli A, Kaya A, Ardicoglu O, et al. Comparison of lidocaine injection, botulinum toxin injection, and
dry needling to trigger points in myofascial pain syndrome. Rheumatol Int. 2005 Oct;25(8):604-11.
http://www.ncbi.nlm.nih.gov/pubmed/15372199
27. Ho KY, Tan KH. Botulinum toxin A for myofascial trigger point injection: a qualitative systematic
review. Eur J Pain. 2007 Jul;11(5):519-27.
http://www.ncbi.nlm.nih.gov/pubmed/17071119
28. Abbott JA, Jarvis SK, Lyons SD, et al. Botulinum toxin type A for chronic pain and pelvic floor spasm
in women: a randomized controlled trial. Obstet Gynecol. 2006 Oct;108(4):915-23.
http://www.ncbi.nlm.nih.gov/pubmed/17012454
29. Zermann D, Ishigooka M, Schubert J, et al. Perisphincteric injection of botulinum toxin type A.
A treatment option for patients with chronic prostatic pain? Eur Urol. 2000 Oct;38(4):393-9.
http://www.ncbi.nlm.nih.gov/pubmed/11025376
10. GENERAL TREATMENT OF CHRONIC PELVIC
PAIN
10.1 Introduction
Chronic pelvic pain (CPP) is well defined and involves multiple mechanisms as described in previous chapters.
The management requires a holistic approach with biological, psychological and social components. This
chapter looks solely at general treatments and should be used as part of a management plan including the
interventions suggested in the specific chapters.
Despite the developments in basic science, there has not been the same in pharmacological intervention. It is
recognised that there are often central mechanisms involved in CPP. This chapter looks at general treatments
for pain (both peripheral and central) and not the specific treatments mentioned in the chapters 2 and 6.
Despite the frequency of CPP, relatively few studies have specifically looked at the medications used in CPP
patients (1). As a result, a wider look at the literature has been undertaken, including the agents used for central
and neuropathic pain. Further specific research is required in this group of patients.
The agents concerned are divided for ease of description. Combinations often provide a greater
benefit than individual agents. They may also allow lower dosages of each agent and thus minimise the side
effects.
The aim of using these drugs is to allow patients to improve their QoL. This is best measured by
assessing their function as well as pain severity. If the addition of these agents does not allow this, then they
should be withdrawn. Unfortunately, the failure of one agent to provide benefit does not mean that there is
an alternative. If the benefit is limited by side effects, then the lowest effective dose should be found (by dose
titration). In some circumstances, patients can tolerate a higher level of pain and have fewer side effects.
If the use of simple analgesics fails to provide adequate benefit, then one should consider using the
neuropathic agents, and if there is no improvement, consider involving a specialist pain management centre
with an interest in pelvic pain.
10.2 Simple analgesics
Paracetamol (acetaminophen)
Paracetamol is a well-tolerated analgesic in a class of its own. This is an antipyretic analgesic with a central
mechanism of action (2). It is often available over the counter without prescription. There is evidence that
paracetamol is beneficial in managing somatic and arthritic pain. (3-5). There is little evidence for its use in CPP
but it should be considered if it has not already been tried.
Non-steroidal anti-inflammatory agents (NSAIDs)
This is a group of agents that include salicylic acid. They have had significant publicity over recent years. They
are anti-inflammatory, antipyretic analgesics that act by inhibiting the enzyme cyclo-oxygenase (COX). They
have a peripheral effect, hence their use in painful conditions involving peripheral or inflammatory mechanisms.
They are commonly used for pelvic pain because many are available over the counter and are usually
well tolerated. The evidence for their benefit is often weak or non-existent. It should be remembered that they
do have side effects, which may be significant. There is no good evidence to suggest one NSAID over another
for pelvic pain.

UPDATE FEBRUARY 2012 123
For pelvic pain in which inflammatory processes are considered to be involved, such as dysmenorrhoea (6),
NSAIDs are more effective than placebo and paracetamol, but with a higher incidence of side effects. For
pelvic pain in which central mechanisms may be incriminated, such as endometriosis (7), then the evidence is
lacking for NSAIDs despite their common use.
Guidelines for use of NSAIDs and COX-2 selective agents have been developed. They have more side effects
than paracetamol, including indigestion, headaches and drowsiness.
At a practical level, NSAIDs could be considered as analgesics for patients with pelvic pain. They
should be tried (having regard for the cautions and contraindications for use) and the patient reviewed for
improvement in function as well as analgesia. If this is not achieved, or there are side effects, then the NSAID
should be stopped.
Neuropathic analgesics
This is a group of agents that are not simple analgesics but are used to modulate neuropathic or centrally
mediated pain. There are several classes used with a recognised benefit in pain medicine. They are taken on a
regular basis rather than as required. They all have side effects that limit their use in some patients.
In the UK, the National Institute for Health and Clinical Excellence (NICE) has reviewed the pharmacological
management of neuropathic pain (8). There is further guidance in progress for the management of neuropathic
pain in the non-specialist setting.
Not all the agents have a licence for use in pain management but there is a history and evidence to
demonstrate their benefit. The evidence for treatment of CPP is lacking but is present for other painful
conditions. For this chapter, most of the evidence is from non-pelvic pain sources.
The general method for using these agents is by titrating the dose against benefit and side effects.
The aim is for patients to have an improvement in their QoL, and is often best assessed by alterations in their
function. Side effects frequently limit the use of these agents.
It is common to use these agents in combinations but studies comparing different agents against each
other or in combination are lacking.
10.2.1 Antidepressants
10.2.1.1 Tricyclic antidepressants
This is a group of drugs with multiple mechanisms of action. They have a long history of use in pain medicine
and have been subjected to a Cochrane review (9). This suggests that they are effective for neuropathic pain
with numbers needed to treat (NNT) of approximately three.
Amitriptyline is the most commonly used member of this group at doses from 10 to 75 mg/day (sometimes
rising to 150 mg/day). This is titrated against benefit or side effects and taken at night (8). Nortriptyline and
imipramine are often used as alternatives.
10.2.1.2 Other antidepressants
Venlafaxine is a serotonin and noradrenalin reuptake inhibiter (SNRI). It does not have a license for managing
neuropathic pain but there is evidence of its benefit in chronic pain (8). There are cautions particularly in
patients with heart disease. This is a drug best used by those familiar with its use.
Duloxetine is a newer SNRI antidepressant. It is used for depression, urinary stress incontinence and
neuropathic pain. There is moderately strong evidence for a benefit in diabetic neuropathy and fibromyalgia at
a dose of 60 mg/day (10). Side effects are common and may result in its discontinuation.
Selective serotonin reuptake inhibitors (SSRIs) are antidepressants with fewer side effects. They are effective
for depression but there have been insufficient studies to demonstrate their benefit in pelvic or neuropathic
pain (9,11,12).
10.2.2 Anticonvulsants
This group of drugs are commonly used in the management of neuropathic pain. There have been general
studies as well as some looking more particularly at pelvic pain. Individual agents have been systematically
reviewed. Their use is suggested in the NICE Neuropathic Guidelines (8).
Carbamazepine has a long history of use in neuropathic pain. Evidence exists for its benefit (13). It should be
remembered that the trials have tended to be of short duration, showing only moderate benefit. There are side

124 UPDATE FEBRUARY 2012
effects; some of which may be serious. With more recently developed agents becoming available, with fewer
serious side effects, carbamazepine is no longer a first-choice agent.
Gabapentin is commonly used for neuropathic pain and has been systematically reviewed (14).
It provides good quality relief with NNT of approximately six. This is a more conservative estimate than in
previous reports. Side effects are common, notably drowsiness, dizziness and peripheral oedema. These
effects do limit compliance but are often tolerated by patients. The doses involved were all greater than 1.2 g/
day. For upper dose levels, reference should be made to local formularies, and many clinicians do not routinely
exceed 2.4g/day in divided doses (most commonly three times daily).
One study of women with CPP has suggested that gabapentin alone or in combination with
amitriptyline provides better analgesia then amitriptyline alone (15).
Pregabalin is another commonly used neuromodulator. There is good evidence for its efficacy in some
neuropathic conditions but the NNT varies depending on the condition (16). The dose for benefit is in the range
of 300 to 600 mg/day. The same systematic review has found that doses less than 150 mg/day are unlikely to
provide benefit. As with gabapentin, side effects are relatively common and may not be tolerated by patients.
Other anticonvulsants are available but not commonly used for managing pain.
10.2.3 Other agents
Other agents can be used in the management of neuropathic pain but are best limited to those that are
specialists in the management of pain and familiar with their use. They tend to be considered after the standard
options have been exhausted. As with all good pain management, they are used as part of a comprehensive
management plan.
Topical capsaicin has been used for neuropathic pain either by repeated low-dose (0.075%) administration or
more recently as a single high dose (8%). Topical application (usually to an area of hyperaesthesia or allodynia)
is more inconvenient than for other medications, and capsaicin does cause initial heat on application. Skin
sensitivity is a limiting factor and may not be well tolerated. A systematic review has suggested there may be
benefit in some patients (17). Care should be taken to ensure that unused cream or that washed off the hands
following application is not inadvertently transferred to other areas of skin or mucous membranes.
Antipsychotics have been used and despite limited research, a systematic review has suggested that further
research should be undertaken on the atypical antipsychotics, which have fewer side effects and are better
tolerated than the older antipsychotics (18).
10.3 Opioids
Opioids are used for chronic non-malignant pain and may be beneficial for a small number of patients. Often
patients will stop taking oral opioids due to side effects or insufficient analgesia (19).
They should only be used in conjunction with a management plan and with consultation between
clinicians experienced in their use. It is suggested that a pain management unit should be involved along with
the patient and their primary care physician.
There are well established guidelines for the use of opioids in pain management as well as considering the
potential risks (20). There is also information available on line for patients (21,22).
Opioid rotation is used in palliative care and to some extent in non-cancer pain. The evidence is clinical, largely
anecdotal, or from small trials and is not convincing (23). The rational is that if a patient has significant side
effects and inadequate analgesia to one opioid then swapping to another agent may be better tolerated.
There are several agents available in the group. They can be divided into weak (e.g., codeine, dihydrocodeine
and tramadol) or strong opioids (e.g., morphine, oxycodone, fentanyl and hydromorphone).
Oral administration is preferable, but if poorly tolerated, a percutaneous (patch) route may have advantages.
More invasive approaches are less commonly used and within the realms of specialist units.
Side effects are common and require active management. This is particularly true of constipation with some
interesting developments on methods for managing it.
There is a growing understanding of opioid-induced hyperalgesia (24); a situation in which patients taking
opioids, paradoxically, become more sensitive to painful stimuli. This is another reason for these drugs to be
used in a controlled fashion for long-term management of non-malignant pain.

UPDATE FEBRUARY 2012 125
10.4.1 Recommendations for use of opioids in chronic/non-acute urogenital pain
Recommendations
All other reasonable treatments must have been tried and failed.
The decision to instigate long-term opioid therapy should be made by an appropriately trained specialist in
consultation with another physician (including the patients and their family doctor).
Where there is a history or suspicion of drug abuse, a psychiatrist or psychologist with an interest in pain
management and drug addiction should be involved.
The patient should undergo a trial of opioids.
The dose required needs to be calculated by careful titration.
The patient should be made aware (and possibly give written consent):
• Thatopioidsarestrongdrugsandassociatedwithaddictionanddependency.
• Opioidswillnormallyonlybeprescribedfromonesource(preferablythefamilydoctor).
• Thedrugswillbeprescribedforfixedperiodsoftimeandanewprescriptionwillnotbeavailable
until the end of that period.
• Thepatientmaybesubjectedtospoturineandpossiblybloodcheckstoensurethatthedrugis
being taken as prescribed, and that non-prescribed drugs are not being taken.
• Inappropriateaggressivebehaviourassociatedwithdemandingthedrugwillnotbeaccepted.
• Hospitalspecialistreviewwillnormallyoccuratleastonceayear.
• Thepatientmayberequestedtoattendapsychiatric/psychologicalreview.
Failure to comply with the above may result in the patient being referred to a drug dependency agency and
the use of therapeutic, analgesic opioids being stopped.
Morphine is the first-line drug, unless there are contraindications to morphine or special indications for
another drug.
• Thedrugshouldbeprescribedinaslow-release/modifiedreleaseform.
• Short-actingpreparationsareundesirableandshouldbeavoidedwherepossible.
• Parenteraldosingisundesirableandshouldbeavoidedwherepossible.
10.4.2 Morphine
There is no compelling evidence that one opioid is better than another. Morphine is the traditional gold
standard and the opioid with which many physicians are most familiar. The aim is to use a slow or sustained
release preparation starting with a low dose and titrating the dose every 3 days to 1 week against improvement
in both function and pain. Side effects should also be monitored and managed accordingly. Particular attention
should be paid to the management of constipation.
10.4.3 Other opioid agents
There are a variety of agents available and some are mentioned below, giving an idea of the options available.
Transdermal fentanyl may be considered when oral preparations are restricted (e.g., iliostomy). It may also be
beneficial when there are intolerable side effects from other opioids.
Methadone has a long record of use as an opioid. There is a theoretical advantage of benefit with its N-methyl-
D-aspartate receptor (NMDA) antagonist activity. This may be particularly relevant in neuropathic pain (25).
Oxycodone may have greater efficacy than morphine in some situations, such as hyperalgesic states including
visceral pain (26).
Analgesics with a dual mode of action may have a role in the management of chronic pain. Tramadol is an
established analgesic with dual effects on opioid receptors and serotonin release. More recently, a new agent,
tapentadol, has been released with opioid action and noradrenalin reuptake inhibition. It is too early to assess
its real value in the armamentarium for pain management.
10.5 Nerve blocks
Nerve blocks for pain management are usually carried out by specialists in pain medicine and as part of a
broader management plan (27). They may have a diagnostic or therapeutic role.
Textbooks have been written on the subject and practioners using them should be trained in appropriate
patient selection, indications, risks and benefits. Many such interventions also require understanding and

126 UPDATE FEBRUARY 2012
expertise in using imaging techniques to perform the blocks accurately.
Diagnostic blocks can be difficult to interpret due to the complex nature of the mechanisms underlying the
painful condition or syndrome. Sustained but limited benefit may lead to more permanent procedures (e.g.,
neurolytic block or radiofrequency procedures). Neurolytic blocks in particular should only be considered by
practioners experienced in their use and with the full understanding of the patient because complications can
be disastrous.
There is a weak evidence base for these interventions for chronic non-malignant pain.
10.6 Transcutaneous electrical nerve stimulation (TENS)
Despite the popularity of TENS and the number of trials undertaken, a systematic review has been unable
to provide an evidence base for this technique (28). It is clear that further more rigorous trials should be
undertaken to provide some clarity for a commonly used intervention.
10.7 Neuromodulation in pelvic pain syndromes
The role of neuromodulation in the management of pelvic pain should only be considered by specialists in
pelvic pain management. These techniques are only used as part of a broader management plan and require
regular follow-up.
The research base is developing and the techniques broadening [e.g., spinal cord stimulation (SCS), sacral root
stimulation, dorsal root ganglion stimulation or peripheral nerve stimulation]. These are expensive interventions
and thus many of the patients involved are refractory to other therapies. It is thus inappropriate to provide a
detailed review of these techniques for this publication.
In the UK, guidance has been published for SCS in neuropathic pain (29). This emphasises the comments
above. This guidance suggests a trial period of stimulation before full implementation.
Neuromodulation is still finding its role in pelvic pain management. There has been growing evidence in small
case series or pilot studies but more detailed research is required (30). Its role in overactive bladder and faecal
incontinence is more robust but is limited for pain.
10.8 Summary
Chronic pelvic pain is a common complaint that is well defined and involves multiple mechanisms. Some
of the conditions have clear management pathways but many do not. In these CPP syndromes, a holistic
multidisciplinary team approach is required with active patient involvement.
This chapter focuses on general treatment of CPP, mainly drug therapy, and comments on other more invasive
techniques. The latter are used in combination with other modalities. Many are aimed at management of
neuropathic pain or conditions in which central mechanisms are implicated.
At this stage in management, the involvement of trained clinicians with expertise in chronic pain management
should be considered. Centres with a particular interest in pelvic pain do exist and involve clinicians from
several specialties along with other health care professionals (e.g., physiotherapy, psychology, nursing and
occupational therapy).
With any of the agents above, the aim is to assess pain relief, improvement in function, and side effects. This
should be done regularly while titrating and optimising drug dose. If there is no benefit, then the drug should be
withdrawn.
Neuropathic agents are frequently used and often in combination. There is significant inter-patient variability in
effect. Use is often limited by side effects that may be worse than any pain reduction.
Opioid drugs are used in this group of patients. Their role is limited and they should only be started in
consultation with all parties involved (including the patient’s family practitioner). National guidelines exist and
should be followed. There is growing understanding of the limitations of opioid use, and more recently, the
paradoxical situation of opioid-induced hyperalgesia.

UPDATE FEBRUARY 2012 127
10.9 Recommendations for the medical treatment of CPP
Agent Pain Type LE GR Comment
Paracetamol Somatic pain 1a A Evidence based on arthritic pain with good benefit
NSAIDs Pelvic pain with
inflammatory
process (e.g.
dysmenorrhoea)
1a A Good evidence for their use
Central mechanisms
(e.g. endometriosis)
1a A No good evidence for their use
Antidepressants
including tricyclic
antidepressants,
venlafaxine and
duloxetine
Neuropathic pain 1a A Effective. No specific evidence for CPP
Anticonvulsants
gabapentin,
pregabalin
Neuropathic pain,
fibromyalgia
1a A Effective
Gabapentin Women with CPP 2b B Effective
Topical capsaicin Neuropathic pain 1a A Some evidence of benefit
Opioids Chronic non-
malignant pain
1a A Beneficial in a small number of patients
Nerve blocks 3 C Have a role as part of a broad management plan
TENS 1a A No good evidence of benefit
Neuromodulation Pelvic pain 3 C Role developing with increasing research
Figure 18: algorithm for the use of neuropathic analgesics
General history
Medications used
Allergic reactions
Use of alcohol
Assessment
Grade A recommended
Daily activities that
will be effected
Treatment
Grade B recommended
Other comments
Paracetamol in somatic pain
NSAID’s when inflammation is present
Anticonvulsants in neuropathic pain
Topical Capsaicin in neuropathic pain
Antidepressants (including TCA) in neuropathic pain
Nerve blocks as part of a broad management plan [C]
Neuromodulation may become an option, increasing research [C]
Opiods in chronic non-malignant pain
Gabapentin in women with CPP

128 UPDATE FEBRUARY 2012
Figure 19: treatment algorithm for general treatment
10.10 References
1 Stones W, Cheong Ying C, Howard Fred M, et al. Interventions for treating chronic pelvic pain in
women. Cochrane database of systematic reviews [serial on the Internet]. 2005; (2)
http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD000387/frame.html.
2 Remy C, Marret E, Bonnet F. State of the art of paracetamol in acute pain therapy.Curr Opin
Anaesthesiol. 2006 Oct;19(5):562-5.
http://www.ncbi.nlm.nih.gov/pubmed/16960492
3 Roelofs PD, Deyo RA, Koes BW, et al. Non-steroidal anti-inflammatory drugs for low back pain. Spine
(Phila Pa 1976). 2008 Jul 15;33(16):1766-74.
http://www.ncbi.nlm.nih.gov/pubmed/18580547
4 Towheed T, Maxwell L, Judd MG, et al. Acetaminophen for osteoarthritis. Cochrane Cochrane
Database Syst Rev. 2006 Jan 25;(1):CD004257.
http://www.ncbi.nlm.nih.gov/pubmed/16437479
5 Altman RD, Zinsenheim JR, Temple AR, et al. Three-month efficacy and safety of acetaminophen
extended-release for osteoarthritis pain of the hip or knee: a randomized, double-blind, placebo-
controlled study. Osteoarthritis Cartilage. 2007 Apr;15(4):454-61.
http://www.ncbi.nlm.nih.gov/pubmed/17142063
6. Marjoribanks J, Proctor M, Farquhar C, et al. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea.
Cochrane Database Syst Rev. 2010 Jan 20;(1):CD001751.
http://www.ncbi.nlm.nih.gov/pubmed/20091521
7. Allen C, Hopewell S, Prentice A, et al. Nonsteroidal anti-inflammatory drugs for pain in women with
endometriosis. Cochrane Database Syst Rev. 2009 Apr 15;(2):CD004753.
http://www.ncbi.nlm.nih.gov/pubmed/19370608
8. NICE clinical guideline 96. Neuropathic pain. The pharmacological management of neuropathic pain in
adults in non-specialist settings.
http://guidance.nice.org.uk/CG96
General treatment
Pain described in neuropathic or central pain terms
yes no
First line management trial using
1. Amitriptyline
2. Gabapentin
Adequate analgesia:
• review regularly
• sustained effect:
consider dose reduction
Adequate analgesia:
• discharge back to
primary care physician
Inadequate response:
• refer to specialist pain
management unit
Inadequate response:
• consider adding another
first line agent
• rotate agents
Still inadequate:
• refer to specialist pain
management unit
Simple analgesics
ReviewReview
Alternatives:
1. Nortriptyline or Imipramine
2. Pregabalin

UPDATE FEBRUARY 2012 129
9. Saarto T, Wiffen PJ. Antidepressants for neuropathic pain. Cochrane Database Syst Rev. 2007 Oct
17;(4):CD005454.
http://www.ncbi.nlm.nih.gov/pubmed/17943857
10. Lunn MP, Hughes RA, Wiffen PJ. Duloxetine for treating painful neuropathy or chronic pain. Cochrane
Database Syst Rev. 2009 Oct 7;(4):CD007115.
http://www.ncbi.nlm.nih.gov/pubmed/19821395
11. Lee RA, West RM, Wilson JD. The response to sertraline in men with chronic pelvic pain syndrome.
Sex Transm Infect. 2005 Apr;81(2):147-9.
http://www.ncbi.nlm.nih.gov/pubmed/15800093
12. Engel CC Jr, Walker EA, Engel AL, et al. A randomized, double-blind crossover trial of sertraline in
women with chronic pelvic pain. J Psychosom Res. 1998 Feb;44(2):203-7.
http://www.ncbi.nlm.nih.gov/pubmed/9532549
13. Wiffen PJ, Derry S, Moore RA, et al. Carbamazepine for acute and chronic pain in adults. Cochrane
Database Syst Rev. 2011 Jan 19;(1):CD005451.
http://www.ncbi.nlm.nih.gov/pubmed/21249671
14. Moore RA, Wiffen PJ, Derry S, et al. Gabapentin for chronic neuropathic pain and fibromyalgia in
adults. Cochrane Database Syst Rev. 2011 Mar 16;(3):CD007938.
http://www.ncbi.nlm.nih.gov/pubmed/21412914
15. Sator-Katzenschlager SM, Scharbert G, Kress HG, et al. Chronic pelvic pain treated with gabapentin
and amitriptyline: a randomized controlled pilot study. Wien Klin Wochenschr. 2005 Nov;117(21-22):
761-8.
http://www.ncbi.nlm.nih.gov/pubmed/16416358
16. Moore RA, Straube S, Wiffen PJ et al. Pregabalin for acute and chronic pain in adults. Cochrane
Database Syst Rev. 2009 Jul 8;(3):CD007076.
http://www.ncbi.nlm.nih.gov/pubmed/19588419
17. Derry S, Lloyd R, Moore RA, et al. Topical capsaicin for chronic neuropathic pain in adults. Cochrane
Database Syst Rev. 2009 Oct 7;(4):CD007393.
http://www.ncbi.nlm.nih.gov/pubmed/19821411
18. Seidel S, Aigner M, Ossege M, et al. Antipsychotics for acute and chronic pain in adults. Cochrane
Database Syst Rev. 2008 Oct 8;(4):CD004844.
http://www.ncbi.nlm.nih.gov/pubmed/18843669
19. Noble M, Treadwell JR, Tregear SJ, et al. Long-term opioid management for chronic noncancer pain.
Cochrane Database Syst Rev. 2010 Jan 20;(1):CD006605.
http://www.ncbi.nlm.nih.gov/pubmed/20091598
20. The British Pain Society. Opioids for persistent pain: Good practice. 2010.
http://www.britishpainsociety.org/book_opioid_main.pdf
21. The British Pain Society. Opioids for persistent pain: Information for patients. 2010.
http://www.britishpainsociety.org/pub_patient.htm
22. The British Pain Society. Pain and problem drug use: Information for patients. 2007.
http://www.britishpainsociety.org/pub_patient.htm
23. Quigley C. Opioid switching to improve pain relief and drug tolerability. Cochrane Database Syst Rev.
2004;(3):CD004847.
http://www.ncbi.nlm.nih.gov/pubmed/15266542
24. Lee M, Silverman SM, Hansen H, et al. A comprehensive review of opioid-induced hyperalgesia. Pain
Physician. 2011 Mar-Apr;14(2):145-61.
http://www.ncbi.nlm.nih.gov/pubmed/21412369
25. Sotgiu ML, Valente M, Storchi R, et al. Cooperative N-methyl-D-aspartate (NMDA) receptor
antagonism and mu-opioid receptor agonism mediate the methadone inhibition of the spinal neuron
pain-related hyperactivity in a rat model of neuropathic pain. Pharmacol Res 2009 Oct;60(4):284-90.
http://www.ncbi.nlm.nih.gov/pubmed/19717013
26. Olesen AE, Staahl C, Arendt-Nielsen L, et al. Different effects of morphine and oxycodone in
experimentally evoked hyperalgesia: a human translational study. Br J Clin Pharmacol. 2010
Aug;70(2):189-200.
http://www.ncbi.nlm.nih.gov/pubmed/20653672
27. Baranowski AP, Fall M, Abrams P. Urogenital Pain in Clinical Practice: Taylor and Francis; 2007.
28. Nnoaham KE, Kumbang J. Transcutaneous electrical nerve stimulation (TENS) for chronic pain.
Cochrane Database Syst Rev. 2008 Jul 16;(3):CD003222.
http://www.ncbi.nlm.nih.gov/pubmed/18646088

130 UPDATE FEBRUARY 2012
29. NICE technology appraisal guidance 159. Spinal cord stimulation for chronic pain of neuropathic or
ischaemic origin.
http://guidance.nice.org.uk/TA159
30. Fariello JY, Whitmore K. Sacral neuromodulation stimulation for IC/PBS, chronic pelvic pain, and
sexual dysfunction. Int Urogynecol J Pelvic Floor Dysfunct 2010 Dec;21(12):1553-8.
http://www.ncbi.nlm.nih.gov/pubmed/20972541

UPDATE FEBRUARY 2012 131
11. ABBREVIATIONS USED IN THE TEXT
This list is not comprehensive for the most common abbreviations
AMPA amino-methylene-phosphonic acid
ATP Adenosinetriphosphate
BCG Bacillus Calmette Guérin
BDNF brain-derived neurotrophic factor
BPS bladder pain syndrome
BTX-A Botulinum toxin A
CBT cognitive behavioural therapy
CFS chronic fatigue syndrome
CHRP calcitonin gene-related peptide
CI confidence interval
CNS central nervous system
CPP chronic pelvic pain
CPPS chronic pelvic pain syndrome
CRH corticotrophin-releasing hormone
CyA Cyclosporin A
DMSO Dimethyl sulphoxide
DNIC diffuse noxious inhibitory control
DRG dorsal root ganglion
EH excisional haemorrhoidectomy
ESSIC European Society for the Study of BPS
FM fibromyalgia
FSS functional somatic syndrome
GAG glycosaminoglycan
HBO Hyperbaric oxygen
HIF hypoxia inducible factor
IASP Association for the Study of Pain
IBS irritable bowel syndrome
ICDB Interstitial Cystitis Data Base
ICSI Interstitial Cystitis Symptom Index
IPPS International Prostate Symptom Score
ISSVD Society for the Study of Vulvovaginal Disease
LUTS lower urinary tract symptoms
MAPP Multi-disciplinary Approach to the study of chronic Pelvic Pain research
MPA medroxyprogesterone acetate
MRI magnetic resonance imaging
NBS non-bladder syndromes
NGF nerve growth factor
NIDDK National Institute of Diabetes and Digestive and Kidney Diseases
NIH National Institutes of Health
NIH-CPSI NIH Prostatitis Symptom Index
NMDA N-methyl-D-aspartate
NNT numbers needed to treat
NO nitric oxide
PAG periaqueductal grey
PID pelvic inflammatory disease
PNS pudendal nerve stimulation
PNS peripheral nervous system
PPMT pre-post-massage test
PPS prostate pain syndrome
QoL quality of life
RBL rubber band ligation
RCT randomised controlled trial
RTX Resiniferatoxin
RUR transurethral resection
TUNA transurethral needle ablation
VAPS visual analogue pain scale

132 UPDATE FEBRUARY 2012
Conflict of interest
All members of the Chronic Pelvic Pain Guidelines panel have provided disclosure statements on all
relationships that they have and that might be perceived to be a potential source of conflict of interest. This
information is kept on file in the European Association of Urology Central Office database. This guidelines
document was developed with the financial support of the European Association of Urology. No external
sources of funding and support have been involved. The EAU is a non-profit organisation and funding is limited
to administrative assistance and travel and meeting expenses. No honoraria or other reimbursements have
been provided.
