British Association of Dermatologists
Dermatology

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
1
This publication is supported by the British Association of Dermatologists.
First edition 2009
Revised first edition 2009
Second edition 2014
Third edition 2020
For comments and feedback, please contact the author at drnicoledermatol[email protected]m

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
2
Dermatology
Dr Nicole Yi Zhen Chiang MBChB (Hons), MRCP (UK), MRCP(UK)(Derm)
Consultant Dermatologist
Manchester University Hospitals NHS Trust
Withington Hospital M20 2LR
Manchester
Professor Julian Verbov JP MD FRCP FRCPCH CBiol FRSB FLS MCSFS
Professor of Dermatology
Consultant Paediatric Dermatologist
Alder Hey Children’s Hospital
East Prescot Road
Liverpool L14 5AB

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
3
Contents
Preface 5
What is dermatology? 6
Essential Clinical Skills 7
Taking a dermatological history 7
Examining the skin 8
Communicating examination findings 9
Background Knowledge 23
Functions of normal skin 23
Structure of normal skin and the skin appendages 23
Principles of wound healing 27
Emergency Dermatology 28
Urticaria, Angioedema and Anaphylaxis 29
Erythema nodosum 30
Erythema multiforme, Stevens-Johnson syndrome, Toxic epidermal necrolysis 31
Acute meningococcaemia 32
Erythroderma 33
Eczema herpeticum 34
Necrotizing fasciitis 35
Skin Infections / Infestations 36
Erysipelas and cellulitis 37
Staphylococcal scalded skin syndrome 38
Superficial fungal skin infections 39
Skin Cancer 41
Basal cell carcinoma 42
Squamous cell carcinoma 43
Malignant melanoma 44
Inflammatory Skin Conditions 46
Atopic eczema 47
Acne vulgaris 49
Psoriasis 50
Foreword 5
Blistering Disorders 52
Bullous pemphigoid 53
Pemphigus vulgaris 54

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
4
Common Important Problems 57
Chronic leg ulcers 58
Itchy eruption 60
A changing pigmented lesion 62
Purpuric eruption 64
A red swollen leg 66
Keloid Scars 67
Practical Skills 72
Patient education 73
Written communication 74
Prescribing skills 74
Clinical examination and investigations 75
71
General Reference & Acknowledgements 76
Management 68
Emollients 69
Topical/Oral steroids 69
Oral aciclovir 69
Oral antihistamines 70
Topical/Oral antibiotics 70
Topical antiseptics 70
Oral retinoids 70
Biological therapy 71
Pigmentary Disorders 55
Vitiligo 55
Melasma 56

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
5
11 years have passed since this Handbook first appeared. It has proved immensely popular
and it has been further updated. We hope that it will continue to be a valuable source book
for those interested in learning about this exciting specialty. The Handbook was designed to
be an overview, both succinct and reader-friendly which continues to be our aim.
Once again, many thanks to the BAD for its essential and continuing support.
Julian Verbov
Professor of Dermatology Liverpool 2020
Past BAD President Dr Mark Goodfield wrote in the first edition:
‘There is a real need for appropriate information about dermatological diseases to meet the
educational needs of doctors at all levels.’
This holds true even more today than in 2009 with the exponential use of social media as an
information sourced by patients and clinicians alike. Since its first publication, this book has
been the go to resource for accurate knowledge in common and urgent dermatological
problems. Its essential role in supporting their workplace learning is highlighted by the 8,843
downloads and 50,000 requests for hard copies from individual students and medical
schools throughout the UK. Starting with scientific and epidemiological facts, moving
through clinical features and management, medical students are given a structure that
enables them to organise learning effectively. The content remains focused on learning at
the undergraduate stage of the medical education spectrum: a vital foundation for
postgraduate training in dermatology.
The UK population has become increasingly diverse over the last few decades, it is therefore
necessary to update the handbook to highlight tips for assessment, variation in presentation
in common and important skin conditions (e.g. common pigmentary disorders) that reflect
the spectrum of cutaneous diversity junior clinicians will encounter in their practice. This, in
combination, with other BAD resources under current development will ensure that medical
students continue to learn from the highest quality education in dermatology to the benefit
of our patients.
Dr Tanya Bleiker
President of the British Association of Dermatologists
Prof Mini Singh
Undergraduate Work Stream Chair, British Association of Dermatologists
Foreword to Third edition
Preface to the 3rd edition

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
6
• Dermatology is the study of both normal and abnormal skin and associated
structures such as hair, nails, and oral and genital mucous membranes.
• Skin diseases are very common, affecting up to a third of the population at any one
time.
• Skin diseases have serious impacts on life. They can cause physical damage,
embarrassment, and social and occupational restrictions. Chronic skin diseases may
cause financial constraints with repeated sick leave. Some skin conditions can be
life-threatening.
• In 2006-07, the total NHS health expenditure for skin diseases was estimated to be
around ₤97 million (approximately 2% of the total NHS health expenditure).
• The British Association of Dermatologists outlined the essential and important
learning outcomes that should be achieved by all medical undergraduates for the
competent assessment of patients presenting with skin disorders
(available on:
https://www.bad.org.uk/shared/get-file.ashx?itemtype=document&id=4168)
• This handbook addresses these learning outcomes and aims to equip you with the
knowledge and skills to practise competently and safely as a junior doctor.
What is dermatology?
Why is dermatology important?
What is this handbook about?
Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
7
• Detailed history taking and examination provide important diagnostic clues in the
assessment of skin problems.
Taking a dermatological history
• Using the standard structure of history taking, below are the important points to
consider when taking a history from a patient with a skin problem (Table 1).
• For dark lesions or moles, pay attention to questions marked with an asterisk (*).
Table 1. Taking a dermatological history
Main headings Key questions
Presenting complaint Nature, site and duration of problem
History of presenting complaint Initial appearance and evolution of lesion*
Symptoms (particularly itch and pain)*
Aggravating and relieving factors
Previous and current treatments (effective or not)
Recent contact, stressful events, illness and travel
History of sunburn and use of tanning machines*
Skin type (see page 70)*
Past medical history History of atopy i.e. asthma, allergic rhinitis, eczema
History of skin cancer and suspicious skin lesions
Family history Family history of skin disease*
Social history Occupation (including skin contacts at work)
Improvement of lesions when away from work
Essential Clinical Skills
Learning outcomes:
1. Ability to take a dermatological history
2. Ability to explore a patient’s concerns and expectations
3. Ability to interact sensitively with people with skin disease
4. Ability to examine skin, hair, nails and mucous membranes systematically
showing respect for the patient
5. Ability to describe physical signs in skin, hair, nails and mucosa
6. Ability to record findings accurately in patient’s records
7.
Essential Clinical Skills
– Taking a dermatological history

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
8
Medication and allergies Regular, recent and over-the-counter medications
Impact on quality of life Impact of skin condition and concerns
Examining the skin
• There are four important principles in performing a good examination of the skin:
INSPECT, DESCRIBE, PALPATE and SYSTEMATIC CHECK (Table 2).
Table 2. Examining the skin
Main principles Key features
INSPECT in general General observation
Note if richly pigmented skin therefore signs of skin
changes may be different ( e.g. erythema not as
obvious
Site and number of lesion(s)
If multiple, pattern of distribution and configuration
DESCRIBE the individual lesion SCAM
Size (the widest diameter), Shape
Colour
Associated secondary change
Morphology, Margin (border)
*If the lesion is pigmented, remember ABCDE
(the presence of any of these features increase the likelihood of melanoma):
Asymmetry (lack of mirror image in any of the
four quadrants)
Irregular Border
Two or more Colours within the lesion
Diameter > 6mm
Evolution ( history of change in size, shape or
colour)
PALPATE* the individual lesion Surface
Essential Clinical Skills
– Examining the skin

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
9
Consistency
Mobility
Tenderness
Temperature
* Essential in richly pigmented skin to accurately
classify lesions
SYSTEMATIC CHECK Examine the nails, scalp, hair & mucous membranes
General examination of all systems relevant to
presenting symptoms
Communicating examination findings
• In order to describe, record and communicate examination findings accurately, it is
important to learn the appropriate terminology (Tables 3-10).
Table 3. General terms
Terms Meaning
Pruritus Itching
Lesion An area of altered skin
Rash An eruption
Naevus A localised malformation of tissue structures
Example: (Picture Source: D@nderm)
Comedone A plug in a sebaceous follicle containing altered sebum, bacteria and
cellular debris; can present as either open (blackheads) or closed
(whiteheads)
Example:
Pigmented melanocytic naevus (mole)
Essential Clinical
Skills – Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
10
Table 4. Distribution (the pattern of spread of lesions)
Terms Meaning
Generalised All over the body
Widespread Extensive
Localised Restricted to one area of skin only
Flexural Body folds i.e. groin, neck, behind ears, popliteal and antecubital fossa
Extensor Knees, elbows, shins
Pressure areas Sacrum, buttocks, ankles, heels
Dermatome An area of skin supplied by a single spinal nerve
Photosensitive Affects sun-exposed areas such as face, neck and back of hands
Example:
Köebner A linear eruption arising at site of trauma
phenomenon Example:
Sunburn
Open comedones (left) and closed comedones (right) in acne
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
11
Table 5. Configuration (the pattern or shape of grouped lesions)
Terms Meaning
Discrete Individual lesions separated from each other
Confluent Lesions merging together
Linear In a line
Target Concentric rings (like a dartboard)
Example:
Annular Like a circle or ring
Example:
Psoriasis
Erythema multiforme
Tinea corporis
(‘ringworm’)
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
12
Discoid / A coin-shaped/round lesion
Nummular Example: Discoid eczema
Table 6. Colour
Terms Meaning
Erythema Redness (due to inflammation and vasodilatation) which blanches on
pressure
Example:
Purpura Red or purple colour (due to bleeding into the skin or mucous membrane)
which does not blanch on pressure – petechiae (small pinpoint macules) and
ecchymoses (larger bruise-like patches)
Example:
Hypopigmentation of discoid
lupus
Palmar erythema
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
13
Hypo- Area(s) of paler skin
pigmentation Examples:
R © Cardiff and Vale University Health Board
De-pigmentation: White skin due to absence of melanin
Examples:
M and R © Cardiff and Vale University Health Board
Note the three colours ‘tricolor’ pattern typical of vitiligo.
Hyper-pigmentation Darker skin which may be due to various causes (e.g. post-
inflammatory, melasma, naevi)
Henoch-Schönlein purpura
(palpable small vessel vasculitis)
Pityriasis versicolor
(a superficial fungus infection)
Vitiligo
(loss of skin
melanocytes)
Melasma (increased melanin pigmentation)
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
14
Examples:
Table 7. Morphology (the structure of a lesion) – Primary lesions
Terms Meaning
Macule A flat area of altered colour
Example:
Patch Larger flat area of altered colour or texture
Example:
Freckles
Vascular malformation
(naevus flammeus / ‘port wine stain’)
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
15
Papule Solid raised lesion < 0.5cm in diameter
Example:
Nodule Solid raised lesion >0.5cm in diameter with a deeper component
Example: (Picture source: D@nderm)
Plaque Palpable scaling raised lesion >0.5cm in diameter
Example:
Vesicle Raised, clear fluid-filled lesion <0.5cm in diameter
(small blister) Example:
Psoriasis
Pyogenic granuloma
(granuloma telangiectaticum)
Xanthomata
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
16
Bulla Raised, clear fluid-filled lesion >0.5cm in diameter
(large blister) Example:
Pustule Pus-containing lesion <0.5cm in diameter
Example:
Abscess Localised accumulation of pus in the dermis or subcutaneous tissues
Example:
W(h)eal Transient raised lesion due to dermal oedema
Acne
Reaction to insect bites
Acute hand eczema
(pompholyx)
Periungual abscess
(acute paronychia)
Essential Clinical Skills
– Communicating examination
findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
17
Examples: Urticaria
Boil/Furuncle Staphylococcal infection around or within a hair follicle
Carbuncle Staphylococcal infection of adjacent hair follicles (multiple boils/furuncles)
Table 8. Morphology - Secondary lesions (lesions that evolve from primary lesions)
Terms Meaning
Excoriation Loss of epidermis following trauma
Example:
Note how subtle the erythema is in this wheal in patient with skin type V.
Excoriations in eczema
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
18
Lichenification Well-defined roughening of skin with accentuation of skin markings
Examples:
Lichenification due to chronic
rubbing in eczema
© Cardiff and Vale University Health Board
Lichenification in
darker skin types:
the clue is the
increased
appearance of skin
lines at the bottom
of this photograph.
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
19
Scales Flakes of stratum corneum
Example:
Crust Rough surface consisting of dried serum, blood, bacteria and cellular debris
that has exuded through an eroded epidermis (e.g. from a burst blister)
Example:
Scar New fibrous tissue which occurs post-wound healing, and may be atrophic
(thinning), hypertrophic (hyperproliferation within wound boundary), or
keloidal (hyperproliferation beyond wound boundary)
Examples: Keloid scars
R © Cardiff and Vale University Health Board
Impetigo
Psoriasis (showing silvery scales)
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
20
Ulcer Loss of epidermis and dermis (heals with scarring)
Example:
Fissure An epidermal crack often due to excess dryness
Example:
Striae Linear areas which progress from purple to pink to white, with the
histopathological appearance of a scar (associated with excessive steroid
usage and glucocorticoid production, growth spurts and pregnancy)
Example:
Leg ulcers
Striae
Eczema
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
21
Table 9. Hair
Terms Meaning
Alopecia Loss of hair
Examples:
Alopecia areata (well-defined patch of complete hair loss) Scarring alopecia of the scalp © Cardiff
and Vale University Health Board
Hirsutism Androgen-dependent hair growth in a female
Example:
Hypertrichosis Non-androgen dependent pattern of excessive hair growth
(e.g. in pigmented naevi)
Example:
Hirsutism
Hypertrichosis
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
22
Table 10. Nails
Terms Meaning
Clubbing Loss of angle between the posterior nail fold and nail plate
(associations include suppurative lung disease, cyanotic heart disease,
inflammatory bowel disease and idiopathic)
Example: (Picture source: D@nderm)
Koilonychia Spoon-shaped depression of the nail plate
(associations include iron-deficiency anaemia, congenital and idiopathic)
Example: (Picture source: D@nderm)
Onycholysis Separation of the distal end of the nail plate from nail bed
(associations include trauma, psoriasis, fungal nail infection and
hyperthyroidism)
Example: (Picture source: D@nderm)
Pitting Punctate depressions of the nail plate
(associations include psoriasis, eczema and alopecia areata)
Example: (Picture source: D@nderm)
Clubbing
Koilonychia
Onycholysis
Pitting
Essential Clinical Skills
– Communicating examination findings

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
23
• This section covers the basic knowledge of normal skin structure and function
required to help understand how skin diseases occur.
Functions of normal skin
• These include:
i) Protective barrier against environmental insults
ii) Temperature regulation
iii) Sensation
iv) Vitamin D synthesis
v) Immunosurveillance
vi) Appearance/cosmesis
Structure of normal skin and the skin appendages
• The skin is the largest organ in the human body. It is composed of the epidermis and
dermis overlying subcutaneous tissue. The skin appendages (structures formed by
skin-derived cells) are hair, nails, sebaceous glands and sweat glands.
Epidermis
• The epidermis is composed of 4 major cell types, each with specific functions (Table
11).
Background Knowledge
Learning outcomes:
1. Ability to describe the functions of normal skin
2. Ability to describe the structure of normal skin
3. Ability to describe the principles of wound healing
4. Ability to describe the difficulties, physical and psychological, that may be
experienced by people with chronic skin disease
Background Knowledge
– Functions of normal skin

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
24
Table 11. Main functions of each cell type in the epidermis
Cell types Main functions
Keratinocytes Produce keratin as a protective barrier
Langerhans’ cells Present antigens and activate T-lymphocytes for immune protection
Melanocytes Produce melanin, which gives pigment to the skin and protects the
cell nuclei from ultraviolet (UV) radiation-induced DNA damage
Merkel cells Contain specialised nerve endings for sensation
• There are 4 layers in the epidermis (Table 12), each representing a different stage of
maturation of the keratinocytes. The average epidermal turnover time (migration of
cells from the basal cell layer to the horny layer) is about 30 days.
Table 12. Composition of each epidermal layer
Epidermal layers Composition
Stratum basale Actively dividing cells, deepest layer
(Basal cell layer)
Stratum spinosum Differentiating cells
(Prickle cell layer)
Stratum granulosum So-called because cells lose their nuclei and contain
(Granular cell layer) granules of keratohyaline. They secrete lipid into the
intercellular spaces.
Stratum corneum Layer of keratin, most superficial layer
(Horny layer)
• In areas of thick skin such as the sole, there is a fifth layer, stratum lucidum, beneath
the stratum corneum. This consists of paler, compact keratin.
• Pathology of the epidermis may involve:
a) changes in epidermal turnover time - e.g. psoriasis (reduced epidermal
turnover time)
b) changes in the surface of the skin or loss of epidermis - e.g. scales,
crusting, exudate, ulcer
c) changes in pigmentation of the skin - e.g. hypo- or hyper-pigmented skin
Background Knowledge
– Structure of normal skin and the skin appendages

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
25
Dermis
• The dermis is made up of collagen (mainly), elastin and glycosaminoglycans, which
are synthesised by fibroblasts. Collectively, they provide the dermis with strength
and elasticity.
• The dermis also contains immune cells, nerves, skin appendages as well as lymphatic
and blood vessels.
• Pathology of the dermis may involve:
a) changes in the contour of the skin or loss of dermis e.g. formation of
papules, nodules, skin atrophy and ulcers
b) disorders of skin appendages e.g. disorders of hair, acne (disorder of
sebaceous glands)
c) changes related to lymphatic and blood vessels e.g. erythema
(vasodilatation), urticaria (increased permeability of capillaries and small
venules), purpura (capillary leakage)
Hair
• There are 3 main types of hair:
a) lanugo hair (fine long hair in fetus)
b) vellus hair (fine short hair on all body surfaces)
c) terminal hair (coarse long hair on the scalp, eyebrows, eyelashes and
pubic areas)
• Each hair consists of modified keratin and is divided into the hair shaft (a keratinized
tube) and hair bulb (actively dividing cells, and melanocytes which give pigment to
the hair).
• Each hair follicle enters its own growth cycle. This occurs in 3 main phases:
a) anagen (long growing phase)
b) catagen (short regressing phase)
c) telogen (resting/shedding phase)
• Pathology of the hair may involve:
a) reduced or absent melanin pigment production e.g. grey or white hair
b) changes in duration of the growth cycle e.g. hair loss (premature entry of
hair follicles into the telogen phase)
c) shaft abnormalities
Background Knowledge
– Structure of normal skin and
the skin appendages

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
26
Nails
• The nail is made up of a nail plate (hard keratin) which arises from the nail matrix at
the posterior nail fold, and rests on the nail bed.
• The nail bed contains blood capillaries which gives the pink colour of the nails.
• Pathology of the nail may involve:
a) abnormalities of the nail matrix e.g. pits and ridges
b) abnormalities of the nail bed e.g. splinter haemorrhage
c) abnormalities of the nail plate e.g. discoloured nails, thickening of nails
Sebaceous glands
• Sebaceous glands produce sebum via hair follicles (collectively called a
pilosebaceous unit). They secrete sebum onto the skin surface which lubricates and
waterproofs the skin.
• Sebaceous glands are stimulated by the conversion of androgens to
dihydrotestosterone and therefore become active at puberty.
• Pathology of sebaceous glands may involve:
a) increased sebum production and bacterial colonisation e.g. acne
b) sebaceous gland hyperplasia
Sweat glands
• Sweat glands regulate body temperature and are innervated by the sympathetic
nervous system.
• They are divided into two types: eccrine and apocrine sweat glands.
• Eccrine sweat glands are universally distributed in the skin.
• Apocrine sweat glands are found in the axillae, areolae, genitalia and anus, and
modified glands are found in the external auditory canal. They only function from
puberty onwards and action of bacteria on the sweat produces body odour.
• Pathology of sweat glands may involve:
a) inflammation/infection of apocrine glands e.g. hidradenitis suppurativa
b) overactivity of eccrine glands e.g. hyperhidrosis
Background Knowledge
– Structure of normal skin and
the skin appendages

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
27
Principles of wound healing
• Wound healing occurs in 4 phases: haemostasis, inflammation, proliferation and
remodelling (Table 13).
Table 13. Stages of wound healing
Stages of wound healing Mechanisms
Haemostasis ● Vasoconstriction and platelet aggregation
● Clot formation
Inflammation ● Vasodilatation
● Migration of neutrophils and macrophages
● Phagocytosis of cellular debris and invading
bacteria
Proliferation ● Granulation tissue formation (synthesised by
fibroblasts) and angiogenesis
● Re-epithelialisation (epidermal cell proliferation
and migration)
Remodelling ● Collagen fibre re-organisation
● Scar maturation
Background Knowledge
– Principles of wound healing

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
28
• These are rapidly progressive skin conditions and some are potentially life-
threatening. Early recognition is important to implement prompt supportive care
and therapy.
• Some are drug reactions and the offending drug should be withdrawn.
• The essential management for all dermatological emergencies, like any emergency,
consists of:
i) full supportive care - ABC of resuscitation
ii) withdrawal of precipitating agents
iii) management of associated complications
iv) specific treatment (highlighted below under each condition)
Emergency Dermatology
Learning outcomes:
1. Ability to recognise and describe these skin reactions:
- urticaria
- erythema nodosum
- erythema multiforme
2. Ability to recognise these emergency presentations, discuss the causes,
potential complications and provide first contact care in these emergencies:
- anaphylaxis and angioedema
- toxic epidermal necrolysis
- Stevens-Johnson syndrome
- acute meningococcaemia
- erythroderma
- eczema herpeticum
- necrotising fasciitis
Emergency Dermatology

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
29
Urticaria, Angioedema and Anaphylaxis
Causes ● Idiopathic, food (e.g. nuts, sesame seeds, shellfish, dairy
products), drugs (e.g. penicillin, contrast media, non-steroidal anti-
inflammatory drugs (NSAIDs), morphine, angiotensin-converting
enzyme inhibitors (ACE-i)), insect bites, contact (e.g. latex), viral or
parasitic infections, autoimmune, and hereditary (in some cases of
angioedema)
Description ● Urticaria is due to a local increase in permeability of capillaries
and small venules. A large number of inflammatory mediators
(including prostaglandins, leukotrienes, and chemotactic factors)
play a role but histamine derived from skin mast cells appears to
be the major mediator. Local mediator release from mast cells can
be induced by immunological or non-immunological mechanisms.
Presentation ● Urticaria (swelling involving the superficial dermis, raising the
epidermis): itchy wheals
● Angioedema (deeper swelling involving the dermis and
subcutaneous tissues): swelling of tongue and lips
● Anaphylaxis (also known as anaphylactic shock): bronchospasm,
facial and laryngeal oedema, hypotension; can present initially
with urticaria and angioedema
Management ● Antihistamines for urticaria
● Corticosteroids for severe acute urticaria and angioedema
● Adrenaline, corticosteroids and antihistamines for anaphylaxis
Complications ● Urticaria is normally uncomplicated
● Angioedema and anaphylaxis can lead to asphyxia, cardiac arrest
and death
Urticaria Angioedema
Emergency Dermatology
– Urticaria, Angioedema and
Anaphylaxis

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
30
Erythema nodosum
Description ● A hypersensitivity response to a variety of stimuli
Causes ● Group A beta-haemolytic streptococcus, primary tuberculosis,
pregnancy, malignancy, sarcoidosis, inflammatory bowel disease
(IBD), chlamydia and leprosy
Presentation ● Discrete tender nodules which may become confluent
● Lesions continue to appear for 1-2 weeks and leave bruise-like
discolouration as they resolve
● Lesions do not ulcerate and resolve without atrophy or scarring
● The shins are the most common site
Erythema nodosum
Emergency Dermatology
– Erythema nodosum

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
31
Erythema multiforme, Stevens-Johnson syndrome and Toxic epidermal necrolysis
Description ● Erythema multiforme, often of unknown cause, is an acute self-
limiting inflammatory condition with herpes simplex virus being
the main precipitating factor. Other infections and drugs are also
causes. Mucosal involvement is absent or limited to only one
mucosal surface.
● Stevens-Johnson syndrome is characterised by
mucocutaneous necrosis with at least two mucosal sites involved.
Skin involvement may be limited or extensive. Drugs or
combinations of infections or drugs are the main associations.
Epithelial necrosis with few inflammatory cells is seen on
histopathology. The extensive necrosis distinguishes Stevens-
Johnson syndrome from erythema multiforme. Stevens-Johnson
syndrome may have features overlapping with toxic epidermal
necrolysis including a prodromal illness.
● Toxic epidermal necrosis which is usually drug-induced, is
an acute severe similar disease characterised by extensive skin and
mucosal necrosis accompanied by systemic toxicity. On
histopathology there is full thickness epidermal necrosis with
subepidermal detachment.
Management ● Early recognition and call for help
● Full supportive care to maintain haemodynamic equilibrium
Complications ● Mortality rates are 5-12% with SJS and >30% with TEN with
death often due to sepsis, electrolyte imbalance or multi-system
organ failure
Erythema multiforme Stevens-Johnson syndrome
Emergency Dermatology
– Erythema multiforme, Stevens
-Johnson syndrome and Toxic epidermal necrolysis

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
32
Acute meningococcaemia
Description ● A serious communicable infection transmitted via respiratory
secretions; bacteria get into the circulating blood
Cause ● Gram negative diplococcus Neisseria meningitides
Presentation ● Features of meningitis (e.g. headache, fever, neck stiffness),
septicaemia (e.g. hypotension, fever, myalgia) and a typical rash
● Non-blanching purpuric rash on the trunk and extremities, which
may be preceded by a blanching maculopapular rash, and can
rapidly progress to ecchymoses, haemorrhagic bullae and tissue
necrosis
Management ● Antibiotics (e.g. benzylpenicillin)
● Prophylactic antibiotics (e.g. rifampicin) for close contacts (ideally
within 14 days of exposure)
Complications ● Septicaemic shock, disseminated intravascular coagulation, multi-
organ failure and death
Emergency Dermatology
– Acute meningococcaemia

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
33
Erythroderma (‘red skin’)
Description ● Exfoliative dermatitis involving at least 90% of the skin surface
Causes ● Previous skin disease (e.g. eczema, psoriasis), lymphoma, drugs
(e.g.sulphonamides, gold, sulphonylureas, penicillin, allopurinol,
captopril) and idiopathic
Presentation ● Skin appears inflamed, oedematous and scaly
● Systemically unwell with lymphadenopathy and malaise
Management ● Treat the underlying cause, where known
● Emollients and wet-wraps to maintain skin moisture
● Topical steroids may help to relieve inflammation
Complications ● Secondary infection, fluid loss and electrolyte imbalance,
hypothermia, high-output cardiac failure and capillary leak
syndrome (most severe)
Prognosis ● Largely depends on the underlying cause
● Overall mortality rate ranges from 20 to 40%
Erythroderma
In richly pigmented skin the erythema doesn’t look as bright, but on close inspection the inflamed
skin might appear a darker shade of brown or black, with a hint of erythema visible. Palpating the skin
for increased temperature is a vital clue.
Emergency Dermatology
– Erythroderma

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
34
Eczema herpeticum (Kaposi’s varicelliform eruption)
Description ● Widespread eruption - serious complication of atopic eczema or
less commonly other skin conditions
Cause ● Herpes simplex virus
Presentation ● Extensive crusted papules, blisters and erosions
● Systemically unwell with fever and malaise
Management ● Antivirals (e.g. aciclovir)
● Antibiotics for bacterial secondary infection
Complications ● Herpes hepatitis, encephalitis, disseminated intravascular
coagulation (DIC) and rarely, death
Eczema herpeticum
Emergency Dermatology
– Eczema herpeticum

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
35
Necrotising fasciitis
Description ● A rapidly spreading infection of the deep fascia with secondary
tissue necrosis
Causes ● Group A haemolytic streptococcus, or a mixture of anaerobic and
aerobic bacteria
● Risk factors include abdominal surgery and medical co-morbidities
(e.g. diabetes, malignancy)
● 50% of cases occur in previously healthy individuals
Presentation ● Severe pain
● Erythematous, blistering, and necrotic skin
● Systemically unwell with fever and tachycardia
● Presence of crepitus (subcutaneous emphysema)
● X-ray may show soft tissue gas (absence should not exclude the
diagnosis)
Management ● Urgent referral for extensive surgical debridement
● Intravenous antibiotics
Prognosis ● Mortality up to 76%
Emergency Dermatology
– Necrotising fasciitis

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
36
• The normal skin microflora and antimicrobial peptides protect the skin against
infection. However, when there is skin damage, microorganisms can penetrate
resulting in infection.
• There are 3 main types of skin infections according to their sources: bacterial (e.g.
staphylococcal and streptococcal), viral (e.g. human papilloma virus, herpes simplex
(see page 34) and herpes zoster (see below)), and fungal (e.g. tinea (see page 39 &
40), candida (see page 39 & 40) and yeasts). Infestations (e.g. scabies (see page 60 &
61), lice, cutaneous leishmaniasis) can also occur.
Skin Infections / Infestations
Herpes zoster (shingles) infection due to varicella-zoster virus affecting the
distribution of the ophthalmic division of the fifth cranial (trigeminal) nerve
Note: Examination for eye involvement is important
Learning outcomes:
Ability to describe the presentation, investigation and management of:
- cellulitis and erysipelas
- staphylococcal scalded skin syndrome
- superficial fungal infections
Skin Infections / Infestations

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
37
Erysipelas and Cellulitis
Description ● Spreading bacterial infection of the skin
● Cellulitis involves the deep subcutaneous tissue
● Erysipelas is an acute superficial form of cellulitis and involves
the dermis and upper subcutaneous tissue
Causes ● Streptococcus pyogenes and Staphylococcus aureus
● Risk factors include immunosuppression, wounds, leg ulcers,
toeweb intertrigo, and minor skin injury
Presentation ● Most common in the lower limbs
● Local signs of inflammation – swelling (tumor), erythema (rubor),
warmth (calor), pain (dolor); may be associated with lymphangitis
● Systemically unwell with fever, malaise or rigors, particularly with
erysipelas
● Erysipelas is distinguished from cellulitis by a well-defined, red
raised border
Management ● Antibiotics (e.g. flucloxacillin or benzylpenicillin)
● Supportive care including rest, leg elevation, sterile dressings and
analgesia
Complications ● Local necrosis, abscess and septicaemia
Cellulitis with elephantiasis of the penis
Erysipelas
Erysipelas
Even though this is in richly
pigmented skin the
unilateral oedema and
erythema is clearly present
suggesting cellulitis.
Skin Infections and Infestations
– Erysipelas and Cellulitis

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
38
Staphylococcal scalded skin syndrome
Description ● Commonly seen in infancy and early childhood
Cause ● Production of a circulating epidermolytic toxin from phage group
II, benzylpenicillin-resistant (coagulase positive) staphylococci
Presentation ● Develops within a few hours to a few days, and may be worse over
the face, neck, axillae or groins
● A scald-like skin appearance is followed by large flaccid bulla
● Perioral crusting is typical
● There is intraepidermal blistering in this condition
● Lesions are very painful
● Sometimes the eruption is more localised
● Recovery is usually within 5-7 days
Management ● Antibiotics (e.g. a systemic penicillinase-resistant penicillin,
erythromycin or appropriate cephalosporin)
● Analgesia
Staphylococcal scalded skin syndrome
Skin Infections and Infestations
– Staphylococcal scalded skin syndrome

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
39
Superficial fungal infections
Description ● A common and mild infection of the superficial layers of the skin,
nails and hair, but can be severe in immunocompromised
individuals
Cause ● Three main groups: dermatophytes (tinea/ringworm), yeasts (e.g.
candidiasis, malassezia), moulds (e.g. aspergillus)
Presentation ● Varies with the site of infection; usually unilateral and itchy
● Tinea corporis (tinea infection of the trunk and limbs) - Itchy,
circular or annular lesions with a clearly defined, raised and scaly
edge is typical
● Tinea cruris (tinea infection of the groin and natal cleft) – very
itchy, similar to tinea corporis
● Tinea pedis (athlete’s foot) – moist scaling and fissuring in
toewebs, spreading to the sole and dorsal aspect of the foot
● Tinea manuum (tinea infection of the hand) – scaling and dryness
in the palmar creases
● Tinea capitis (scalp ringworm) – patches of broken hair, scaling
and inflammation
● Tinea unguium (tinea infection of the nail) – yellow discolouration,
thickened and crumbly nail
● Tinea incognito (inappropriate treatment of tinea infection with
topical or systemic corticosteroids) – Ill-defined and less scaly
lesions
● Candidiasis (candidal skin infection) – white plaques on mucosal
areas, erythema with satellite lesions in flexures
● Pityriasis/Tinea versicolor (infection with Malassezia furfur) – scaly
pale brown patches on upper trunk that fail to tan on sun
exposure, usually asymptomatic
Management ● Establish the correct diagnosis by skin scrapings, hair or nail
clippings (for dermatophytes); skin swabs (for yeasts)
● General measures: treat known precipitating factors (e.g.
underlying immunosuppressive condition, moist environment)
Skin Infections and Infestations
– Superfical fungal infections

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
40
● Topical antifungal agents (e.g. terbinafine cream)
● Oral antifungal agents (e.g. itraconazole) for severe, widespread,
or nail infections
● Avoid the use of topical steroids – can lead to tinea incognito
● Correct predisposing factors where possible (e.g. moist
environment, underlying immunosuppression)
Tinea corporis
Diffuse Tinea capitis
Tinea capitis
Tinea manuum (right hand)
Tinea pedis with associated tinea unguium
Candidiasis (right axilla)
Pityriasis versicolor
Skin Infections and Infestations
– Superfical fungal infections

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
41
• Skin cancer is one of the most common cancers.
• In general, skin cancer can be divided into: non-melanoma (basal cell carcinoma and
squamous cell carcinoma) and melanoma (malignant melanoma).
• Malignant melanoma is the most life-threatening type of skin cancer and is one of
the few cancers affecting the younger population.
• Sun exposure is the single most preventable risk factor for skin cancer.
Skin Cancer
Learning outcomes:
Ability to recognise:
- basal cell carcinoma
- squamous cell carcinoma
- malignant melanoma
Skin Cancer

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
42
Basal cell carcinoma
Description ● A slow-growing, locally invasive malignant tumour of the
epidermal keratinocytes normally in older individuals, only rarely
metastasises
● Most common malignant skin tumour
Causes ● Risk factors include UV exposure, history of frequent or severe
sunburn in childhood, skin type I (always burns, never tans),
increasing age, male sex, immunosuppression, previous history of
skin cancer, and genetic predisposition
Presentation ● Various morphological types including nodular (most common),
superficial (plaque-like), cystic, morphoeic (sclerosing), keratotic
and pigmented
● Nodular basal cell carcinoma is a small, skin-coloured papule or
nodule with surface telangiectasia, and a pearly rolled edge; the
lesion may have a necrotic or ulcerated centre (rodent ulcer)
● Most common over the head and neck
Management ● Surgical excision - treatment of choice as it allows histological
examination of the tumour and margins
● Mohs micrographic surgery (i.e. excision of the lesion and tissue
borders are progressively excised until specimens are
microscopically free of tumour) - for high risk, recurrent tumours
● Radiotherapy - when surgery is not appropriate
● Other e.g. cryotherapy, curettage and cautery, topical
photodynamic therapy, and topical treatment (e.g. imiquimod
cream) - for small and low-risk lesions
Complications ● Local tissue invasion and destruction
Prognosis ● Depends on tumour size, site, type, growth pattern/histological
subtype, failure of previous treatment/recurrence, and
immunosuppression
Basal cell carcinoma – nodular type
Skin Cancer – Basal cell carcinoma

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
43
Squamous cell carcinoma
Description ● A locally invasive malignant tumour of the epidermal
keratinocytes or its appendages, which has the potential to
metastasise
Causes ● Risk factors include excessive UV exposure, pre-malignant skin
conditions (e.g. actinic keratoses), chronic inflammation (e.g. leg
ulcers, wound scars), immunosuppression and genetic
predisposition
Presentation ● Keratotic (e.g. scaly, crusty), ill-defined nodule which may ulcerate
Management ● Surgical excision - treatment of choice
● Mohs micrographic surgery – may be necessary for ill-defined,
large, recurrent tumours
● Radiotherapy - for large, non-resectable tumours
Prognosis ● Depends on tumour size, site, histological pattern, depth
of invasion, perineural involvement, and immunosuppression
Squamous cell carcinoma – adjacent to ear (left) and glans penis (right)
Skin Cancer – Squamous cell carcinoma

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
44
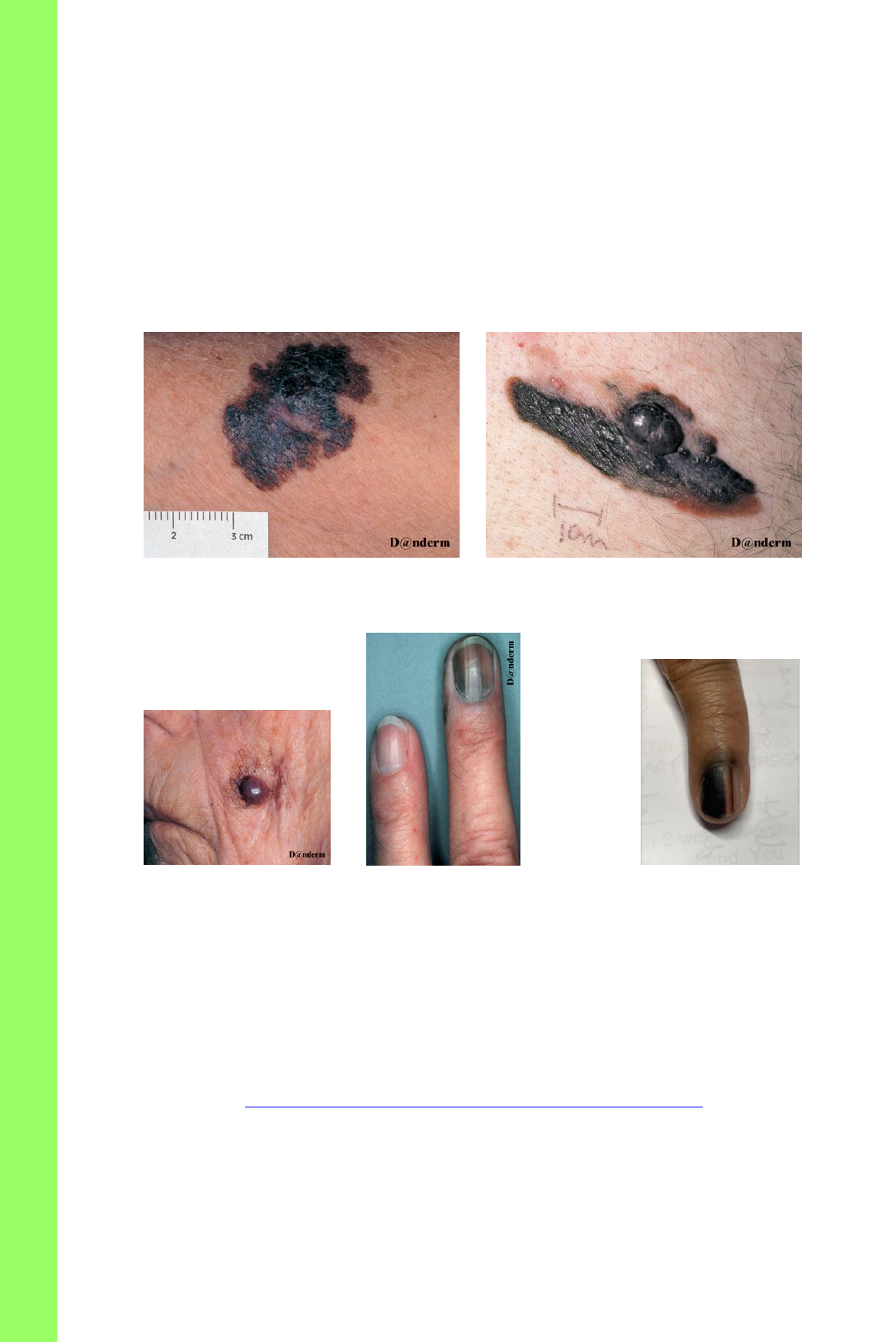
Malignant melanoma
Description ● An invasive malignant tumour of the epidermal melanocytes,
which has the potential to metastasise
Causes ● Risk factors include excessive UV exposure, skin type I (always
burns, never tans), history of > 100 moles or atypical neavus
syndrome moles, family history in first degree relative or previous
history of melanoma
Presentation ● The ‘ABCDE Symptoms’ rule (*major suspicious features):
Asymmetrical shape*
Border irregularity
Colour irregularity*
Diameter > 6mm
Evolution of lesion (e.g. change in size and/or shape)*
Symptoms (e.g. bleeding, itching)
● More common on the legs in women and trunk in men
Types ● Superficial spreading melanoma – common on the lower limbs,
in young and middle-aged adults; related to intermittent high-
intensity UV exposure; around 70% of all melanomas are superficial
spreading melanomas
● Nodular melanoma - common on the trunk, in young and middle-
aged adults; related to intermittent high-intensity UV exposure
● Lentigo maligna melanoma - common on the face, in elderly
population; related to long-term cumulative UV exposure
● Acral lentiginous melanoma - common on the palms, soles and nail
beds, in elderly population; no clear relation with UV exposure
Management ● Depends on the staging of melanoma (currently used system in
the UK - 2009 American Joint Committee of Cancer Staging System
(AJCC)). Stages I-IV are based on primary tumour Breslow thickness,
lymph node involvement and evidence of metastases. Stage I is the
earliest and stage IV is the most advanced)
● In general, surgical excision is the definitive treatment (often a
second surgery, wide local excision is needed after the initial
Skin Cancer – Malignant melanoma
Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
45
excision biopsy). Radiotherapy may sometimes be useful.
Chemotherapy is used for metastatic disease.
Prognosis ● Prognosis depends on the stage of melanoma and Breslow
thickness.
● In general, 90% of people diagnosed with melanoma in England and
Wales survived 10 years or more (Cancer Research UK, 2010-2011).
Superficial spreading melanoma Nodular melanoma
Lentigo maligna melanoma Acral lentiginous melanoma
Further reading: British Association of Dermatologists. Revised UK guidelines for the management of cutaneous
melanoma 2010. https://www.bad.org.uk/library-media%5Cdocuments%5CMelanoma_2010.pdf
Skin Cancer – Malignant melanoma
Acral lentiginous melanoma (in situ)
©by Matthew Scorer, licensed under CC BY-
NC-ND 4.0.

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
46
• Eczema, acne and psoriasis are chronic inflammatory skin disorders that follow a
relapsing and remitting course. There are many types of eczema but we shall just
consider atopic eczema here.
• These skin disorders are not infectious.
• Management is aimed at achieving control and not providing a cure.
• Complications are mainly due to the psychological and social effects.
• Patient education is important in these chronic skin conditions and should
concentrate on providing information about the nature of condition, aims of
treatment and the available treatment options.
Inflammatory Skin Conditions
Learning outcomes:
Ability to describe the presentation, demonstrate assessment, formulate a
differential diagnosis, instigate investigation and discuss how to provide
continuing care of:
- atopic eczema
- acne
- psoriasis
Inflammatory Skin Conditions

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
47
Atopic eczema
Description ● Eczema (or dermatitis) is a chronic skin condition common in
children but also prevalent in adults.
Epidemiology ● 20% prevalence in <12 years old in the UK
Causes ● Not fully understood, but a positive family history of atopy (i.e.
eczema, asthma, allergic rhinitis) is often present
● A primary genetic defect in skin barrier function (loss of function
variants of the protein filaggrin) appears to underlie atopic eczema
● Exacerbating factors such as infections, allergens (e.g. chemicals,
food, dust, pet fur), sweating, heat, occupation and severe stress
Presentation ● Acute presentation consists of itchy papules and vesicle often
weepy (exudative)
● Chronic lesions : dry scaly itchy patches can be erythematous in
paler skin or grey/ brown in richly pigmented skin
▪ More common on the face and extensor aspects of limbs in infants,
and the flexor aspects in children and adults
● In richly pigmented skin eczema may present as
brown, grey or purple bumps (papular eczema or follicular
eczema)
● Chronic scratching/rubbing leads to lichenification
● Across of skin types eczema can lead to
pigmentary changes such as hypopigmentation (reduced
pigmentation) and hyperpigmentation (increased pigmentation)
● Nail may show pitting and ridging of the nails
Management ● General measures - avoid known exacerbating agents, frequent
emollients +/- bandages and bath oil/soap substitute
● Topical therapies – topical steroids for active areas; topical
immunomodulators (e.g. tacrolimus, pimecrolimus) for
maintenance therapy as steroid-sparing agents
● Oral therapies - antihistamines for symptomatic relief, antibiotics
(e.g. flucloxacillin) for secondary bacterial infections, and
antivirals (e.g. aciclovir) for secondary herpes infection
Inflammatory Skin Conditions
– Atopic eczema

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
48
● Phototherapy and immunosuppressants (e.g. azathioprine,
ciclosporin, methotrexate) for severe non- responsive cases, biologic
therapy
Complications ● Secondary bacterial infection (crusted weepy lesions)
● Secondary viral infection - molluscum contagiosum (pearly
papules with central umbilication), viral warts and eczema
herpeticum (see page 34)
© Cardiff and Vale University Health Board.
Atopic eczema
Further reading: NICE. Eczema – Atopic, last updated Jan 2018. https://cks.nice.org.uk/eczema-atopic
Inflammatory Skin Conditions
– Atopic eczema

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
49
Acne vulgaris
Description ● An inflammatory disease of the pilosebaceous follicle
Epidemiology ● Over 80% of teenagers aged 13- 18 years
Causes ● Hormonal (androgen)
● Contributing factors include increased sebum production,
abnormal follicular keratinization, bacterial colonization
(Propionibacterium acnes) and inflammation
Presentation ● Non-inflammatory lesions (mild acne) - open and closed
comedones (blackheads and whiteheads)
● Inflammatory lesions (moderate and severe acne) - papules,
pustules, nodules, and cysts
● In richly pigmented skin:
1. Inflammatory lesions’ may not be so apparent, instead
hyperpigmented lesions (‘acne hyperpigmented
macules’) are seen.
Hyperpigmented lesions may also signify ongoing
inflammation
2. Non erythematous nodules may be present and detected by
palpation
● Commonly affects the face, chest and upper back
Comedones (Left and Middle) Papules and nodules (Right)
Management ● General measures - no specific food has been identified to cause
acne, treatment needs to be continued for at least 6 weeks to
produce effect
● Topical therapies (for mild acne) - benzoyl peroxide and topical
antibiotics (antimicrobial properties), and topical retinoids
Inflammatory Skin Conditions
– Acne vulgaris

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
50
(comedolytic and anti-inflammatory properties)
● Oral therapies (for moderate to severe acne) - oral antibiotics, and
anti-androgens (in females)
● Oral retinoids (for severe acne)
Complications ● Post-inflammatory hyperpigmentation, scarring, deformity,
psychological and social effects
Psoriasis
Description ● A chronic inflammatory skin disease due to hyperproliferation of
keratinocytes and inflammatory cell infiltration
Types ● Chronic plaque psoriasis is the most common type
● Other types include guttate (raindrop lesions), seborrhoeic
(naso-labial and retro-auricular), flexural (body folds), pustular
(palmar-plantar), and erythrodermic (total body redness)
Epidemiology ● Affects about 2% of the population in the UK
Causes ● Complex interaction between genetic, immunological and
environmental factors
● Precipitating factors include trauma (which may produce a
Köebner phenomenon), infection (e.g. tonsillitis), drugs, stress,
and alcohol
Presentation ● Well-demarcated erythematous scaly plaques
● in richly pigmented skin psoriasis can
present as dark brown, grey or purple patches or plaques
● Lesions can sometimes be itchy, burning or painful
● Common on the extensor surfaces of the body and over scalp
● Auspitz sign (scratch and gentle removal of scales cause capillary
bleeding)
● 50% have associated nail changes (e.g. pitting, onycholysis)
● 5-8% suffer from associated psoriatic arthropathy - symmetrical
polyarthritis, asymmetrical oligomonoarthritis, lone distal
interphalangeal disease, psoriatic spondylosis, and arthritis
mutilans (flexion deformity of distal interphalangeal joints)
Inflammatory Skin Conditions
– Psoriasis

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
51
Management ● General measures - avoid known precipitating factors, emollients
to reduce scales
● Topical therapies (for localised and mild psoriasis) - vitamin D
analogues, topical corticosteroids, coal tar preparations,
dithranol, topical retinoids, keratolytics and scalp preparations
● Phototherapy (for extensive disease) - phototherapy i.e. UVB and
photochemotherapy i.e. psoralen+UVA
● Oral therapies (for extensive and severe psoriasis, or psoriasis
with systemic involvement) - methotrexate, retinoids,
ciclosporin, mycophenolate mofetil, fumaric acid esters,
and biological agents (e.g. etanercept, adalimumab, ustekinumab)
(see page 71)
Complications ● Erythroderma (see page 33), psychological and social effects
Köebner phenomenon
Plaque Psoriasis
Plaque psoriasis
Nail changes and arthropathy
Scalp Psoriasis
Inflammatory Skin Conditions
– Psoriasis

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
52
• In general, blistering skin disorders can be divided into: immunobullous diseases
(e.g. bullous pemphigoid, pemphigus vulgaris), blistering skin infections (e.g. herpes
simplex) and other (e.g. porphyria cutanea tarda).
• The fragility of blisters depends on the level of split within the skin – an intra-
epidermal split (a split within the epidermis) causes blisters to rupture easily;
whereas a sub-epidermal split (a split between the epidermis and dermis) causes
blisters to be less fragile.
• The common causes of blisters are impetigo (see below), insect bites, herpes simplex
infection (see page 34), herpes zoster infection (see page 36), acute contact
dermatitis, pompholyx (vesicular eczema of the hands and feet, see below) and
burns.
• Bullous pemphigoid (see page 53) and pemphigus vulgaris (see page 54) are
uncommon conditions due to immune reaction within the skin.
Bullous impetigo in a new tattoo Pompholyx
Blistering Disorders
Learning outcomes:
1. Ability to recognise common causes of blisters
2. Ability to recognise:
- Bullous pemphigoid
- Pemphigus vulgaris
Blistering Disorders

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
53
Bullous pemphigoid
Description ● A blistering skin disorder which usually affects the elderly
Cause ● Autoantibodies against antigens between the epidermis and
dermis causing a sub-epidermal split in the skin
Presentation ● Tense, fluid-filled blisters on an erythematous base
● Lesions are often itchy
● May be preceded by a non-specific itchy rash
● Usually affects the trunk and limbs (mucosal involvement less
common)
Management ● General measures – wound dressings where required, monitor
for signs of infection
● Topical therapies for localised disease - topical steroids
● Oral therapies for widespread disease – oral steroids, combination
of oral tetracycline and nicotinamide, immunosuppressive agents
(e.g. azathioprine, mycophenolate mofetil, methotrexate, and
other)
Bullous pemphigoid
Blistering Disorders
– Bullous pemphigoid

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
54
Pemphigus vulgaris
Description ● A blistering skin disorder which usually affects the middle-aged
Cause ● Autoantibodies against antigens within the epidermis causing an
intra-epidermal split in the skin
Presentation ● Flaccid, easily ruptured blisters forming erosions and crusts
● Lesions are often painful
● Usually affects the mucosal areas (can precede skin involvement)
Management ● General measures – wound dressings where required, monitor for
signs of infection, good oral care (if oral mucosa is involved)
● Oral therapies – high-dose oral steroids, immunosuppressive
agents (e.g. methotrexate, azathioprine, cyclophosphamide,
mycophenolate mofetil, and other)
Pemphigus vulgaris
Pemphigus vulgaris affecting the oral mucosa
Blistering Disorders
– Pemphigus vulgaris

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
55
Pigmentary Disorders
• Pigmentary issues are a significant problem in all patients, how it differs in different
skin colour - population in the UK and it is important that medical students and
junior doctors appreciate the dermatoses pertinent to these groups.
• In general, a pigment change can present as hypopigmentation (reduced
pigmentation), depigmentation (complete loss of pigment), or hyperpigmentation
(increased pigmentation).
• Below are some of the common pigmentary disorders which can cause significant
embarrassment and distress especially in the darker skin types.
Vitiligo
Description ● An acquired depigmenting disorder, where there is complete loss
of pigment cells (melanocytes)
Cause ● Thought to be an autoimmune disorder, where the innate
immune system causes destruction or loss of melanocytes, leading
to loss of pigment formation in the skin
Presentation ● Presentation at any age
• A single patch or multiple patches of depigmentation (complete loss
of pigment), often symmetrical
● Common sites are exposed areas such as face, hands, feet, as well
as body folds and genitalia
● Favours sites of injury and this phenomenon is called the Koebner
phenomenon
Management ● Minimise skin injury as a cut, graze, or sunburn can potentially
trigger a new patch of vitiligo
● Topical treatments such as topical steroids and calcineurin
inhibitors (such as topical tacrolimus and pimecrolimus)
Learning objectives:
1. Ability to formulate a differential diagnosis, describe the investigation and
discuss the management in patients with:
- vitiligo
- melasma
Pigmentary Disorders
– Vitiligo

Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists
56
● Phototherapy such as UVB therapy, excimer laser
● Oral immunosuppressants such as methotrexate, ciclosporin and
mycophenolate mofetil
Melasma
Description ● An acquired chronic skin disorder, where there is increased
pigmentation in the skin
Cause ● Thought to be due to genetic predisposition, and triggered by
factors such as sun exposure, hormonal changes such as pregnancy
and contraceptive pills
● The pigmentation is caused by an overproduction of pigment
(melanin) by pigment cells (melanocytes)
Presentation ● Brown macules (freckle-like spots) or larger patches with an
irregular border
● Symmetrical distribution
● Common sites are forehead, cutaneous upper lips and cheeks,
rarely can occur on neck, shoulders and upper arms
Management ● Lifelong sun protection
● Discontinuation of hormonal contraceptive pills
● Cosmetic camouflage
● Topical treatments that aim at inhibiting the formation of new
melanin such as hydroquinone, azelaic acid, kojic acid (a chelating
agent) and vitamin C
● Laser treatments need to be used with caution as the heat
generated by lasers can potentially cause post-inflammatory
hyperpigmentation.
Pigmentary Disorders
– Melasma

Dermatology: Handbook for medical students & junior doctors
57 British Association of Dermatologists
• There are several commonly-encountered skin problems in clinical practice. Below
are some of the important differential diagnoses for each of these presentations.
• Clinical exposure is the key to achieve competence in diagnosing, investigating and
managing these skin problems.
Common Important Problems
Learning objectives:
Ability to formulate a differential diagnosis, describe the investigation and
discuss the management in patients with:
- chronic leg ulcers
- itchy eruption
- a changing pigmented lesion
- purpuric eruption
- a red swollen leg
- keloid scars
Common Important Problems

Dermatology: Handbook for medical students & junior doctors
58 British Association of Dermatologists
Chronic leg ulcers
• Leg ulcers are classified according to aetiology. In general, there are three main types: venous, arterial and neuropathic ulcers. Other causes include
vasculitic ulcers (purpuric, punched out lesions), infected ulcers (purulent discharge, may have systemic signs) and malignancy (e.g. squamous cell
carcinoma in long-standing non-healing ulcers).
• In clinical practice, there can be mixture of arterial, venous and/or neuropathic components in an ulcer.
Venous ulcer
© Cardiff and Vale University Health Board.
Venous ulcer
Arterial ulcer
Neuropathic ulcer
Common Important Problems
– Chronic leg ulcers

Dermatology: Handbook for medical students & junior doctors
59 British Association of Dermatologists
Chronic leg ulcers
Venous ulcer
Arterial ulcer
Neuropathic ulcer
History
- Often painful, worse on standing
- History of venous disease e.g. varicose
veins, deep vein thrombosis
- Painful especially at night, worse when
legs are elevated
- History of arterial disease e.g.
atherosclerosis
- Often painless
- Abnormal sensation
- History of diabetes or neurological
disease
Common sites
- Malleolar area (more common over
medial than lateral malleolus)
- Pressure and trauma sites e.g. pretibial,
supramalleolar (usually lateral), and at
distal points e.g. toes
- Pressure sites e.g. soles, heel, toes,
metatarsal heads
Lesion
- Large, shallow irregular ulcer
- Exudative and granulating base
- Small, sharply defined deep ulcer
- Necrotic base
- Variable size and depth
- Granulating base
- May be surrounded by or underneath a
hyperkeratotic lesion (e.g. callus)
Associated
features
- Warm skin
- Normal peripheral pulses
- Leg oedema, haemosiderin and melanin
deposition (brown pigment),
lipodermatosclerosis, and atrophie
blanche (white scarring with dilated
capillaries)
- Cold skin
- Weak or absent peripheral pulses
- Shiny pale skin
- Loss of hair
- Warm skin
- Normal peripheral pulses*
*cold, weak or absent pulses if it is a
neuroischaemic ulcer
- Peripheral neuropathy
Possible
investigations
- Normal ankle/brachial pressure index
(i.e. ABPI 0.8-1)
- ABPI < 0.8 - presence of arterial
insufficiency
- Doppler studies and angiography
- ABPI < 0.8 implies a neuroischaemic
ulcer
- X-ray to exclude osteomyelitis
Management
- Compression bandaging
(after excluding arterial insufficiency)
- Vascular reconstruction
- Compression bandaging is
contraindicated
- Wound debridement
- Regular repositioning, appropriate
footwear and good nutrition
Common Important Problems
– Chronic leg ulcers

Dermatology: Handbook for medical students & junior doctors
60 British Association of Dermatologists
Itchy eruption
• An itchy (pruritic) eruption can be caused by an inflammatory condition (e.g. eczema), infection (e.g. varicella), infestation (e.g. scabies), allergic
reaction (e.g. some cases of urticaria) or an unknown cause, possibly autoimmune (e.g. lichen planus).
Chronic fissured hand eczema
Scabies
Urticaria
R © Cardiff and Vale University Health Board.
© Cardiff and Vale University Health Board.
Lichen planus
Lichen planus
Wickham’s striae
Note that lichen planus in darker skin types has a typical purplish tinge.
Dermatology: Handbook for medical students & junior d
octors
Common Important Problems
– Itchy eruption

Dermatology: Handbook for medical students & junior doctors
61 British Association of Dermatologists
Itchy eruption
Eczema
Scabies
Urticaria
Lichen planus
History
- Personal or family history of
atopy
- Exacerbating factors (e.g.
allergens, irritants)
- May have history of contact
with symptomatic individuals
- Pruritus worse at night
- Precipitating factors (e.g.
food,
contact, drugs)
- Family history in 10% of cases
- May be drug-induced
Common sites
- Variable (e.g. flexor aspects in
children and adults with
atopic eczema)
Lichen nitidus pattern in darker
skin
- Sides of fingers, finger webs,
wrists, elbows, ankles, feet,
nipples and genitals
- No specific tendency
- Forearms, wrists, and legs
- Always examine the oral
mucosa
Lesion
- Dry, erythematous patches
- Acute eczema is
erythematous, vesicular and
exudative
- Linear burrows (may be
tortuous) or rubbery nodules
- Pink wheals (transient)
- May be round, annular, or
polycyclic
- Violaceous (lilac) flat-topped
Papules or hyperpigmented
papules (in darker skin)
- Symmetrical distribution
Associated
features
- Secondary bacterial or viral
infections
- Secondary eczema and
impetigo
- May be associated with
angioedema or anaphylaxis
- Nail changes and hair loss
- Lacy white streaks on the oral
mucosa and skin lesions
(Wickham’s striae)
Possible
investigations
- Patch testing
- Serum IgE levels
- Skin swab
- Skin scrape, extraction of
mite and view under
microscope
- Bloods and urinalysis to
exclude a systemic cause
- Skin biopsy
Management
- Emollients
- Corticosteroids
- Immunomodulators
- Antihistamines
- Scabicide (e.g. permethrin
or malathion)
- Antihistamines
- Antihistamines
- Corticosteroids
- Corticosteroids
- Antihistamines
Dermatology: Handbook for medical students & junior d
octors
Common Important Problems
– Itchy eruption

Dermatology: Handbook for medical students & junior doctors
62 British Association of Dermatologists
A changing pigmented lesion
• A changing pigmented lesion can be benign (e.g. melanocytic naevi, seborrhoeic wart) or malignant (e.g. malignant melanoma).
Congenital naevus Seborrhoeic keratoses Malignant melanoma
Common Important Problems
– A changing pigmented lesion

Dermatology: Handbook for medical students & junior doctors
63 British Association of Dermatologists
A changing pigmented lesion
Benign
Malignant
Melanocytic naevi
Seborrhoeic wart
Malignant melanoma
History
- Not usually present at birth but develop
during infancy, childhood or adolescence
- Asymptomatic
- Tend to arise in the middle-aged or elderly
- Often multiple and asymptomatic
- Tend to occur in adults or the middle-aged
- History of evolution of lesion
- May be symptomatic (e.g. itchy, bleeding)
- Presence of risk factors
Common sites
- Variable
- Face and trunk
- More common on the legs in women and
trunk in men
- Darker skin tomes acral sites
Lesion
- Congenital naevi may be large,
pigmented, protuberant and hairy
- Junctional naevi are small, flat and dark
- Intradermal naevi are usually dome-shape
papules or nodules
- Compound naevi are usually raised, warty,
hyperkeratotic, and/or hairy
- Warty greasy papules or nodules
- ‘Stuck on’ appearance, with well-defined
edges
- Features of ABCDE:
Asymmetrical shape
Border irregularity
Colour irregularity
Diameter > 6mm
Evolution of lesion
Management
- Only if symptomatic
Shave or complete excision
- Only if symptomatic
Curette and cautery
Cryotherapy
- Local Excision
Treatment based on Breslow Thickness
Common Important Problems
– A changing pigmented lesion

Dermatology: Handbook for medical students & junior doctors
64 British Association of Dermatologists
Purpuric eruption
• A purpuric eruption can be thrombocytopenic (e.g. meningococcal septicaemia, disseminated intravascular coagulation, idiopathic
thrombocytopenic purpura) or non-thrombocytopenic e.g. trauma, drugs (e.g. steroids), aged skin, vasculitis (e.g. Henoch-Schönlein
purpura).
Henoch-Schönlein purpura Actinic purpura
Common Important Problems
– Purpuric
eruption

Dermatology: Handbook for medical students & junior doctors
65 British Association of Dermatologists
Purpuric eruption
Meningococcal septicaemia
Disseminated intravascular
coagulation
Vasculitis
Actinic purpura
History
- Acute onset
- Symptoms of meningitis and
septicaemia
- History of trauma,
malignancy,
sepsis, obstetric
complications,
transfusions, or liver failure
- Painful lesions
- Arise in the elderly population
with sun-damaged skin
Common sites
- Extremities
- Spontaneous bleeding from
ear, nose and throat,
gastrointestinal tract,
respiratory tract or wound
site
- Dependent areas (e.g. legs,
buttocks, flanks)
- Extensor surfaces of hands
and forearms
- Such skin is easily traumatised
Lesion
- Petechiae, ecchymoses,
haemorrhagic bullae and/or
tissue necrosis
- Petechiae, ecchymoses,
haemorragic bullae and/or
tissue necrosis
- Palpable purpura (often
painful)
- Non-palpable purpura
- Surrounding skin is atrophic
and thin
Associated
features
- Systemically unwell
- Systemically unwell
- Systemically unwell
- Systemically well
Possible
investigations
- Bloods
- Lumbar puncture
- Bloods (a clotting screen is
important)
- Bloods and urinalysis
- Skin biopsy
- No investigation is needed
Management
- Antibiotics
- Treat the underlying cause
- Transfuse for coagulation
deficiencies
- Anticoagulants for thrombosis
- Treat the underlying cause
- Steroids and
immunosuppressants if there
is systemic involvement
- No treatment is needed
Dermatology: Handbook for medical students & junior d
octors
Dermatology: Handbook for medical stud Dermatology: Handbook for medical students & junior d
octors ent s & junior doctors
Common Important Problems
– A red swollen leg
Common Important Problems
– Purpuric
eruption

Dermatology: Handbook for medical students & junior doctors
66 British Association of Dermatologists
A red swollen leg
• The main differential diagnoses for a red swollen leg are cellulitis, erysipelas, venous thrombosis and chronic venous insufficiency.
Cellulitis/Erysipelas
Venous thrombosis
Chronic venous insufficiency
History
- Painful spreading rash
- History of abrasion or ulcer
- Pain with swelling and redness
- History of prolonged bed rest, long haul
flights or clotting tendency
- Heaviness or aching of leg, which is
worse on standing and relieved by
walking
- History of venous thrombosis
Examination
- Erysipelas (well-defined edge)
- Cellulitis (diffuse edge)
- Complete venous occlusion may lead to
cyanotic discolouration
- Discoloured (blue-purple)
- Oedema (improved in the morning)
- Venous congestion and varicose veins
Associated
features
- Systemically unwell with fever and
malaise
- May have lymphangitis
- Usually systemically well
- May present with pulmonary embolism
- Lipodermatosclerosis (erythematous
induration, creating ‘champagne
bottle’ appearance)
- Stasis dermatitis (eczema with
inflammatory papules, scaly and
crusted erosions)
- Haemosiderin deposition
- Venous ulcer
Possible
investigations
- Anti-streptococcal O titre (ASOT)
- Skin swab
- D-dimer
- Doppler ultrasound and/or venography
- Doppler ultrasound and/or venography
Management
- Antibiotics
- Anticoagulants
- Leg elevation and compression
stockings
- Sclerotherapy or surgery for varicose
veins
Dermatology: Handbook for medical students & junior d
octors
Dermatology: Handbook for medical stud Dermatology: Handbook for medical students & junior d
octors ent s & junior doctors
Common Important Problems
– A red swollen leg
Common Important Problems
– A red swollen leg

Dermatology: Handbook for medical students & junior doctors
67 British Association of Dermatologists
Keloid Scars
Description ● An overgrowth of scar tissue, which tends to be larger than the original wound itself
Cause ● Thought to be due to overproduction of collagen during wound healing after minor injuries, skin surgery, insect bites and acne
spots in genetically predisposed individuals
● More commonly seen in darker skin types
Presentation ● Firm, smooth, hard nodule which can be itchy or painful
● Common sites are chest and shoulders
Management ● Avoidance of further trauma to the skin such as scratching
● Topical treatments such as topical steroids and silicone gel can potentially flatten the scar, and improve the symptoms
● Intralesional steroid injection if topical treatments are not effective
● Surgery such as excision needs to be carried out only as the last resort and with caution as the new wound may cause a larger
keloid scar
Common Important Problems – Keloid Scars

Dermatology: Handbook for medical students & junior doctors
68 British Association of Dermatologists
Management and therapeutics
• Treatment modalities for skin disease can be broadly categorised into medical
therapy (topical and systemic treatments) and physical therapy (e.g. cryotherapy,
phototherapy, photodynamic therapy, lasers and surgery).
• Topical treatments directly deliver treatment to the affected areas and this reduces
systemic side effects. It is suitable for localised and less severe skin conditions. They
consist of active constituents which are transported into the skin by a base (also
known as a ‘vehicle’). Examples of active ingredients are steroids, tar,
immunomodulators, retinoids, and antibiotics. The common forms of base are lotion
(liquid), cream (oil in water), gel (organic polymers in liquid, transparent), ointment
(oil with little or no water) and paste (powder in ointment).
• Systemic therapy is used for extensive and more serious skin conditions, if the
treatment is ineffective topically or if there is systemic involvement. However, they
have the disadvantage of causing systemic side effects.
Management
Learning objectives:
Ability to describe the principles of use of the following drugs:
- emollients
- topical/oral corticosteroids
- oral aciclovir
- oral antihistamines
- topical/oral antibiotics
- topical antiseptics
- biological therapy
- Oral retinoids
Management

Dermatology: Handbook for medical students & junior doctors
69 British Association of Dermatologists
Emollients
Examples ● Aqueous cream, emulsifying ointment, liquid paraffin and white soft
paraffin in equal parts (50:50)
Quantity ● 500 grams per tub
Indications ● To rehydrate skin and re-establish the surface lipid layer
● Useful for dry, scaling conditions and as soap substitutes
Side effects ● Reactions may be irritant or allergic (e.g. due to preservatives or perfumes
in creams)
Topical/Oral corticosteroids
Examples ● Topical steroids: classified as mildly potent (e.g, hydrocortisone),
moderately potent (e.g. clobetasone butyrate (Eumovate)), potent
(e.g.betamethasone valerate (Betnovate)), and very potent (e.g. clobetasol
propionate (Dermovate))
● Oral steroids: prednisolone
Quantity ● Usually 30 grams per tube (enough to cover the whole body once)
Indications ● Anti-inflammatory and anti-proliferative effects
● Useful for allergic and immune reactions, inflammatory skin conditions,
blistering disorders, connective tissue diseases, and vasculitis
Side effects ● Local side effects (from topical corticosteroids): skin atrophy (thinning),
telangiectasia, striae, may mask, cause or exacerbate skin infections,
acne, or perioral dermatitis, and allergic contact dermatitis.
● Systemic side effects (from oral corticosteroids): Cushing’s syndrome,
immunosuppression, hypertension, diabetes, osteoporosis, cataract, and
steroid-induced psychosis
Oral aciclovir
Examples ● Aciclovir
Indications ● Viral infections due to herpes simplex and herpes zoster virus
Side effects ● Gastrointestinal upsets, raised liver enzymes, reversible neurological
reactions, and haematological disorders
Management – Emollients, Topical/Oral corticosteroids, Oral acyclovir, Oral antihistamines

Dermatology: Handbook for medical students & junior doctors
70 British Association of Dermatologists
Oral antihistamines
Examples ● Classified into nonsedative (e.g. cetirizine, loratadine) and sedative
antihistamines (e.g. chlorpheniramine, hydroxyzine)
Indications ● Block histamine receptors producing an anti-pruritic effect
● Useful for type-1 hypersensitivity reactions and eczema (especially
sedative antihistamines for children)
Side effects ● Sedative antihistamines can cause sedation and anticholinergic effects
(e.g. dry mouth, blurred vision, urinary retention, and constipation)
Topical/Oral antibiotics
Examples ● Topical antibiotics: fusidic acid, mupirocin (Bactroban), neomycin
● Oral antibiotics: penicillins, cephalosporins, gentamicin, macrolides,
nitrofurantoin, quinolones, tetracyclines, vancomycin, metronidazole,
trimethoprim
Indications ● Useful for bacterial skin infections, and some are used for acne
Side effects ● Local side effects (from topical antibiotics): local skin irritation/allergy
● Systemic side effects (from oral antibiotics): gastrointestinal upset, rashes,
anaphylaxis, vaginal candidiasis, antibiotic-associated infection such as
Clostridium difficile, and antibiotic resistance (rapidly appears to fusidic
acid)
Topical antiseptics
Examples ● Chlorhexidine, cetrimide, povidone-iodine
Indications ● Treatment and prevention of skin infection
Side effects ● Local side effects: local skin irritation/allergy
Oral retinoids
Examples ● Isotretinoin, Acitretin
Indications ● Acne, psoriasis, and disorders of keratinisation
Side effects ● Mucocutaneous reactions such as dry skin, dry lips and dry eyes,
disordered liver function, hypercholesterolaemia, hypertriglyceridaemia,
myalgia, arthralgia and depression
● Teratogenicity: effective contraception must be practised one month
Management – Oral antihistamines, Topical/Oral antibiotics, Topical antiseptics, Oral retinoids

Dermatology: Handbook for medical students & junior doctors
71 British Association of Dermatologists
before, during and at least one month after isotretinoin, but for two years
after Acitretin (consult current BNF for further details)
Biological Therapy Management
Examples Monoclonal antibodies (eg. Infliximab, Adalimumab, Ustekinumab,
Certolizumab, Gorlilumab), Fusion antibody proteins (eg. Etanercept),
Recombinant human cytokines and growth factors (eg. Interleukins)
Indications ● Mainly for psoriasis, atopic dermatitis and hidradenitis suppurativa
Side effects ● Local side effects: redness, swelling, bruising at the site of injection
● Systemic side effects: allergic reactions, antibody formation, flu-like
symptoms, infections, hepatitis, demyelinating disease, heart failure, blood
problems, rare reports of cancers (eg. non-melanoma skin cancers,
lymphoma)
Management – Biological Therapy

Dermatology: Handbook for medical students & junior doctors
72 British Association of Dermatologists
• There are four main aspects to focus on in clinical practice:
i) Patient education, particularly on the nature of disease, treatment and
ways to achieve full compliance and effectiveness, and prevention strategies
ii) Effective written communication to general practitioner so that patient care
can be continued appropriately
iii) Good prescribing skills
iv) Good clinical examination and appropriate investigations to facilitate
accurate diagnosis
Practical Skills
Learning objectives:
1. Ability to perform the following tasks:
- explain how to use an emollient or a topical corticosteroid
- make a referral
- write a discharge letter
- write a prescription for emollient
- take a skin swab
- take a skin scrape
2. Describe the principles of prevention in:
- pressure sores
- sun damage and skin cancer
Practical Skills

Dermatology: Handbook for medical students & junior doctors
73 British Association of Dermatologists
Patient education
How to use emollients
● Apply liberally and regularly
How to use topical corticosteroids
● Apply thinly and only for short-term use (often 1 or 2 weeks only)
● In general, use 1% hydrocortisone or mild-moderate potent topical
steroids on the face and thin skin areas eg. neck and flexures.
● Fingertip unit (advised on packaging) – strip of cream the length of a
fingertip
Preventing pressure sores
● Pressure sores are due to ischaemia resulting from localised damage to
the skin caused by sustained pressure, friction and moisture, particularly
over bony prominences.
● Preventative measures involve frequent repositioning, nutritional support,
and use of pressure relieving devices e.g. special beds
Preventing sun damage and skin cancer
● Excessive exposure to UV radiation is the most significant
and preventable risk factor for the development of skin cancer (Table 14)
● Skin types I and II are at higher risk of developing skin cancer with
excessive sun exposure than other skin types (Table 15)
Table 14. SMART ways to avoid excessive sun exposure
Spend time in the shade between 11am-3pm
Make sure you never burn
Aim to cover up with a t-shirt, wide-brimmed hat and sunglasses
Remember to take extra care with children
Then use Sun Protection Factor (SPF) 30+ sunscreen
Practical Skills
– Patient education

Dermatology: Handbook for medical students & junior doctors
74 British Association of Dermatologists
Table 15. Fitzpatrick Skin phototype
Skin types Description
I Always burns, never tans
II Always burns, sometimes tans
III Sometimes burns, always tans
IV Never burns, always tans
V Tans very easily, very rarely burns
VI tans very easily, never burns
Written communication
Writing a referral letter
Important points to include:
● Reason(s) for referral, current presentation, and impact of disease
● Patient’s medical and social background
● Current and previous treatment, length of treatment, and response to
treatment
Writing a discharge letter
Important points to include:
● Reason(s) for admission and current presentation
● Hospital course
● Investigation results
● Diagnostic impression
● Management plan (including treatment and follow-up appointment)
● Content of patient education given
Prescribing skills
Writing a prescription
General tips:
● Include drug name, dose, frequency and an intended duration/review date
● 30 grams of cream/ointment covers the whole adult body area
● 1 fingertip unit covers the area of two palms and equals ½ gram
Practical Skills
– Written communication and prescribing skills

Dermatology: Handbook for medical students & junior doctors
75 British Association of Dermatologists
Prescribing emollients
General tips
● Emollients come in 500 gram tubs
● In general, ointment-based emollients are useful for dry, scaling skin
whereas creams and lotions are for red, inflamed and weeping lesions
Prescribing topical corticosteroids
General tips
● Prescribe the weakest potency corticosteroid that is effective
● Use only for short term
● Need to specify the base i.e. cream, lotion or ointment
Clinical examination and investigations
Taking a skin swab
• Skin swabs can be taken from vesicles, pustules, erosions, ulcers and mucosal
surfaces for microbial culture.
• Surface swabs are generally not encouraged.
Taking a skin scrape
• Skin scrapes are taken from scaly lesions by gentle use of a scalpel in suspected
fungal infection (to show evidence of fungal hyphae and/or spores) and from
burrows in scabies (see page 60).
Measuring ankle-brachial pressure index (ABPI)
• ABPI is used to identify the presence and severity of peripheral arterial insufficiency,
which is important in the management of leg ulcers.
• Measure the cuff pressure of dorsalis pedis or posterior tibial artery using a Doppler
and compare it to the pressure of brachial artery.
• The ABPI is measured by calculating the ratio of highest pressure obtained from the
ankle to highest brachial pressure of the two arms and is normally >0.8.
• Inappropriately high reading will be obtained in calcified vessels (often in diabetics).
Practical Skills
– Clinical examination and investigations
Dermatology: Handbook for medical students & junior doctors
76 British Association of Dermatologists
1. Verbov J Dermatological disorders. In: Lissauer T, Carroll W eds. Illustrated Textbook
of Paediatrics. 5th Edition: 2018: Chap25: 442-52. Elsevier.
2. British Association of Dermatologists guidelines and patient information leaflets.
We wish to acknowledge the following contributors:
• Dr Tanya Bleiker, President (2020-2022) and Prof Mini Singh, Undergraduate
workstream Chair of the British Association of Dermatologists, for writing the
Foreword to the 3
rd
edition.
• Mark Goodfield, former President (2008-2010) of the British Association of
Dermatologists, for writing the Foreword to the 1
st
edition.
• Dr Niels K. Veien for allowing us to use his photographs. All illustrations in this
handbook were obtained from "D@nderm" with his permission.
• Dr Susan Burge OBE, retired Consultant Dermatologist, Oxford Radcliffe Hospitals
NHS Trust, Professor Peter Friedmann, Emeritus Professor of Dermatology,
Southampton General Hospital, and Professor Lesley Rhodes, Professor of
Experimental Dermatology, University of Manchester for reviewing and contributing
valuable suggestions.
• Mr Kian Tjon Tan, Consultant Plastic Surgeon, Calderdale and Huddersfield NHS
Foundation Trust for contributing the chapter Background Knowledge.
• Dr Yi Ning Chiang, Specialist Trainee in Dermatology, Salford Royal NHS Foundation
Trust for contributing the chapter Common Important Problems.
• Dr Matthew Scorer, Locum Consultant Dermatologist, University Hospitals of
Leicester for allowing us to use his photographs in this handbook. All illustrations
used are with his permission.
• The Cardiff and Vale University Health Board for allowing us to use their photographs
in this handbook. All illustrations used are with their permission.
• DermNet NZ for allowing us to use their photographs in this handbook. All
illustrations used are with their permission.
Acknowledgements
General References
Dermatology: Handbook for medical students & junior doctors
British Association of Dermatologists

