1
MBBS
Year 4
GUIDE TO HISTORY TAKING
AND EXAMINATION
2015-16
Copyright University College London Medical School
University College London
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
2
Contents
The Medical History ................................................................................ 3
How to take a Respiratory History ..................................................... 12
How to take a Cardiovascular History ............................................... 13
How to take a Locomotor History ....................................................... 14
How to take a history of pain ............................................................... 14
Presenting patients Workshop ............................................................. 15
General Tips on How to Perform an Examination ........................... 16
Dress and Behaviour Expected in Clinical Area ............................... 18
Cardiovascular Examination ................................................................ 19
Respiratory Examination ...................................................................... 24
Abdominal Examination ....................................................................... 26
Musculoskeletal Examination- GALS Screen ................................... 30
Motor Examination of Lower Limbs ................................................... 32
Examination of the Upper Limbs ........................................................ 35
Sensory Examination of Lower Limbs ................................................ 38
Cranial Nerve Examination .................................................................. 41
Ophthalmology - How to measure visual acuity .............................. 44
Examination using an Ophthalmoscope with a patient................... 45
How to record your clinical notes ....................................................... 47
How to measure Blood Pressure……… ……………………………49
How to perform urinalysis………………………………………......50

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
3
The Medical History
‘The medical history’ is a structured assessment conducted to generate a comprehensive
picture of a patient’s health and health problems. It includes an assessment of:
the patient’s current and previous health problems
current and previous medical treatment
the patient’s health in general
factors which might affect the patient’s health and their response to prevention or
treatment of health problems (e.g. risk factors, lifestyle issues)
their family’s health
Taking together the history, information from the physical examination and any
investigations or tests, this should provide all the information needed to make a diagnosis
(i.e. to identify the nature of a health problem). Making a diagnosis is often a preoccupation
of clinical students, however, it is important to remember that a clerking (i.e. an assessment in
which a medical history is taken) provides much more information than this. This
consultation should include questioning about the patient’s perspective of their situation (an
often-used mnemonic being ‘ICE’ - Ideas, Concerns and Expectations).
The patient’s perspective affects:
their response to information and recommended treatment
the working relationship between the doctor (or team) and the patient
Recent initiatives by the government and other institutions (e.g. the Department of Health’s
NHS Plan, 2000; the GMC’s Duties of a Doctor) have emphasised the importance of involving
the patient at every stage in their care.
As a medical student you often have very defined goals:
to practise how to ‘take a history’
to get information so you can identify a sensible differential diagnosis
to give a clear case presentation to your firm
to give a good impression to your consultant and colleagues
Be aware that as a doctor you will also need to consider:
the impact of the patient’s health problem on their life
the complex interplay between their current health problem, any chronic health
problems, their lifestyle and risk factors, their social and family situation – and how
this affects their health in the long-term
their short- and long-term relationship with health care providers, including you
their response to information and recommended treatment
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
4
The Medical History – Common Misconceptions
There is often confusion about what ‘a medical history’ is, because the term is used for
different things. It can mean:
the whole consultation in which information is gathered (i.e. including both the
process of communication, and the content, i.e. the information gathered)
only the clinical content (the medical information) which is gleaned during the
consultation
a written or presented version of the information gathered (e.g. in medical notes, a
student case presentation)
These are all very different – the key point being that how you conduct a consultation to
gather information to obtain ‘a medical history’ is not the same as how you subsequently
record it or communicate it to colleagues.
Common problems
1. Trying to gather the information in the order in which it is written or presented. The
information communicated to colleagues is a concise summary, presented in a
logical, linear manner. Consultations, whilst structured, allow the information to
unfold more slowly, often with parts being covered in a different order (e.g. the
patient may start their story with the onset of a problem some time ago, not their
current presenting symptom). Sometimes an additional line of questioning occurs to
you later, and you have to revisit a part of the history. In addition, there may be
much clarification of terminology used – such as the patient’s description of their
symptoms – which in the notes might be summarised simply as ‘complains of
pressing pain in chest’.
You will have training in how to structure the consultation, but be aware that you are
not expected to cover everything in the same order in the consultation as in a
subsequent case presentation.
Example: At the start of a case presentation, you might begin with the patient’s age,
gender, occupation and marital status. However, asking the patient’s occupation and
marital status as your second and third questions can appear intrusive and/or
irrelevant - the patient is expecting to tell you about their medical problem first. It is
more appropriate to ask about these later on in the consultation, when you are
opening up the discussion to talk more generally about their lifestyle.
2. Clinical students become rapidly socialised into the use of medical jargon, which is
then unintentionally used with patients. Case presentations and medical notes are
full of jargon; it is concise. Consultations should not be.
Example: The word ‘history’. You would not, in a consultation, start a line of
questioning by saying ‘Now, what about your social history?’. You would say ‘I’d
just like to ask you about your life in general, to get a better picture of your health.
First of all, who’s at home with you?…’
Other common jargon to avoid: ‘drugs’ (meaning prescribed or over the counter
medication), and reading straight from a list whilst doing your systems review (e.g.
‘anything associated with this?’, ‘does it radiate?’).

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
5
3. Experienced doctors obtain the clinical history in a problem-solving manner which is
based on testing a hypothesis. It is still necessary to ask all the usual questions about
a symptom (e.g. onset, course, severity, associated symptom, previous episodes etc.)
but the format of the history of the presenting problem should be problem based. In
order to perform the problem solving method competently, it is necessary to have
knowledge of the causes of each symptom and the symptoms of each disease. This
style of history taking is something to work towards as you gain experience.
The Medical History – Content and Process
The Professional Development Spine uses the Calgary-Cambridge Guide to the Medical
Interview, which integrates both the content (clinical information) and process
(communication) of the consultation. A card summarising the Guide will be given out during
the Introductory Course.
Recommended further reading:
Silverman J, Kurtz S, Draper J (2005) Skills for Communicating with Patients (2nd ed).
Oxford: Radcliffe Publishing. (essential textbook)
www.skillscascade.com/handouts/Calgarycambridgeframework.pdf
www.skillscascade.com/handouts/CalgaryCambridgeGuide.pdf (downloadable
handouts)
Initiating the consultation
1. Check the setting
Find a chair (do not sit on the bed, do not stand over the patient)
Consider ambient noise and privacy (can you be overheard?)
2. Establish initial rapport
Be approachable and friendly – it helps to begin with a smile and an ice-breaker (i.e. a
comment about a non-medical topic)
Greet the patient with their title and surname, and check you are using their
preferred form of address
Introduce yourself – full name and role (e.g. third year medical student)
Explain reason for interview (e.g. to practise gathering information)
Seek consent - if they decline, thank them and leave
Seek consent for taking notes, explain information is passed on to doctor
Demonstrate respect and interest, attend to the patient’s physical comfort and
privacy (e.g. would they like the curtain drawn?)
3.Identify the reason for their attendance
Open question to identify the patient’s current problem/reason for attending
Listen attentively to the opening statement without interruption
Acknowledge problem(s) mentioned (i.e. reflect back)
Do not engage in detailed questioning at this point – you are establishing a problem
list
Query whether there are other problems – acknowledge and repeat until no further
problems are mentioned
Write down each problem as it is mentioned
Summarise the problem list back to the patient

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
6
Negotiate an agenda / explain your wish to gather information about the problems in
detail and their health in general
Keynote: The problems that patients mention may not all be symptoms – they may be
questions or concerns. You are not expected to solve these and must not ignore them. You
should gather information about them – in the same way as you do for the other problems –
and explain that you will then pass this on to their doctor.
Gathering information
1. Explore the patient’s problems
Encourage the patient to tell the story from when it first started
Use open questions at the start, clarifying with closed questions later
Show that you are listening – make eye contact while the patient is talking, tailor
your questions to the information being given, reflect back what the patient is saying
and periodically summarise
Encourage the patient to talk – if you leave space, the patient will talk
Pick up verbal and non-verbal cues indicating that there is something else the patient
wants to say
Clarify statements and any jargon used by the patient
Use concise, easily understood language
2. Understand the patient’s perspective
Determine, acknowledge and appropriately explore:
o the patient’s ideas and concerns
o the patient’s expectations
o how each problem affects the patient’s life
Encourage expression of the patient’s feelings
Keynote: New clinical students often feel embarrassed about asking about a patient’s feelings,
expectations or concerns. Ask about these aspects in the same, matter-of-fact way as you ask
about other aspects of the history. If you feel comfortable asking the questions, the patient is
more likely to feel comfortable about answering.
Providing structure to the consultation
1. Know what information you need
have the main headings of the history and lists of any systems-specific questions in
front of you
2. Take notes
take brief notes during the consultation itself
3. Make organisation overt
signpost - explain what the next section addresses
summarise periodically (e.g. after each section)
4. Attend to flow
address topics in a logical sequence (and signpost for the patient)
attend to timing – be clear and honest with the patient about duration of the
consultation

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
7
if the consultation digresses, gently redirect – explain why certain information is
needed
Keynote: Taking notes: say what you are writing as you write it – it reassures the patient that
you have heard and are recording the information correctly, and prevents note-taking from
interrupting the flow of the consultation.
Building the relationship
1. Develop rapport
accept the patient’s views and feelings non-judgementally
use empathy - acknowledge feelings and their predicament
be supportive
deal sensitively with embarrassing or disturbing topics, and pain
2. Involve the patient
share your thinking with the patient
explain the rationale for your questions
during physical examination, explain the process and ask permission
3. Respond to the patient’s needs
e.g. if the patient seems in discomfort, or tired, or in pain, acknowledge this and
respond appropriately - do not simply continue.
4. Use appropriate non-verbal behaviour
eye contact, facial expression, posture, position and movement
vocal cues, e.g. rate, volume, tone
Ending the consultation
The end of a consultation is important for two reasons:
you need to check that the information you have is complete and accurate
the patient needs to know what will happen next
All consultations should have a definite conclusion – note these points down so you can
follow this 5-point plan.
1. When you are satisfied that you have completed the history-taking, tell the patient
that you have covered everything that you need to.
2. Check that the patient has nothing more to add.
3. Summarise the information and check that it is complete and accurate.
4. Explain what will happen next (e.g. you will pass the information on to the doctor,
whether they are going to be seen soon by the doctor etc.)
5. Thank the patient and leave immediately after concluding the interview.
Keynote: If you are asked questions by the patient (e.g. about diagnosis), reiterate that you
are a student and still learning, and that you will pass on the request for information on to the
doctor. Always acknowledge – do not ignore patients’ questions or any requests that you
cannot meet.

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
8
Content of the history
Presenting Complaint
This is the main reason for the patient’s attendance to hospital/GP surgery and should be
recorded in the patient’s own words.
History of Presenting Complaint
This is a list of the main symptoms, either volunteered by the patient or elicited from them
during the consultation.
For each, gather information about:
body location
quality and severity
chronology, including when it first began, mode of onset, mode of ending, duration,
frequency, periodicity
setting (under what circumstances does it take place)
aggravating and alleviating factors, including treatment
associated manifestations
overall course, effect on normal activities
a review of any other symptoms with regard to the body systems under
consideration
any previous history of similar symptoms
It is also important to ask about any relevant risk factors relating to the presenting complaint,
e.g. if taking a history from a patient who has presented with chest pain then ask about
smoking, hypertension, high cholesterol, diabetes, family history of heart disease.
Past medical and surgical history
This is to gather information about the person’s past illnesses and treatment. This will
include information about:
previous hospital admissions
past operations or investigations
major illnesses; rheumatic fever, diabetes, heart disease, jaundice
accidents and injuries
Keynote: Preface questions which mention specific illnesses to the patient with a comment
that you are going to ask a series of routine questions that you ask everyone.
Drug history
This is to establish:
medication the patient is taking (prescribed and over the counter)
medication that the patient is known to be sensitive to
This information is needed because:
medication may be the cause of the presenting problem
current medication may preclude the use of other medications
if a person is admitted to hospital they may need to continue current medication
it provides an opportunity to review the need for taking medications and to find out
whether the person is actually taking them
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
9
the patient may be suffering from side effects
Family history
The family history should include:
causes and age of death of parents
details about the health of siblings and children
details about any health problems or conditions within the family.
Personal and social history
This documents factors in the person’s lifestyle, environment and personal habits which can
put them at risk from illness or have a bearing on established disease. This is an opportunity
to discuss how the person maintains their health (as opposed to discussing illness) and to
consider whether there is a need for primary or secondary prevention. Primary prevention is
the prevention of disease, for example, by health education or immunisation. Secondary
prevention is the prevention of the effects of disease, by early treatment or prevention of
worsening the disease, e.g. by removing the causative agent (e.g. by stopping smoking or
losing weight after the development of angina).
Illness may be related to occupation, to environment, or to being unemployed. Home
responsibilities may preclude admission to hospital. Some social security payments are
stopped during hospital admission. Recent or past travel abroad may have important
implications.
Information to be gathered can include:
general well-being
alcohol, smoking, recreational drug use
HIV risk factors
housing
family relationships and support
Any carers/district nurse/ social worker input
occupation and job security
social or financial problems
It is important to bear in mind that certain aspects of social history can be private and some
patients may find this intrusive. You are reminded to be mindful of this, and to maintain an
open and non-judgemental attitude.
Systems Review
The ‘systems review’ is a traditional comprehensive sweep of all bodily systems, to identify
any symptoms which may otherwise be missed. Symptoms which are important in making
the diagnosis may only come to the surface at the end of a consultation – either because they
have been forgotten or considered trivial by the patient, or even because the patient has been
particularly worried (sometimes known as the ‘by the way, doctor’ or ‘hand-on-the-door’
symptom).

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
10
As a medical student, you do a systems review in order to learn by rote a set of questions for
each bodily system, so that you have these at your disposal when required. However,
running through the entire list for any given patient would exhaust both of you.
Be selective, i.e. focus on the system(s) relating to the patient’s problem list and include others
only if clearly related to the differential diagnosis. Please see the check list below. Remember
to avoid all jargon in your consultation.
Keynote: A well-taken history will usually provide more clues to the diagnosis than the
physical examination. It provides a basis for confidence and trust between the patient and
doctor/medical student.

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
11
Check list for Systems Review
GENERAL
Fatigue/malaise
Fever/rigors/night sweats
Weight/appetite
Skin: rashes/bruising
Sleep disturbance
CARDIOVASCULAR
Chest pain/angina
Shortness of breath (including on exercise)
Orthopnoea
Paroxysmal nocturnal dyspnoea
Palpitations
Ankle swelling
RESPIRATORY
Chest pain
Shortness of breath/wheeze
Cough/sputum/haemoptysis
Exercise tolerance
GASTROINTESTINAL
Appetite/weight loss
Dysphagia
Nausea/vomiting/haematemesis
Indigestion/heart burn
Jaundice
Abdominal pain
Bowels: change/constipation/diarrhoea/
description of stool/blood/mucus/flatus
MUSCULOSKELETAL
Pain/swelling/stiffness – muscles/joints/
back
Restriction of movement or function
Power
Able to wash and dress without difficulty
Able to climb up and down stairs
GENITO-URINARY
Frequency/dysuria/nocturia/polyuria/oliguria
Haematuria
Incontinence/urgency
Prostatic symptoms
Impotence
Menstruation (if appropriate):
menarche (age at onset)
duration of bleeding, periodicity
menorrhagia (blood loss)
dysmenorrhoea, dyspareunia
menopause, post-menopausal bleeding
CENTRAL NERVOUS SYSTEM
Headaches
Fits/faints/loss of consciousness
Dizziness
Vision – acuity, diplopia
Hearing
Weakness
Numbness/tingling
Loss of memory/personality change
Anxiety/depression
ENDOCRINE
Menstrual abnormalities
Hirsutism/alopecia
Abnormal secondary sexual features
Polyuria/polydipsia
Amount of sweating
Quality of hair
SKIN
Rash
Pruritus
Acne
Recommended further reading:
Silverman J, Kurtz S, Draper J (2005) Skills for Communicating with Patients (2nd ed).
Oxford: Radcliffe Publishing. (essential textbook)
http://www.skillscascade.com/handouts/CalgaryCambridgeGuide.pdf

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
12
How to take a Respiratory History
Record the date and time the history was taken.
Name, Age, Occupation(s)
Presenting Problem/Complaint
There are seven main respiratory symptoms to ask about:
1. Cough (character)
2. Sputum (colour, amount)
3. Haemoptysis (colour, amount)
4. Wheeze (diurnal variation?)
5. Chest Pain (site, radiation, character)
6. Shortness of breath (exercise tolerance, orthopnoea)
7. Systematic symptoms e.g. night sweats and weight loss
As for any history, For each symptom describe:
Onset
Duration
Course
Severity
Precipitating Factors
Relieving factors
Associated features
Previous episodes
Past Medical History
e.g. Tuberculosis, atopy, pre-existing respiratory conditions, childhood infections.
Drug History
Allergies, inhalers, nebuliser, home oxygen
Drugs that cause respiratory problems including long term amiodarone, methotrexate,
nitrofurantoin, and chemotherapy agents
Family history
e.g. asthma/hayfever
Social and Occupational History
Smoking history-measured in pack years
Illicit drug use (including cannabis and other inhaled substances eg crack)
Contact with animals/pets (especially birds –don’t forget to ask about hobbies such as pigeon
racing). Presence of stairs in or leading into flat/house. Who does/how is shopping done?
Exposure asbestos, dusts, and other chemicals and organic material (hay, fungi)
Systemic Review and Summarise – does the patient have any questions?

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
13
How to take a Cardiovascular History
Record the date and time the history was taken.
Name, Age, Occupation(s)
Presenting Problem/ Complaint
Remember, this is the main reason for the patient’s attendance to hospital/GP surgery and
should be recorded in the patient’s own words.
History of Presenting Complaint
There are 4 main cardiovascular symptoms:
1. Chest pain (character, radiation)
2. Shortness of breath (exercise tolerance, orthopnoea, paroxysmal nocturnal dyspnoea)
3. Presence and extent of oedema (ankle, leg or sacral)
4. Palpitations (tap out rhythm, any dizziness or blackouts)
Remember the 8 questions you need to ask about each symptom?
During the history consider (and ask about) the main risk factors for Ischaemic Heart Disease:
1. Smoking
2. Hypertension
3. Diabetes mellitus
4. Hyperlipidaemia
5. Family history
Past Medical History
e.g. angina, myocardial infarction, previous coronary bypass operation, valvular disease or
previous heart valve replacement surgery, rheumatic fever, stroke, intermittent claudication
Drug History
Allergies, anti-hypertensive drugs, anti-hyperlipidaemic drugs, anti-arrhythmic drugs etc
Family History
e.g. ischaemic heart disease, myocardial infarction (MI) - remember in particular to ask about
the age of the family member(s) first MI
Social History
Smoking (pack years)
Alcohol
Exercise and diet
Presence of stairs in or leading into flat/house
Systemic Review Summarise – does the patient have any questions?

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
14
How to take a Locomotor History
Main points to enquire about are:
Evolution of condition
Acute or chronic?
Associated events
Response to treatment
Current symptoms
Pain
Stiffness
Swelling
Pattern of joint involvement
Involvement of other organ symptoms
E.g. Skin, lung, eye or kidney symptoms
Any symptom of malaise, weight loss, fevers or night sweats?
Impact of lifestyle
Patient’s needs/ aspirations
Details of any functional impairment
Ability to adapt with functional loss
How to take a Pain History
If the presenting complaint is pain (most types of pain e.g. chest, abdominal etc) the main
points to elicit can easily be remembered using the mnemonic ‘SOCRATES’. All of these
should be documented in the history of presenting complaint.
S -site
O -onset
C -character
R -radiation
A - associations
T -timing
E -exacerbating & relieving factors
S -severity
Remember to ask about analgesic use.

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
15
History Taking Workshop & Presenting
patients
The workshop involves a lecture and demonstration by clinicians so that you can learn about
the content and the process of the medical history and its presentation to colleagues. Taking
what you learnt from the first session and incorporating what you have learnt in
Communications Skills, the second session provides an excellent opportunity to put your
new skills to the test.
The medical “clerking” involves a lot of new terms, abbreviations and diagrams you may not
be familiar with. It can be difficult to know where to best put information that a patient tells
you and how to structure your clerking so that it makes sense. Presenting your history to
experienced doctors can be a very daunting experience at first and you may not know what
information they want from you.
In this workshop, you will have the opportunity to look at complete patient clerkings and see
what doctors actually write down in practice and what it all means. This includes filling in a
drug chart. You will also see presentations of patient histories and have the chance to reflect
on how information is presented and practice presenting in a non-threatening environment.
It is worth preparing for the second session by familiarising yourself with what you have
learnt in the first session and Communication Skills. You don’t have to worry, however,
about knowing lots of clinical conditions. The focus is on how you take the history and
present it. You will learn the meaning of the information you gather over the next few years.
You will realise that at first it is very difficult to remember the content of the history, ask
questions that the patient will understand, listen to the answers and take notes all at the same
time. This session will be a chance to practice this ‘juggling act’ before your join your firms
for history taking.
Learning objectives:
By the end of the sessions students should:
Recall the components of the medical history
Understand the ways in which doctors present medical information
Have seen how to complete a simple drug chart
Be able to explain the features of a good presentation
Have practiced presenting medical information to a colleague

Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
16
General Tips on How to Perform an
Examination
To begin the Examination- WIPER
Wash your hands.
Introduce yourself to the patient (name and status)
Find out the name they like to be called.
Permission: Explain what you would like to do and obtain consent for the
examination.
Expose the relevant part of the patient ensuring as much privacy as possible.
Re-position the patient appropriately (45 degrees for cardiovascular and respiratory,
flat for abdominal)
Before starting the examination, perform a general inspection of the patient from the end of
the bed. Do they look well or unwell? Do they look comfortable/breathless/in any pain?
Don’t forget to also look at the surroundings, e.g. for sputum pots, walking sticks,
medications at the bedside, oxygen, sick bowls etc.
During the Examination
Have a methodical approach to examination. Although each system is slightly different the
standard order is:
INSPECT
PALPATE
PERCUSS
AUSCULTATE
You should avoid causing pain to the patient. You can achieve this by asking the patient if
they have any pain, and by palpating gently to start with. Remember to look at the patient’s
face when you are feeling for tenderness.
To end the Examination
1) Consider whether you need to examine any system in more depth (e.g. a full examination of
joints in a patient with rheumatoid arthritis).
2) Re-examine any aspect that you are unsure about.
3) Inform patient that you have completed your examination. Thank them and help them get
dressed.
4)Wash your hands
After the consultation has finished and you have left the patient:
a) Write a two line summary of what you found in the history and examination
b) Offer a differential diagnosis list for the presenting complaint
c) Make a problem list which will include the present complaint, other illnesses and other
personal, psychological or social factors which affect this illness.
d) Consider what tests (biochemical and radiological) are required to confirm or establish the
diagnosis.
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
17
e) Consider what treatment should be given to the patient.
f) Consider what/if arrangements are needed to hand over the patient’s care to another team.
f) Reflect how the consultation was performed including points to consider for future
consultations

18
Dress and Behaviour Expected in
Clinical Area
In order to gain and maintain the trust and confidence of patients, there are certain rules of behaviour
that a doctor or medical student must observe. Obviously you must never appear in front of a patient
(or indeed in any other teaching situation in College) the worse for drink or drugs, or even smelling of
drink. Remember that abuse of drugs implies that you are not to be trusted with drugs and medicines,
and a conviction for a drugs-related offence may mean that we cannot certify you as fit to practice.
You should regard the clinical aspects of the course as an apprenticeship for your professional career as
a doctor. Certain standards of appearance are necessary, both in your own interests and, most
importantly, for the well-being of patients. Please remember that patients come from all sections of
society and that people who are ill or worried may more easily become anxious about small details.
Many of them will regard you in the same way they will a fully-trained doctor. If your standards of
dress and behaviour are professional and reasonably conservative you will be unlikely to cause offence
or anxiety to your patients, and you will find that your relationships with them and with hospital staff
will be easier.
Students should be smartly dressed in an appropriate and professional manner and in compliance with
NHS infection control policies whilst on hospitals wards, at GP surgeries, at clinical skills sessions
with patients or simulated patients and at OSCEs.
bare below the elbow (short sleeves or sleeves neatly folded) where required by local policy -
most Trusts but not all GP surgeries
no white coats
no denim, no low cut tops, no bare midriffs
no trainers, no stilettos
no wrist watches, bracelets or charity wrist bands
no jewellery except:
rings – one single metal band, no stones
earrings – small studs only
necklaces – a simple chain if tucked inside clothing
no piercings (other than earrings)
face visible
religious head coverings permitted
ties secured inside shirts unless asked by an individual consultant to remove them
hair kept neat and tidy, long hair tied back, modest hair colouring/highlights only
fingernails short and clean, no false nails
identification visible at all times - except during OSCE examinations when badges showing
candidate numbers will be issued
Please note that local Trust policies take precedence, in particular regarding white coats and ties.
If this code is not adhered to by students they may be asked to leave that
clinical session and asked to see the Faculty Tutor.

19
Cardiovascular Examination
(see Clinical Examination, Epstein et al, page 149)
Introduction
W - Wash your hands.
I - Introduce yourself to the patient.
P - Permission. Explain that you wish to examine their heart. Obtain consent for the
examination.
Pain. Ask the patient if they are in any pain and to tell you if they experience any
during the examination.
E - Expose the necessary parts of the patient. Ideally the patient should be undressed
from the waist up taking care to ensure the patient is not cold or unnecessarily
embarrassed.
R - Reposition the patient. In this examination the patient should be supine and reclined
at 45 degrees.
In the cardiovascular examination a lot of information can be obtained by looking for
peripheral signs of cardiovascular disease. The examination is therefore split into a
peripheral examination and then examination of the precordium.
Peripheral Examination
End of the Bed
Look at the patient at the end of the bed for signs of breathlessness or distress.
It is also important to look at the surrounding environment for oxygen, fluid
restriction signs or GTN spray.
Hands
Take the patient’s hand and assess warmth, sweating and whether there is
peripheral cyanosis.
Check the capillary refill (press the end of the finger for 5 seconds, release and see
how long it takes the colour to return. It should be less than 2 seconds)
Examine the nails for clubbing or signs of infective endocarditis (splinter
haemorrhages, Osler’s nodes and Janeway lesions).
Palpate the radial pulse and assess the rate and rhythm.
Locate and palpate the brachial pulse and assess its character.
Measure the blood pressure. If the blood pressure is raised compare both arms
Face
Check eyes for corneal arcus and per-orbital region for xanthelasma.
Inspect the conjunctiva for pallor (which can be a sign of anaemia)
Look at the lips and tongue for central cyanosis. (please note that you do not have
to check under the tongue)
Assess the jugular venous pressure height and wave form. The height of the JVP is
the vertical height above the sternal angle (see figure 1)
Palpate the carotid pulse and assess its character.

20
Tips for assessing the JVP:
This is an area that many students struggle with. Firstly, it is important to remember
the anatomy : the internal jugular vein tracks from beneath the mastoid process down
to between the sternal and clavicular heads of the sternocleidomastoid, always deep to
the sternocleidomastoid, so if the patient’s neck is not relaxed, you will struggle to see
the JVP. Another consequence of the internal jugular vein lying deep, is that you will
never see a clear outline of the JVP, only a diffuse pulsation. Remember that the
external jugular vein is more superficial and can be easily visualised, but this should
not be routinely used to assess the JVP as it is prone to kinking which may give
misleading results.
To examine the JVP, the patient must be lying at 45° and in good light. Ensure that the
patient’s neck muscles are relaxed (you may want to have the patient’s head turned
slightly to the left).
The height of the JVP is directly related to the right atrial pressure, since there are no
valves between the atrium and the internal jugular vein. It is measured as the vertical
height above the sternal angle with the patient lying at 45°. A normal patient’s right
atrial pressure should be less than 9cmH2O, which corresponds to less than a 4cm
vertical distance above the sterna angle (since at 45° the right atrium is approximately
5cm below). Note that it is therefore often very difficult to see in normal patients. To
practise, you may want to experiment with the bed flatter than 45°, since this will
make the JVP more easily visible (remember though that you are then unable to quote
the height of it as you have changed the angle).

21
Differentiating the carotid pulse from the JVP
The JVP :
has a double waveform
is impalpable
varies with position of the patient
height of pulstaion varies with respiration
rises with increased abdominal pressure
Examination of the precordium
Inspection
Inspect the chest wall for
Previous scars
Pacemaker
Abnormal pulsations
A visible apex beat
Palpation
Palpate for:
Apex beat, note the location and assess the quality of impulse felt. Is it forceful,
diffuse, tapping?
Heaves. Heaves are forceful ventricular contractions. Heaves represent ventricular
hypertrophy and feel as if your hand is being lifted of patient’s chest. This should be
performed close to the left sternal border and towards the apex.
Thrills. Thrills are ‘palpable murmurs’ that can be present over any area of heart.
They feel like ‘stroking a purring cat’. If present there should be an easily audible
murmur present on auscultation.
Percussion
This is not normally performed in this examination.
22
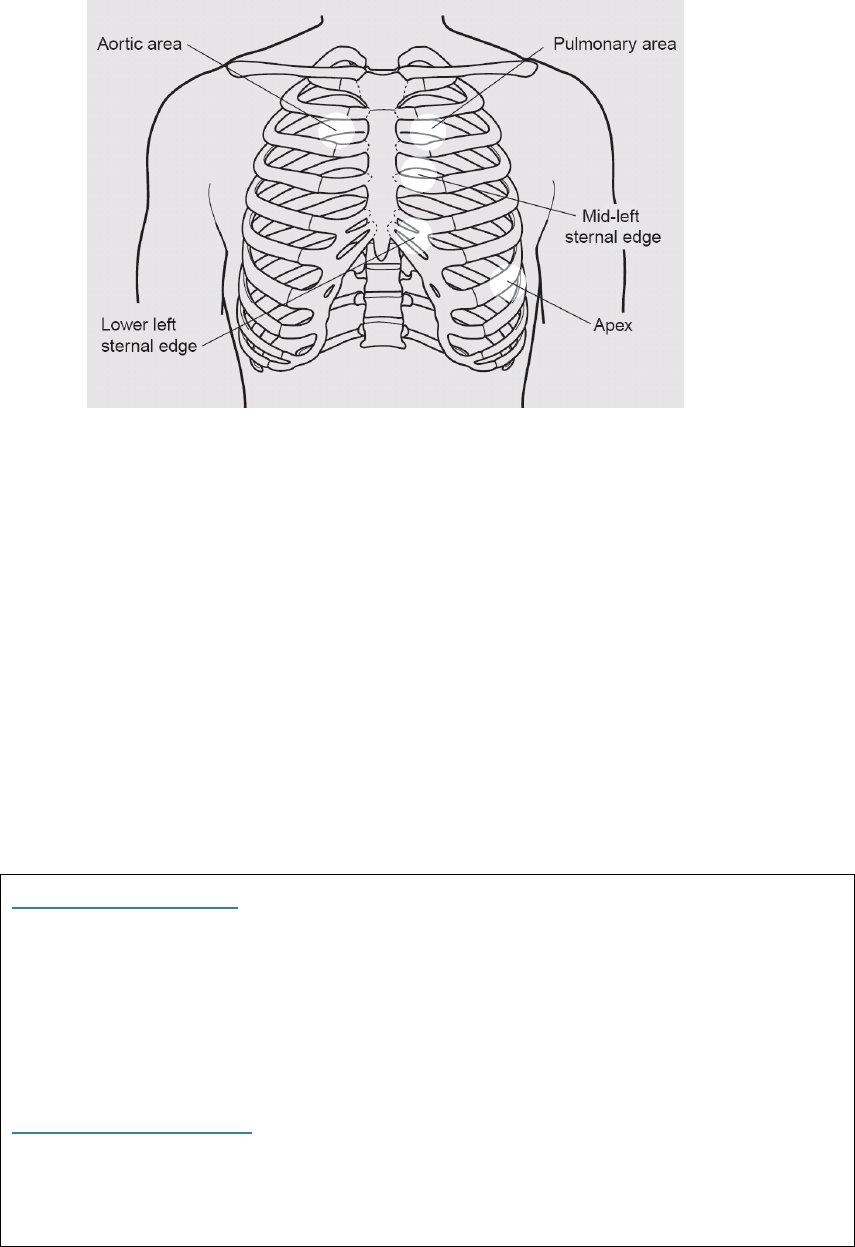
Auscultation
Listen with diaphragm and the bell of your stethoscope at the apex, base, aortic and
pulmonary regions. (see Figure 2 below)
Figure 2: Auscultation areas
Start by listening to the heart sounds. To help you differentiate between the heart
sounds they should be timed against the carotid pulse.
The first heart sound is principally the sound of the mitral valve closing. It is the
sound immediately before the main apical impulse and carotid pulsation. It is usually
loudest at the apex or between the apex and the lower left sternal border.
The second heart sound is due to closure of the aortic and pulmonary valves. It is
the sound which follows the apical impulse and carotid pulsation. It is usually best
heard at the upper left sternal edge using the diaphragm of the stethoscope.
If you hear any murmurs these should also be timed with the carotid pulse to
determine whether they are systolic (with carotid pulse) or diastolic. Also listen to
whether the murmur is louder in inspiration or expiration.
Ask your patient to hold their breath and auscultate over the carotid arteries for
bruits.
Systolic murmurs
Aortic stenosis is an ejection systolic murmur best heard at the apex and upper right
sternal edge. It often radiates to neck.
Mitral regurgitation is a pansystolic murmur best heard at the apex. It radiates to the
axilla.
Diastolic murmurs
These are often more difficult to hear and require the patient to be moved into the best
position to hear them.

23
Mitral Stenosis is best heard with the patient rolled on to their left side using the bell of
the stethoscope to auscultate at the apex. The murmur is low pitched and rumbling and often
localised.
Aortic Regurgitation is best heard with the patient sitting up, leaning forward and
breathing out. (NB left sided murmurs are quieter on inspiration and louder on expiration).It
is heard at the left sternal edge using the diaphragm.
You can hear examples of normal heart sounds and murmurs at ‘Auscultation Assistant:’
http://www.wilkes.med.ucla.edu/intro.html
Finishing Off
State that you would complete the examination by:
Auscultating the lung bases posteriorly for pulmonary oedema
Checking for sacral and ankle oedema
Checking the peripheral pulses – femoral, popliteal, posterior tibial & dorsalis pedis.
Check for an abdominal aortic aneurysm
Finally explain to the patient that your examination has
been completed, thank them for their cooperation and help
them to get dressed.

24
Respiratory Examination
(see Clinical Examination, Epstein et al, page 130).
Introduction
W - Wash your hands.
I - Introduce yourself to the patient.
P - Permission. Explain that you wish to perform a respiratory examination and obtain
consent for the examination.
Pain. Ask the patient if they are in any pain and to tell you if they experience any
during the examination.
E - Expose the necessary parts of the patient. Ideally the patient should be undressed
from the waist up taking care to ensure the patient is not cold or unnecessarily
embarrassed.
R - Reposition the patient. In this examination the patient should be supine and reclined
at 45 degrees.
Peripheral Examination
End of the Bed
First look at the patient from the end of the bed for signs of breathlessness or distress.
It is also important to look at the surrounding environment for sputum pots,
nebulisers, peak-flow meters, inhalers or oxygen tubing.
Hands
Look at the hands for clubbing (note this is best checked by looking at finger from the
side), tar staining and peripheral cyanosis.
Examine for tremor and a carbon dioxide retention flap.
Palpate the radial pulse to calculate heart rate. At this time also assess respiratory rate
and determine the pattern of breathing.
Locate and palpate the brachial pulse and assess its volume and character, feeling for
a bounding pulse (which can be a sign of carbon dioxide retention)
Face
Look at the patient’s eyes and face for signs of Horner’s syndrome.
Inspect the conjunctiva for signs of anaemia.
Look at the lips and tongue for central cyanosis
Lie the patient at 45 degrees and assess JVP.
Palpate the cervical, supraclavicular and axillary lymph nodes.
Examination of the chest
Inspection
Look at the chest wall for:
Chest wall deformity (e.g. barrel chest, pectus excavatum/carinatum, scoliosis or
kyphosis)
Previous scars
Use of accessory muscles
Asymmetry of chest wall expansion (ask patient to take deep breath)
Next note the pattern of breathing; is it regular, what is the rate?
Palpation

25
Palpate the trachea by placing a finger either side of the trachea and judging whether
the distance between it and the sternomastoid tendons are equal on both sides. Before
doing this warn the patient that this might be slightly uncomfortable.
Assess chest expansion by putting the fingers of both your hands as far round the
chest as possible and then bring your thumbs together in the midline but not
touching the chest wall. Ask your patient to take a deep breath and observe whether
the distance moved is the same for both thumbs.
Palpate for tactile vocal fremitus by placing the edge or flat of your hand on the chest
and asking your patient to say ‘ninety nine’. This should be performed in a
systematic fashion, comparing each side and covering all areas of the front and back
of the thorax (including the axilla).
Percussion
Start percussion by tapping directly in the middle of both clavicles. Then work down
the chest in a systematic manner comparing each side and including the axillary
region. The finger on the chest should always be placed in the intercostal space, and
there is no need to percuss more heavily than is necessary as this can be distressing
for the patient.
Auscultation
Auscultation is then performed in a similar manner using the diaphragm of your
stethoscope.
Ask the patient to take deep breaths through their mouth and commencing at the
apices work down the chest in a stepwise manner, comparing each side with the
other and remembering to include the axillary region.
Listen for breath sounds - are they vesicular (normal)? Next are there any added
sounds (wheeze, crackles, or rubs)?
Assess vocal resonance: use the same auscultation technique but ask patient to say
‘ninety nine’. If appropriate (normally if consolidation is suspected) test for
whispering pectoriloquy by asking patient to whisper (if consolidation present the
sound will still be heard clearly).
The patient is then asked to lean forward and the examination is then performed on the
posterior aspect of the patient’s chest.
Finishing Off
State that you would complete the examination by:
Checking for ankle oedema (cor pulmonale)
Measuring the peak flow rate
Measuring the oxygen saturation
Examining the contents of the sputum pot
Finally explain to the patient that you have finished
your examination, thank them for their cooperation and
help them to get dressed.
Online resources:
Examples of recordings of breath sound are available at:
http://www.med.ucla.edu/wilkes/lungintro.htm
http://www.rale.ca/Recordings.htm
Guidelines on how to perform a peak flow measurement:
http://www.netdoctor.co.uk/diseases/facts/asthmapeakflowmeter.htm
26
Abdominal Examination
(see Clinical Examination, Epstein et al, page 214)
Introduction
W - Wash your hands.
I - Introduce yourself to the patient
P - Permission. Explain that you wish to perform an abdominal examination and obtain
consent for the examination. Pain. Ask the patient if they are in any pain and to tell
you if they experience any during the examination.
E - Expose the necessary parts of the patient. Ideally patients should be exposed from
xiphisternum to pubis (classically they should be exposed from “nipples to knees”,
but this is rarely done in practice to preserve patient dignity). Ensure adequate
privacy.
R - Reposition the patient. In this examination the patient should be lying flat with one
pillow under the head. This is not possible with all patients so first check if they are
comfortable in this position.
During the examination of the abdominal system a lot of information can be obtained by
looking for peripheral signs of gastrointestinal disease. The examination is therefore split into
a peripheral examination and then an examination of the abdomen.
Peripheral Examination
End of the Bed
Look at the patient from the end of the bed for obvious jaundice, nutritional status,
signs of pain or distress, signs of easy bruising or weight loss.
Are there any abdominal drains, stoma bags or signs of an AV (arteriovenous)
fistula?
It is also important to look at the surrounding environment for sick bowls, food
supplements, special dietary notices and ‘nil by mouth’ instructions etc.
Hands
Examine the hands for palmar erythema, Dupuytren’s contracture, koilonychia and
leukonychia.
If appropriate (patient jaundiced or confused) examine for liver flap.
Face
Look at sclera to assess whether jaundiced and inspect the conjunctiva for signs of
anaemia. Also look for xanthelasma (chronic cholestasis), corneal arcus
(hyperlipidaemia), parotid swelling (alcohol abuse) and bruising.
Look at the mouth to assess dentition, angular cheilitis (iron deficiency) and any
presence of aphthous ulcers (Crohn’s).
Look at the tongue for any glossitis. A red and beefy tongue can indicate folate/B12
deficiency. atrophic and smooth can indicate iron deficiency

27
Look for signs of dehydration in the face and mouth (e.g. sunken eyes, dry mucous
membranes)
Chest
Examining chest for spider naevi (>5 is abnormal) and gynaecomastia.
Note distribution of body hair, particularly paucity of hair (liver disease).
Examination of the abdomen
Inspection
First inspect abdomen from the end of the bed before closer inspection at bedside.
Initially look for general signs such as weight loss. Then check specifically for:
Asymmetry
Abdominal distension (remember the 5Fs – flatus, faeces, foetus, fat, fluid)
Scars and striae
Prominent veins
Hernia
Visible peristalsis (this is normally only seen in chronic pyloric stenosis or intestinal
obstruction)
Palpation
Position yourself by kneeling or sitting on the patient’s right hand side. Ensure your
hands are warm. Ask patient if they have any pain or tenderness.
Begin with light palpation of the nine segments. If patient has complained of pain
begin at opposite side. Observe patient’s face throughout palpation to ensure that you
are not causing pain.
Light palpation is used to assess tenderness and guarding (a sign of irritation of the
peritoneum).
Proceed next to deep palpation of the same nine segments. Deep palpation is used to
assess for masses.
If appropriate, test for rebound tenderness (a sign of peritonitis)
Figure 3 Nine segments of the abdomen. Taken from Wikipedia
28
Palpation of organs
Liver
A normal liver extends from 5
th
intercostal space to costal margin. It may be palpable in
normal individuals. Position your hand in the right iliac fossa with fingers in an upward
position facing the liver edge (alternatively you can use the radial aspect of your index
finger). Press your fingertips inward and upward and hold this position while your patient
takes a deep breath. As the liver moves downward with inspiration the liver edge will be felt
under fingertips. If no edge is felt repeat the procedure closer and closer to the costal margin
until either the liver is felt or the rib is reached.
Spleen
The normal spleen cannot be felt and only becomes palpable when it has doubled in size. It
enlarges from under the left costal margin towards the right iliac fossa.
Position the palmer aspect of your left hand around the back and side of the lower rib cage.
The fingertips of right hand are then positioned obliquely across the abdomen pointing to the
left costal margin towards the axilla (again, you may use the radial aspect of your index
finger). Press your fingertips inward and upward and hold this position while your patient
takes a deep breath. As the spleen moves with inspiration the edge may be felt under your
fingertips. If no edge is felt repeat the procedure closer and closer to the left lower rib cage
until the costal margin is reached.
If the spleen is not palpable, this procedure can then be repeated with the patient rolled onto
right lateral position with knees drawn up to relax abdominal position. Palpate with your
right hand while using your left hand to press forward on the patient’s left lower ribs from
behind. It could be argued that this method should be used first, since very few patients have
spleens which have enlarged to occupy the right iliac fossa.
Kidneys
The kidneys are retroperitoneal, so not usually palpable except in some thin individuals.
To examine left kidney, place the palmar aspect of left hand posteriorly under left flank.
Position the middle three fingers of right hand below the left costal margin, lateral to the
rectus muscle (opposite position of left hand). Ask patient to take deep breath and press both
fingers firmly together. If the kidney is palpable it will be felt slipping between both fingers.
To examine the right kidney repeat the procedure with your left hand tucked behind the right
loin and your right hand below the costal margin, lateral to the rectus muscle.
Aorta
In thin patients’ or those with a dilated aorta, the aorta can be palpated by placing both hands
on either side of the midline at a point half way between the xiphisternum and the umbilicus.
Press your fingers posteriorly and slightly medially and the pulsation should be present
against your fingertips.
Percussion
Liver
Begin by establishing lower liver edge. Place hands parallel to the right costal margin starting
at the same point as you began palpation. Repeat in a stepwise manner moving the fingers

29
closer to the costal margin until the note becomes duller. This is the position of the lower liver
edge. Next find the upper margin of the liver. It can be located by detecting a change in note
from the dullness of liver to resonance of lungs.
Spleen
Begin by percussing the ninth intercostal space anterior to the anterior axillary line (Traub’s
space). If the spleen is not enlarged the sound will be tympanic. If it is dull continue to
percuss in a stepwise manner moving hands towards right iliac fossa.
Ascites
If ascites is suspected percuss across patients abdomen (from midline to left flank) until the
percussion note changes from tympanic to dull. Mark that spot and then ask your patient to
turn onto their right side (if you are standing on right of patient). After 30 seconds repeat
percussing from the right flank towards the midline. If fluid is present it will have
redistributed secondary to gravity and therefore the area previously marked as sounding dull
to percussion will now be tympanic.
Bladder
If the bladder is distended the suprapubic area will be dull rather than tympanic. Percuss
from the level of the umbilicus, parallel to the pubic bone.
Auscultation
Bowel sounds
Place the diaphragm of your stethoscope on the midabdomen and listen for gurgling sounds.
These normally occur every 5-10seconds however you listen for 30 seconds before concluding
that they are absent. Absent bowel sounds indicates intestinal ileus. Increased bowel sounds
indicate bowel obstruction.
Arterial bruits
Place diaphragm of stethoscope over aorta and apply moderate pressure. If a systolic
murmur is heard this indicates turbulent flow caused by atherosclerosis or an aneurysm.
Listen for renal bruits 2.5cm above and lateral to the umbilicus. Then listen over liver and
spleen.
Finishing off
State that you would complete the examination by:
Checking for any lympahdenopathy
Examining the hernial orifices
Examining the external genitalia
Performing a digital examination of the anus and rectum
Performing a urinary ‘dipstick’ analysis
Finally explain to patient that your examination has been
completed, thank them for their cooperation and help them
to get dressed

30
Musculoskeletal Examination- GALS
Screen
The GALS screen is a quick screening examination to pick up problems in the musculoskeletal
system. You are checking for changes in appearance (swelling, deformity, abnormal posture) and
movement (restricted, pain).
W - Wash your hands.
I - Introduce yourself to the patient.
P - Permission. Explain that you wish to examine their arms, legs and spine. Obtain
consent for the examination.
E - Expose the necessary parts of the patient. Ideally the patient should be dressed only
in their underwear.
R - Reposition the patient. In this examination the patient should be supine and the bed
flat. This is not possible with all patients so first check if they are comfortable in this
position.
Begin by asking 3 screening questions.
Have you any pain or stiffness in your muscles, joints or back?
Can you dress yourself completely without any difficulty?
Can you walk up and down stairs without any difficulty?
Next examine the patient as documented below. Remember to get the patient to copy you
and compare one side with the other.
Gait
Ask the patient to walk a few steps, turn and walk back. Observe gait for symmetry, smoothness
and ability to turn quickly.
With the patient standing, inspect from behind, from side and in front. Look for bulk and
symmetry of shoulder, gluteal, quadriceps and calf muscles; limb alignment, alignment of spine;
level iliac crests; ability to fully extend elbows and knees; popliteal swelling; abnormalities of
feet.
Arms
Ask patient to put their hands behind their head. Assess shoulder abduction and
external rotation and elbow flexion.
With patient’s hands held out, palms down, fingers outstretched, observe the back of
the hands for joint swelling and deformity.
Ask patient to turn their hands over. Look for muscle bulk and deformities.
Ask patient to make a fist. Visually assess power grip, hand and wrist function and
range of movement in fingers.
Ask patient to squeeze your fingers to assess grip strength.
Ask patient to bring each finger in turn to meet the thumb. Assess fine precision
pinch.

31
Gently squeeze the metacarpophalangeal (MCP) joints for tenderness (ask about pain
first).
Legs
While standing inspect from the front, side and behind paying special attention to the
popliteal fossa.
Lie patient on couch. Assess full flexion and extension of both knees, feeling for
crepitus.
With hip flexed to 90 degrees, holding the knee and ankle, assess internal rotation of
each hip in flexion.
Perform a patellar tap.
Squeeze across metatarsophalangeal (MTP) joints (ask about pain first).
From end of bed inspect feet for swelling deformity and callosities.
Spine
From behind inspect the spine for scoliosis
From the side inspect spine for lordosis and kyphosis
Ask patient to touch their toes. Assess lumbar spine flexion by placing two fingers on
the lumbar vertebrae. Your fingers should move apart on flexion.
Inspect lateral cervical flexion by asking the patient to put ‘their ear to their shoulder’
on each side.
Finally explain to patient that your examination has been
completed, thank them for their cooperation and help them
to get dressed.
32
Motor Examination of Lower Limbs
(see Clinical Examination, Epstein et al, page 355)
Introduction
W - Wash your hands.
I - Introduce yourself to the patient
P - Permission. Explain that you wish to perform an examination of their legs and obtain
consent for the examination. Pain. Ask the patient if they are in any pain and to tell
you if they experience any during the examination.
E - Expose the necessary parts of the patient. Ideally the patient should be undressed
from the waist down (excluding underwear) taking care to ensure the patient is not
cold or unnecessarily embarrassed.
R - Reposition the patient. In this examination the patient should be supine.
Inspection
End of the bed
Is the patient comfortable or uncomfortable
It is also important to look at the surrounding environment for walking sticks or a
wheelchair.
Inspect for:
Symmetry of muscle bulk.
Muscle wasting
Hypertrophy
Spontaneous muscle contractions (fasciculations).
Any skin changes (especially vasculitic skin changes)
Tone
Ask the patient to relax their legs.
Place your hands on the thighs and gently roll each leg while observing the
movement of the corresponding foot. If normal tone the foot will move. In markedly
raised tone both legs move when one is rolled.
Place your hands under the thigh and try to lift up leg briskly. In normal tone the foot
of the leg lifted stays on bed.
All movements should be carried out both quickly and slowly, so as to tell the
difference between a spastic increase in tone (velocity dependent, a sign of pyramidal
pathology) compared to a rigid increase in tone (velocity independent, a sign of
extra-pyramidal pathology)
If the tone is increased then, with the knee bent, quickly dorsiflex foot to test for
clonus.
Power
Test each muscle group in turn, comparing the same muscle group in the other limb. Test
against gravity before applying a force. Make sure you are testing power across only one
joint at a time- ideally put one hand above the joint being tested and test with the hand below
the joint.
Lift your leg up: don’t let me push it down (L1, 2)

33
Now push me down with the whole leg (to look specifically for a pyramidal
distribution of weakness (where hip flexion is much weaker than hip extension) vs a
proximal weakness (both weak)
Bend your knee: don’t let me straighten it (L5, S1)
(Knee still bent) Kick me away (L3, 4)
Bend your foot down: push my hand away (S1)
Cock up your foot, point your toes to the ceiling: stop me pushing your foot down
(L4, L5)
Now just push your big toe up to your face (L5)
[IF weakness of ankle dorsiflexion also test ankle eversion (L5 and common peroneal
nerve) and Inversion (L5 and post tibial)
Record as MRC grade 0-5
As with the upper limb ideally you would get a PATTERN of weakness-eg proximal
(shoulders and hips weak hands and feet strong usually MYOPATHY), distal (fingers and
toes/ankles weak usually NEUROPATHY) or PYRAMIDAL (especially weak shoulder
Abductors, Elbow Extensors, Finger ABdutors, Hip Flexors, Knee Flexors and Ankle
Dorsiflexors) or GLOBAL which could mean anything ie no pattern.
Reflexes
Knee (L3, L4)
Insert your left arm under the patient’s knees and flex them slightly. THEY MUST RELAX!
Tap first the right patella tendon and then the left-COMPARE SIDES. If present, the reflex
will be observable at the quadriceps muscle.
Ankle (S1))
Abduct and externally rotate the patient’s leg at the hip then flex the knee. Passively dorsiflex
the ankle by placing your hand on the ball of the patient’s foot, then tap over the Achilles
tendon. If present, you will see the reflex in the calf muscles and you may feel it in your
hand.
Many students struggle with reflexes. If you are having trouble eliciting reflexes, make sure
that the patient’s muscles are relaxed and the tendon is stretched. Most importantly,
remember that one single, confident strike is far better than numerous tentative ones! You
may also want to try reinforcement if the reflex cannot be elicited; ask the patient to interlock
fingers and pull one hand against the other on your command immediately before you strike
the tendon.
0
No movement
1
Flicker of movement
2
Movement with gravity eliminated
3
Movement against gravity
4
Movement against resistance but incomplete
5
Normal power for age & sex
34
Grading reflexes
0
Absent
+/-
Present with reinforcement
+
Just present
++
Brisk normal
+++
Exaggerated response
Plantar
Using an orange wood stick (you will rarely find these on a non-neurology ward. If this is the
case, any blunt implement will work, such as a thumb nail), stroke the lateral aspect of the
sole of the foot, starting from the heel to the base of the toes. In a normal person the first
movement of the big toe is plantar flexion.
Sensation
IF PERFORMING A FULL NEUROLOGICAL EXAMINATION, THE SENSORY PART
WOULD COME IN HERE
Coordination
Ask patient to slide the heel of one foot in a straight line down the shin of the other leg. When
the heel has reached the bottom of the shin, ask the patient to flex the leg then bring the heel
back down on to the shin just below the knee.
In a person who does not have any problems with co-ordination these steps are completed in
smooth manner- The key is movement through free air. Do not let them cheat by dragging
the heel back up the shin.
Gait
In the real world patients are often frail and unsteady and letting them fall is something to be
avoided. Therefore assume they can hardly stand and work from there:
1) Ask the patient whether they can stand with both feet close together
2) If yes, then put a hand behind & in front to prevent the patient from falling. Instruct
them to close their eyes (Romberg’s test) [note that this is really a sensory test. It is
mentioned here as in practice motor and sensory systems are usually tested at the
same time and this a convenient time to do it]
3) If the patient is still okay, ask them to stand on tip-toes (with your hands lightly
supporting their shoulders) for a true test of ankle plantar flexion power.
4) Then ask the patient to stand back on their heels and lift their toes to test for foot
drop
5) Ask the patient to walk to a defined point and back looking for any abnormal gait
and the evidence of arm swing. In addition to this, ask the patient to walk heel to toe
(demonstrates ataxia)
Finally explain to patient that you have finished your
examination, thank them for their cooperation and help
them to get dressed.

35
Examination of the Upper Limbs
(see Clinical Examination, Epstein et al, page 355)
Introduction
W - Wash your hands.
I - Introduce yourself to the patient
P - Permission. Explain that you wish to perform an examination of their arms and
obtain consent for the examination. Pain. Ask the patient if they are in any pain and
to tell you if they experience any during the examination.
E - Expose the necessary parts of the patient. Ideally the patient should be exposed from
the waist upwards taking care to ensure the patient is not cold or unnecessarily
embarrassed.
R - Repostition the patient. In this examination the patient should be in the sitting
position.
Inspection
End of the bed
Is the patient comfortable or uncomfortable
It is also important to look at the surrounding environment for clues to the patient’s
condition.
Inspect for:
Symmetry of muscle bulk.
Muscle wasting (have a pointed look over the thenar (median nerve), hypothenar
(ulnar nerve) and area between (carpal tunnel release scar) as well as for wasting of
the first dorsal interossei(fleshy part between thumb and finger on the dorsum of the
hand- ulnar nerve)
Observe muscle for spontaneous contractions (fasciculations).
Skin changes
Pronator Drift test: Ask the patient to stretch out their arms (palms UP) and close
their eyes. Look for any drifting down of the arms, especially unequal drifts-suggests
pyramidal lesion in brain such as stroke-a good screening test to do at the start of an
exam.
Tone
Hold the patient’s hand as if shaking hands, using your other hand to support the
patient’s elbow.
o First, check for a velocity-dependent increase in tone (clasp-knife) by briskly
pronating/supinating the forearm
o Second, check for generalised increase in rigidity by slowly flexing/extending
at the elbows; and by rotating the wrist. You may notice a tremor on top of
the increase in tone, in which case it is called ‘cogwheel-rigidity’.

36
Power
Test each muscle group in turn, comparing the same muscle group in the other limb. Test
against gravity before applying a force. Make sure you are testing power across only one
joint at a time- ideally put one hand above the joint being tested and test with the hand below
the joint.
Shoulder abduction (C5)
(Shoulder adduction is generally not performed due to multiple muscles/nerve roots
involved)
Elbow flexion (C5, 6) and extension (C6, 7, 8)
Wrist extension (C7)
Finger extension (C7, radial nerve)
Finger abduction (T1, ulnar nerve)
Thumb abduction (with your palms up to ceiling point your thumbs up to your nose)
(T1, median nerve)
Record as MRC grade 0-5
Reflexes
Biceps (C5, C6)
Ask the patient to flex their elbow to 90° and rest their forearm on their abdomen. Locate the
biceps tendon and rest your finger on it. Strike your finger and watch the biceps muscle for
contraction.
Triceps (C7)
Ask patient to resume the position as above. Strike the triceps tendon directly, just above the
olecranon process and watch the triceps muscle for contraction.
Supinator (C5, C6)
Ask the patient to maintain the position described above, making sure their hand is in the
mid prone position. Rest your finger on the lower radius on the extensor aspect of the arm
and strike it with the tendon hammer. Observe the movement in the brachioradialis muscle.
If you are having trouble eliciting these reflexes, you can use reinforcement. For upper limbs
it is carried out by asking the patient to tightly clench their teeth just before the hammer is
used.
If the reflexes are very brisk you could test for Finger Jerks & Hoffmann’s sign
Grading reflexes
0
No movement
1
Flicker of movement
2
Movement with gravity eliminated
3
Movement against gravity
4
Movement against resistance but incomplete
5
Normal power for age & sex
37
0
Absent
+/-
Present with reinforcement
+
Just present
++
Brisk normal
+++
Exaggerated response
Sensory
Same as for the lower limbs but testing the dermatomes in the arms. Remember that
it is easiest to test the dermatomes with the patient’s arms in the anatomical position.
Test for light touch, pain, temperature, proprioception and vibration
Coordination
Finger-nose test: Place your finger so that the patient can reach it with a fully
outstretched arm. Ask the patient to touch your finger with their finger and then
touch their own nose. Move your finger and ask the patient to repeat. An intention
tremor is one that becomes worse the closer the finger is to the target, whereas a
postural tremor is one that stays constant throughout the range of movement.
Rapid alternating movements: Ask the patient to rapidly pronate and supinate their
hand on the dorsum of the other hand. An inability to perform this task is called
dysdiadochokinesis. Make sure they take the hand right off rather than just rolling on
the edge of the hand-. The key is movement through free air, so do not let them cheat!
Finally explain to patient that you have finished your
examination, thank them for their cooperation and help
them to get dressed.

38
Sensory Examination of Lower Limbs
(See Clinical Examination, Epstein et al, page 367)
Introduction
W - Wash your hands.
I - Introduce yourself to the patient
P - Permission. Explain that you wish to perform an examination of their legs and obtain
consent for the examination. Pain. Ask the patient if they are in any pain and to tell
you if they experience any during the examination.
E - Expose the necessary parts of the patient. Ideally the patient should be undressed
from the waist down (excluding underwear) taking care to ensure the patient is not
cold or unnecessarily embarrassed.
R - Repostition the patient. In this examination the patient should be supine.
Principles of examination
There are five modalities of the sensory system; light touch, pain, temperature,
proprioception and vibration. Symptoms of an alteration in sensation include numbness, pins
and needles and pain. Start each examination by asking the patient if they have any areas of
altered sensation- if in an OSCE, ask the examiner if this is okay as this is borderline history
taking.
The stimuli being tested is demonstrated to the patient with their eyes open before being
tested with their eyes closed. Proprioception and vibration are demonstrated on the patient’s
feet; light touch, pain and temperature are demonstrated on the patient’s torso or arm-the
levels are usually NOT the same even for same pathway so don’t be surprised-classically joint
perception may only be affected to digits but vibration much further up limb). Light touch,
pain and temperature are then examined in all the dermatomes. (see fig 4)
Light Touch
Use a wisp of cotton wool or monofilament, if cotton wool is used do not drag it over the skin
but apply it to a single point. Demonstrate the sensation to the patient-use their torso with
their eyes open. Then ask them to close their eyes and to say ‘yes’ when they can feel the
sensation of being touched with whichever object you are using (just feeling “something” is
not necessarily normal- they should be able to identify it). Examine each dermatome in a
systematic manner (this can be done comparing legs or testing each leg separately). If an area
of abnormality is found map out the extent of the problem- is it dermatomal or glove and
stocking distribution?
Pain (DON’T say PAIN to the patient-say PINPRICK SENSATION!!)
This is examined using a neurological pin (Neurotip). Needles or cannulae should not be
used as these can puncture the skin. The examination routine is the same as that used for light
touch and the patient should be able to feel the stimulus as sharp. (It is often done at the same
time getting the patient to differentiate between the stimuli). Pain (and temperature) is
conveyed by the spinothalamic tract.
39
Temperature
This is not generally performed in a routine examination however it can be examined in the
same way as light touch. As both hot and cold are carried on the same fibres it is sufficient to
test one, due to lack of available equipment this is normally cold using the metal of the tuning
fork.
Proprioception
This is examined by testing the joint position sense in the big toe. First isolate the joint by
holding it apart from the other toes. Hold the distal phalanx of the patient’s large toe at the
sides to avoid giving information from pressure. Demonstrate the movements of ‘up’ and
‘down’ to the patient. Ask the patient to close their eyes and to say whether the movement is
up or down. Proprioception can also be assessed by Romberg’s test: ask the patient to stand
with feet together with both eyes open (be in a position in which to catch patient if required-
ie hand behind & in front of the patient). Then ask the patient to close their eyes. If they are
more unsteady with their eyes closed this is a sign of difficulty with proprioception.
Remember that proprioception (and vibrational sense) is conveyed by the dorsal
column/medial lemniscal pathway.
Vibration
Use a 128 Hz tuning fork. Demonstrate the sensation on the sternum. To ensure that you are
testing vibration rather than sensation ask the patient first ‘if they feel buzzing sensation’. If
they answer yes; ask them to tell you when ‘it stops’. Vibration is tested on bony
prominences, initially on the medial aspect of the big toe. If vibration is absent here then the
tuning fork should be moved proximally to establish the level at which it can be appreciated.
Start at a boney part of the toes, the medial or lateral malleolus, then the upper part of the
tibia, then the iliac crests.
Finally explain to patient that you have finished your
examination, thank them for their cooperation and help
them to get dressed.

40
Fig 4. Dermatome distribution
It is important to note that dermatomal distribution differs from person to person (and from
textbook to textbook), so these mappings are not absolute. A useful way to remember
dermatomes is to memorise a few landmarks and the rest falls into place (usually this is
easiest to do with the model in the anatomical position). Some useful landmarks are C5
(shoulder point), T4 (nipples), T10 (umbilicus), L3 (medial side of the knee) and S1 (sole of the
foot).
41
Cranial Nerve Examination
(See Clinical Examination, Epstein et al., page 309)
Introduction
W - Wash your hands.
I - Introduce yourself to the patient
P - Permission. Explain that you wish to perform an examination of the nerves in their
head and obtain consent for the examination. Pain. Ask the patient if they are in any
pain and to tell you if they experience any during the examination.
E - Expose the necessary parts of the patient. The face and neck should be exposed.
R - Reposition the patient. In this examination the patient should be either sitting in
chair or sitting at side of bed. Ensure adequate privacy.
Inspection
Does the patient look well or unwell
Are there any obvious abnormalities of the face e.g. facial weakness, drooping mouth
Are there any obvious abnormalities elsewhere
The Cranial Nerves
I. - Olfactory nerve
Test the sense of smell in each nostril with coffee or some other distinct smell
(Usually it is only asked about:.Have you noticed a recent change in your sense of
smell or taste? (both are intrinsically linked)
II -Optic nerve
Check acuity using Snellen chart and colour vision using Ishihara plates
Perform visual field assessment comparing your visual fields to the patient’s
o It is important to test all four quadrants.
Examine the pupils for pupillary light responses.
o Look for asymmetry; reactivity to direct & indirect light; and to
accommodation
Perform fundoscopy- note the appearance of the optic disc and its margin
III/IV/VI- Oculomotor, Trochlear & Abducens nerves
Near and light reaction (as tested above) – the efferent pathways of the accomodation
reaction pass through the oculomotor nerve.
Inspect the eyelids and the pupils- ?ptosis. If yes think Horners (subtle ptosis only on
downgaze and a small pupil, as well as upside down ptosis); IIIrd nerve palsy (gross
ptosis and eye down and out) or myasthenia (variable ptosis which is worse on
prolonged looking up)
Ask the patient to follow your finger with their eyes and assess eye movements.
During these movements, get them to tell you if they see double at any point.
Hold the finger at the extremes and observe for the presence of nystagmus
42
Remember VI (Lateral rectus) allows the eye to look to the side, IV (superior oblique)
allows the adducted eye to look down at tip of nose and all other movements are due
to III)
V- Trigeminal nerve
Sensory – using cotton wool touch each of the 3 divisions (ophthalmic, maxillary and
mandibular) comparing side to side
Motor – examine muscles of mastication – temporalis and masseter. Ask the patient
to open their mouth against resistance (lateral pterygoids) and note jaw deviation
towards the side of the lesion.
Reflexes- The afferent part of the jaw jerk is formed by the motor root of the
trigeminal nerve. In the corneal reflex the afferent limb is contained in the ophthalmic
division- in an OSCE, offer to do this but you won’t be asked to as it is
uncomfortable. If you have to, touch lightly over the COLOURED part or eye not
black or white!)
VII -Facial
Examine the muscles of facial expression (including buccinator). N.B the upper half
of the face is innervated by both cerebral hemispheres: thus, in upper motor neuron
lesions there is sparing of the frontalis muscle and unilateral, lower facial weakness.
Examine (or ask about) taste- note this is only for anterior 2/3 of tongue.
VIII-Vestibulocochlear
Examine hearing by rubbing fingers together or whispering numbers
Rinne’s test-Place a 256 or a 512Hz fork on the mastoid process and then move it in
front of the pinna. A patient with no hearing problems should hear sounds
transmitted via air conduction louder than those via bone. In a conductive hearing
loss, bone conduction will be louder than through air.
Weber’s test-Place a 256 or a 512Hz tuning fork on top of head and ask which ear the
buzzing is loudest. Normally both are same. If different it should be heard loudest in
the ear affected by conductive deafness and quieter in the ear affected by perceptive
deafness.
IX/X-Glossopharyngeal and Vagus
Isolated lesions of IX are very unusual and are difficult to test for.
If there is suspicion of a problem, offer to test the gag reflex-(this is uncomfortable so
is very rarely performed). To do it, place a round tongue depresser lightly on the soft
palate on each side. IX is the sensory and X is the motor component.
For vagus, assess movement of soft palate and NOT the uvula (it can go anyway it
likes) (ask the patient to say ‘aahh’). The palate will not lift up on the side of the
lesion
43
XI- Accessory
Examine the sternomastoid and upper fibres of the trapezius by asking the patient to
shrug their shoulders and to turn their head against resistance (feel for the strength in
the contralateral sternocleidomastoid).
XII-Hypoglossal
Examine the tongue for wasting and fasciculations (if found and combined with brisk
jaw jerk when testing V suggestive but not diagnostic of Motor Neurone Disease (NB
never use this term in front of patients. Say anterior horn cell disease))
Assess tongue movements and note any deviation. The tongue deviates to the side of
the lesion.
Finally explain to the patient that you have finished and
thank them for their cooperation.
44
Ophthalmology - How to measure visual
acuity
Distance vision
Sit the patient at a standard distance - 6metres (unless using modified chart)
Test each eye separately by covering one of the eyes
Ask patient to read letters on chart. The lowest correct line is their distance visual
acuity.
Unaided visual acuity is measured first (no glasses).
Corrected visual acuity measured next (with glasses).
If no letters seen test ability to count fingers, then hand movements, then perceive
light.
The pin hole test
If the vision falls below 6/6 use the pin hole test to tell if the cause of reduced vision is due to
refractive error. If reading through the pin hole occluder the patient is able to read further
down the chart they have an uncorrected refractive error.
Near vision
This is usually tested using a book of standard test types. (If these are not available most
newspaper text is N8 and headlines N12).
With glasses on if required occlude one eye and ask patient to hold book at
comfortable distance and read smallest text that they can see.
Repeat with other eye.
How to record visual acuity
Distance Visual Acuity is recorded as a fraction
The numerator is the distance from the chart in metres.
The denominator is the number written on the chart
i.e 6 (metres)/ 6 (line reached on chart)
The acuity recorded must reflect how this measure was achieved.
If glasses were worn the number is followed by – C gl
If glasses were not worn (but usually are) the number is followed by- S gl
If contact lenses were worn, the number is followed by – CCL
If acuity is achieved by pinhole, the number is followed by – C PH
Near visual acuity is recorded according to the smallest size text which could be seen e.g. N4
For patients that do not speak English use the Sheridan-Gardiner test. This shows single
letters which the patient can match to letters on a hand held chart.

45
Examination using an Ophthalmoscope
with a patient
Introduction
W - Wash your hands.
I - Introduce yourself to the patient
P - Permission. Explain that you wish to perform an examination of their eyes and
obtain consent for the examination. Warn the patient beforehand that you will need
to stand quite close to their face to be able to look into the back of their eyes and
check that they are comfortable with this.
Pain. Ask the patient if they are in any pain and to tell you if they experience any
during the examination.
E - Expose the necessary parts of the patient. The face and neck should be exposed.
R - Reposition the patient. In this examination the patient should be sitting in a chair
Inspection
Is the patient wearing glasses/contact lenses?
Are there any signs of eye disease, e.g. cataracts, pupillary abnormalities, conjunctival
injection etc?
Fundoscopy
Setting up the ophthalmoscope
Ideally the room should be dimly lit
Switch on the ophthalmoscope.
Shine the light on your hand and select a large aperture.
Rotate the focusing wheel and set it on zero.
Keep your index finger on the focusing wheel.
Ask the patient to remove their glasses [not contact lenses].
It is optional to take off your own glasses.
Ask the patient to look at a distant object straight ahead.
Warn the patient that you will shine a light into their eye.
Red reflex
Look through the ophthalmoscope and illuminate the pupils one at a time. The pupil should
appear red- this is called the red reflex. Absence of the red reflex can indicate certain
conditions, e.g cataracts, retinoblastomas.
Examining the retinas
To examine the right eye, hold the ophthalmoscope in your right hand and visa versa. Stand
at arms length from the patient and gently rest your other hand on the patient’s forehead
with your thumb on their eyebrow (warn them before doing this).
Locate the optic disc and assess its colour, margins and cup to disc ratio
Follow the major vessels and assess their tortuosity and dilation
Examine the peripheral retina by asking the patient to look up, down, right and left.
Look for the presence of exudates, haemorrhages, pigmentation
Locate the fovea (macula) by asking the patient to look directly at the light
46
Finally explain to the patient that you have finished and
thank them for their cooperation.
47
How to Record your Clinical Notes
The case notes, sometimes called case records, are the written record of a patient’s medical
condition. When you assess a patient the notes that you write are called a ‘patient clerking’. In
these notes you should include your initial findings, proposed investigations and the plan of
management for your patient’s condition. (Table 1) All entries in the case notes must be
clearly timed and dated, written in black pen and signed at the end. This signature should be
legible and include your status (e.g. 3rd year medical student). Entries allow information to
be recorded and shared by all staff, not only during this episode of illness, but over time.
When a patient presents in the future any findings can be compared with those found at any
earlier presentation. Notes must therefore be accurate, legible and clearly signed.
Information provided in the case notes
• History and examination findings
• Investigations and results
• The management plan
• Assessments of other health professionals, e.g. dieticians, speech and language therapists
• Information and education provided to patients and their relatives
• Correspondence about the patient
• The patient’s progress
• Advance directives or ‘living will’
• Contact details about next of kin.
Table 1: Information found in Clinical Notes
You may write notes while talking to the patient but do not let this interrupt the flow of your
discussion, and maintain as much eye contact as possible. Active listening is difficult if you
are writing, so try to make brief notes at the time and write the full history after you have left
the patient. Write up the physical findings when you have completed the examination and
not as you proceed. Only record objective findings and never make judgemental or pejorative
comments. Not only is this unprofessional, but also remember that patients or their lawyer
may subsequently read their notes.
As structured proformas for recording the initial history and examination findings are used
increasingly in many hospitals, it is not possible to record every detail of the history and
examination in every patient. Only record negative findings if they are relevant; for instance,
if a patient presents with chest pain, the negative details of the cardiovascular enquiry are
important but negative responses to the nervous system enquiry may be condensed to ‘nil’.
You may use abbreviations but they should not be obscure or ambiguous. Widely recognized
ones are included in the case example and can also be found at:
www.pcps.ucl.ac.uk/commskills/student_handbook/abbreviations.htm.

48
Diagrams should be used to show the site and size of superficial injuries, rashes and ulcers, to
illustrate any abnormalities in the chest and abdomen and to show areas of sensory loss. (fig
5)
There are also accepted ways to document heart sounds (see Clinical Examination, Epstein et
al. Page 159-160), muscle strength (see Clinical Examination, Epstein et al. Page 352) and
conscious level (see Clinical Examination, Epstein et al. Page 372)
Completing the clerking
To complete the ‘clerking’ summarise the history (both the important positive and negative
findings) in two sentences. Then provide a diagnosis, a differential diagnosis, a problem list,
an investigation list, and a management plan. Finally, it is important to spend some time
reflecting on how you felt the session went. Points to consider include one of these questions:
What really happened?
What was interesting or worrying?
What can you conclude generally about the situation?
What did the patient say and think? (if appropriate)
What did you say and think? (if appropriate)
What was done well?
What should be done differently next time?
What did you learn about yourself?
Identify future learning needs?
Presenting your Clinical Notes
The purpose of the oral presentation of the patient clerking is to provide other clinicians with
patient information. This should be done in a way that tells the patient’s story in a clear,
logical and systematic way. It needs to be focused and brief, but also needs to include all
relevant details of the patient and their illness.
This is a difficult skill to master and the first time you are asked to present a patient to a
medical team you will find this quite stressful. During the IOM, listen to an experienced
clinician present a patient (probably on a ward round) and try to identify what constitutes a
concise, effective presentation.
A useful resource:
Please visit the Clinical Skills Guidelines and Teaching Materials site, where you
will find Guidelines, Lecture Slides, Videos and Revision tools.
http://www.ucl.ac.uk/medicalschool/current-students/course-information/csg-tm/
49
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
Measuring Blood Pressure
Measurement of blood pressure is one of the most often performed examinations. It is
performed using a sphygmomanometer and stethoscope. Previously mercury
sphygmomanometers were used; current practice is to use aneroid and digital models.
Before you start consider....
Why do we measure blood pressure?
What are we measuring?
What are we listening for?
What measurement is considered “too high”?
What are the pieces of equipment called?
Introduction
W- Wash your hands.
I- Introduce yourself to the patient
P- Permission. Explain that you wish to measure their blood pressure and obtain
consent for the examination.
E- Expose the necessary parts of the patient. Sleeve rolled up.
R- Reposition the patient. Blood pressure is usually measured seated. The
sphygmomanometer and the supported arm should be at the same level as the heart.
Taking the Measurement
1. Choose the correct cuff size for the patient (in normal adults this is 30-35cm in
length and 12cm wide).
2. Position cuff in correct position with tube pointing downwards over brachial
artery. There is usually a mark or arrow that should be lined up with the brachial
artery.
3. Close valve.
4. Palpate radial artery and then inflate cuff until pulse disappears. This is a
i. rough measure of systolic pressure.
5. Deflate cuff.
6. Locate brachial pulse and position stethoscope over pulse.
7. Re-inflate cuff to 20-30mmHg above previous reading obtained by palpation.
8. Deflate cuff slowly until regular heart sounds (Korotkoff sounds) can be heard.
This is the systolic pressure.
9. Continue to deflate no faster than 1-2 mm/Hg per second. Record the point when
the sounds disappear. This is the diastolic pressure.
10. Deflate cuff fully and then remove cuff from arm.
11. Thank the patient and help to dress again if appropriate.

50
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
Performing urinalysis
Urinalysis means analysis of urine. This is a very commonly ordered test which is performed in many
clinical settings. Urinalysis is a simple test that can provide important clinical information, has a quick
turn-around time, and is also cost effective.
Before you start consider…
Why do we perform urinalysis?
What are we measuring or looking for?
What results are considered abnormal?
What are the pieces of equipment called?
Urinalysis is very a useful test in the diagnosis of and screening for many diseases and conditions.
Results of a urinalysis may be helpful in:
diagnosing urinary tract infections (UTIs),
diagnosing kidney stones,
screening for and evaluating kidney diseases, and
diagnosing and monitoring the progression of diabetes mellitus and hypertension
Urinalysis Procedure – collecting the specimen
The urinalysis test first involves the collection of urine sample in a specimen cup. The proper
collection of a sample is important in order to avoid contamination of urine. The collection
technique is different for men and women. For men, the opening of the urethra (tip of the
penis) should be wiped clean with a cleansing wipe before collection is begun.
In women, the area around the urethra also needs to be wiped clean with a cleansing wipe.
The woman then spreads the labia of the external genitalia and wipes from front to back.
After the urethra is properly cleaned, the collection may begin by discarding the initial
stream of urine into the toilet.
Then, 10-15 millilitres (ml) of urine may be collected in the provided sterile specimen cup
by directly urinating into the cup.
Once an adequate amount is collected, then the remaining urine should be voided in the
toilet.
This technique is called the mid-stream clean catch urine sample collection.
Other collection methods may be necessary depending on the specific situation. Frequently,
hospitalized patients may have a urinary catheter. Here the urine is collected from the
collection bag into the sterile cup. Samples can be collected from babies and toddlers who are
not yet toilet trained by attaching a small collection bag with a bandage-type adhesive to the
external genital region.
The collected urine sample should be analysed soon (within 1-2 hours) after collection. If this
is not possible, then the sample may be refrigerated.

51
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
A dipstick test is usually performed on the urine specimen to check for:
o glucose
o ketones
o blood (detected as haemoglobin in the urine),
o leukocyte esterase (suggests white blood cell in the urine),
o nitrites (evidence of any bacteria in the urine),
o bilirubin, and
o Urobilinogen in the urine (related to an elevated bilirubin level, denoting possible liver
disease or red blood cell breakdown in the body).
Available tests include the likes of Multistix® (suitable for screening for glycosuria only),
Micral-Test II® or Microalbustix® (detect microalbuminuria) and the more commonly used
multiple combination strips - e.g., five tests on each strip (detects blood, ketones, glucose, pH
and protein), or seven tests on each strip (tests for blood, ketones, glucose, pH, bilirubin,
urobilinogen and protein).
The test strip is a chemical reagent strip. It consists of a ribbon made of plastic with pads
containing chemicals that react with the compounds present in urine producing a
characteristic colour. Depending on the stick being used, it can provide analysis of pH,
protein, glucose, ketones, blood, nitrite, presence of WBCs, bile and urbilinogen. The strip is
dipped in the urine and colour changes are measured after a set period, according to the
manufacturer’s instructions. The colours appearing on the dipstick are compared with a chart
provided. Strips may be qualitative strips that only determine if the sample is positive or
negative, or there are semi-quantitative ones that in addition to providing a positive or
negative reaction also provide an estimation of a quantitative result, in the latter the colour
reactions are approximately proportional to the concentration of the substance being tested for
in the sample.
Semi-quantitative values are usually reported as: trace, 1+, 2+, 3+ and 4+.
Visual inspection
Macroscopic analysis of the urine is done by inspecting the physical appearance of the urine.
Normal urine is light yellow and clear. Macroscopic urinalysis notes the amount, color, and
clarity of the urine as well as any other visible characteristics of the urine such as the presence
of blood or blood clots, precipitates, or sediments
Obvious abnormalities in colour, clarity, and cloudiness may suggest conditions such
as:
o dehydration,
o infection,
o liver disease, or
o Muscle breakdown (rhabdomyolysis).

52
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
Common Causes of Urine Discolouration
Colour
Pathological causes
Food and drug causes
Brown
Bile pigments, myoglobin
Levodopa, metronidazole, nitrofurantoin,
some antimalarial agents
Brownish-
black
Bile pigments, melanin,
methaemoglobin
Levodopa, methyldopa, senna
Green or
blue
Pseudomonas urinary tract infection
(UTI)
Amitriptyline, IV cimetidine, IV
promethazine
Orange
Bile pigments
Phenothiazines, rifampicin,
hydroxocobalamin
Red
Haematuria, haemoglobinuria,
myoglobinuria, porphyria
Beets, blackberries, rhubarb, rifampicin
Yellow
Concentrated urine (orange to gold
in dehydration)
Carrots
Turbidity
Cloudy urine may be due to a variety of normal and abnormal processes including
contamination with vaginal mucus or epithelial cells, pyuria secondary to infection or
hyperuricosuria secondary to a diet high in purine-rich foods.
Odour
In concentrated specimens this can be strong but does not necessarily imply infection.
Patients with diabetic ketoacidosis produce urine that may have a sweet or fruity odour. Other
causes of abnormal odours are gastrointestinal-bladder fistulae (a faecal smell), medications
(e.g., vitamin B6), and diet (e.g., asparagus).
Testing the urine
1) Wash hands, put on gloves
2) Look at the bottle – confirm the patient’s identity and the date of the specimen. Verify when
the sample was taken and, if there has been a delay, that it has been refrigerated.
3) Visually inspect the sample noting the colour and clarity of the sample. Note also the presence
of odour when the sample is opened
4) Check the dipsticks: Are they in-date? Check silica gel crystals are present in the container to
ensure the sticks have been kept dry. Note the type of strips in use and what they test for. We
generally use Siemens Multistix 8SG:

53
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
5) Dip the sample – immerse the stick fully in the urine sample ensuring all the pads are covered
and then remove it immediately. Shake off the excess urine, and dab it on a paper towel.
6) Wait the recommended amount of time and note down the results by comparing the reaction
observed with the colour chart on the tube. Read each pad at the time shown on the container,
starting with the shortest time.
54
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
7) Comment on any irregularities present and say what you would do to test them further.
8) Put the lid back on, put the sample back. Take gloves off (yellow bin) and wash your hands.
9) Document the result of the dipstick analysis and any further management that is required in
the patient’s notes.
An improper technique can produce false results, for example, leukocytes and erythrocytes
precipitate at the bottom of the container and may not be detected if the sample is not properly
mixed, and in the same way, if an excess of urine remains on the strip after it has been
removed from the test sample, may cause the reagents to leak from the pads onto adjacent
pads resulting in mixing and distortion of the colours. To ensure that this does not occur, it is
recommended the edges of the strip are dried on absorbent paper.
Interpreting results
Haematuria
A positive test indicates either haematuria, haemoglobinuria or myoglobinuria.
Dipstick tests for the presence of haemoglobin with the degree of colour change directly
related to amount present.
False positive readings are most often due to contamination with menstrual blood; they are
also seen with dehydration which concentrates the number of RBCs produced, and exercise.
Dipstick testing for haematuria is at best a screening tool which needs the support of
microscopy to make a definitive diagnosis
Proteinuria.
Healthy adults normally excrete 80-150 mg protein in urine daily. Normal urinary proteins
include serum globulins, albumin, and proteins secreted by the nephron.
Proteinuria is defined as albumin: creatinine ratio >30 mg/mmol or albumin concentration >200
mg/L. Clinical proteinuria is indicated at greater than 0.5 g of protein per day (greater or equal to
250 mg/L on a test strip).
Detectible proteinuria may be the first sign of renovascular, glomerular or tubulo-interstitial renal
disease. Alternatively, it may be caused by overflow of abnormal proteins in diseases such as
multiple myeloma.
Persistent significant proteinuria detected by dipstick requires further assessment with 24-hour
urinary protein excretion, urinary protein: creatinine ratio, and assessment of renal function.
Glucose
Nearly all glucose filtered by the glomeruli is reabsorbed in the proximal tubules and only
undetectable amounts appear in urine in healthy patients. Above the renal threshold (10
mmol/L) glucose will appear in urine.
Useful screen for diabetes mellitus.
False positive results: seen when high levels of ketones are present. Also seen in patients
taking levodopa.
Ketones
Ketones are not normally found in urine.
A positive test is associated with uncontrolled diabetes, pregnancy without diabetes,
carbohydrate-free diets and starvation.
55
Originally by Kate Chatten, Mary Howe, Gillian Marks and Tom Smith. Edited and
updated by Henry Tufton, Dr Alison Sturrock and Dr Deborah Gill. Further updates Dr
Jessica Bilaney, Dr Beth Walker, Dr Laura-Jane Smith and Mr David Gamble. Dr Helen
Nolan 2015 ©ACME 2015
Bilirubin and urobilinogen
Unconjugated bilirubin is water-insoluble and not normally present in the urine.
Conjugated bilirubin only appears in urine in the presence of liver disease or obstruction of the
bile ducts.
A small amount of urobilinogen is normally found in urine
Nitrites
This test relies on the breakdown of urinary nitrates to nitrites, which are not found in normal
urine.
Many Gram-negative and some Gram-positive bacteria are capable of producing this reaction
and a positive test suggests their presence in significant numbers (i.e. more than 10,000 per
ml). A negative result does not rule out a UTI.
The reagent is highly sensitive to air exposure, which may cause a false positive response.
False negative results may be seen where:
Bladder incubation time is shortened (less than four hours).
There is absence of dietary nitrate.
There is presence of nitrate reductase-negative organisms (e.g., some mycobacteria
strains).
Leukocyte esterase
This relies on the reaction of leukocyte esterase produced by neutrophils and a positive result
suggests pyuria associated with UTI.
False positive results may be caused by contamination with vaginal discharge
